
Abstract
Purpose:
The purpose of the study was to answer the following questions. What was functional results of pediatric patients receiving a short stem allograft-prosthesis composite of the proximal femur? What was complication rate and revision-free implant survival? Was it possible to preserve the bone stock of the proximal femur in pediatric patients?
Methods:
We reviewed 10 pediatric patients treated with proximal femur resection for a primary bone tumor and reconstruction with short stem allograft-prosthesis composite, with at least 24 months follow-up. The median age was 9 years (4–13) at surgery. The mean resection length was 15 cm (6–29). In six cases, fixation was performed with a short plate positioned under the great trochanter while in four cases a long plate extended over the great trochanter was employed.
Results:
Nine complications that required surgical revision were assessed in six patients (one wound dehiscence, two nonunions, two fractures, one acetabular wear, three hypometria), while allograft-prosthesis composite removal was required in three patients. The revision-free survival was 57% (95% confidence interval 33%–100%) at 5 and 10 years. The graft removal-free survival was 75% (95% confidence interval 50%–100%) at 5 and 10 years. The mean Musculo-Skeletal Tumor Society Score was 28 (20–30).
Conclusions:
Allograft-prosthesis composites with short stem and compression plate represents an effective reconstructive option after proximal femur resection for primary bone tumors in growing patients, preserving bone stock. The use of a compression plate extended over the greater trochanter seemed to reduce failure rate.
Introduction
Proximal femur is the fourth most common site of occurrence of primary bone tumors in children, following distal femur, proximal tibia, and proximal humerus.1,2 Since the introduction of well-established chemo- and radiation therapy protocols, limb salvage surgery has been accepted as standard of treatment for malignant bone tumors.3,4 In adults and skeletally mature patients, allograft-prosthesis composites (APCs) and modular prostheses are commonly used for reconstruction.5 –10 However, osteoarticular replacement of the proximal femur in growing children poses several challenges. Cementless prosthetic stem fixation in an immature bone is at risk for stress shielding, whereas with cemented implants, there are concerns of bone loss during subsequent revision surgery. The progressive growth in size of the femoral head stimulates the consensual growth in width of the acetabular cavity through the triradiate cartilage. Femoral head replacement with a prosthetic implant impairs acetabular growth and, due to the plasticity of the immature bone, frequent progressive subluxation can be observed. Tendinous reconstructions of the gluteal muscles and iliopsoas are crucial for functional recovery after proximal femur resections and this is difficult to obtain with prosthetic implants, even when additional synthetic meshes are employed. Moreover, proximal femur reconstruction in growing children should consider high functional expectations of pediatric population and long-term survival of patients with eventual requirement of subsequent revisions. For this reason, bone stock preservation appears as an important objective in pediatric reconstructions.
Several reconstructive options have been described after proximal femur resection in children, such as massive osteoarticular allografts,11,12 hip arthrodesis, 11 recycled autograft-prosthesis composites,13,14 combination between massive allograft and vascularized growing fibula autograft, 15 modular, custom made and lengthening prosthesis,1,2,16 –19 and APCs.2,9,10
The supposed benefit of APC reconstruction over endoprosthesis include biological attachment of tendons, improving stability, function recovery and gait, restoration of bone stock, and load-sharing properties of the allograft if union occurs; in particular, restoration of bone stock is very beneficial in young patients who are at high risk of requiring further surgeries.5 –7
APCs have been described with two different assembling: long stem prosthesis cemented into the allograft, by-passing the osteotomy line, achieving fixation in healthy bone with or without cement; short stem prosthesis, cemented into the allograft, using compression plate fixation to the femoral diaphysis.5 –10 Long stems theoretically decrease the risk of allograft fractures, but on the other hand, transfer loads directly to the femoral shaft, leading to an increasing risk of stress-shielding in pediatric host bone.20,21 On contrary, short stem APC is indicated in proximal femur pediatric reconstructions for the following reasons: the immature bone of healthy femoral diaphysis is not violated by an intramedullary stem, avoiding stress-shielding and facilitating subsequent revisions or lengthening procedures, and proximal femur bone stock is preserved by allograft replacement providing a biologic scaffold for future revisions. Furthermore, in growing patients, the residual femoral shaft dimension does not always allow the use of long stems. In this population, an APC using compression plates and short stem prosthesis minimally affects the host–donor osteotomy site, allowing physiologic load transfer once union has been reached by periosteal and endosteal callus formation.10,22 To our knowledge, this is the first study reporting long-term outcome of reconstruction with short stem APC after proximal femur resection in pediatric patients. The purpose of the study was to answer the following questions. (a) What was functional results of pediatric patients receiving a short stem APC of the proximal femur? (b) What was complication rate and revision-free implant survival? (c) Was it possible to preserve the bone stock of the proximal femur in pediatric patients?
Materials and methods
All skeletally immature patients treated with intraarticular resection of proximal femur for a primary bone tumor and reconstruction with short stem APC in our institution between 2001 and 2020 were reviewed. Eleven patients were identified, but one of them had less than 24 months follow-up and he was excluded, leaving 10 patients for the final analysis; their characteristics are summarized in Table 1.
Patients’ Characteristics and Complications.
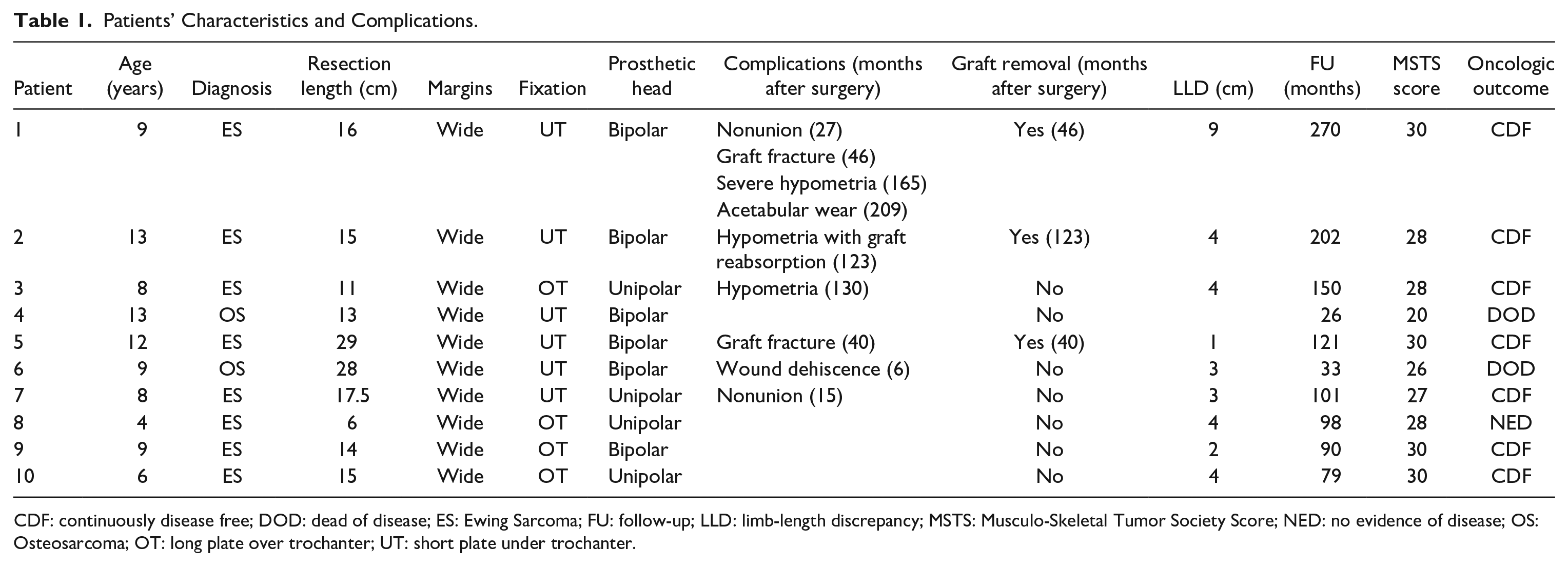
CDF: continuously disease free; DOD: dead of disease; ES: Ewing Sarcoma; FU: follow-up; LLD: limb-length discrepancy; MSTS: Musculo-Skeletal Tumor Society Score; NED: no evidence of disease; OS: Osteosarcoma; OT: long plate over trochanter; UT: short plate under trochanter.
There were nine males and one female with a median age of 9 years (4–13) at surgery. The diagnosis was a malignant bone tumor in all cases; eight Ewing’s sarcoma and two high-grade osteosarcoma. At diagnosis, one patient had pathologic fracture that healed spontaneously during preoperative chemotherapy. According to MSTS (Musculo-Skeletal Tumor Society Score) Staging System, 23 at diagnosis one tumor was Stage IIA, five were IIB, and four were IIIB. All patients received pre- and postoperative chemotherapy according to the appropriate protocol for the tumor type, while none underwent radiation therapy. All patients underwent intraarticular resection of proximal femur. In one osteosarcoma with a subtotal involvement of the femur, the resection was extended to the distal femur growth plate. On histological examination of the resected tumor, surgical margins resulted wide in all cases.
In nine patients, the short stem APC was used as primary reconstruction after intraarticular resection of proximal femur for a malignancy, while in one case it was used as salvage procedure after failure of APC with resurfacing prosthesis in a Ewing’s sarcoma, who had a femoral neck fracture of the graft at 3 years from index surgery. Our policy is to use a short stem APC with compression plate fixation in skeletally immature patients undergoing intra-articular proximal femur resection for a primary bone tumor. In this group of patients, we prefer to employ a short stem APC to restore the bone stock once the allograft-host bone union is achieved, in addition to the other benefits of proximal femur composites reconstructions, such as biological attachment of abductors and ilio-psoas tendons, improving hip stability, function, and gait. Furthermore, short stem APC preserve the integrity of residual distal femoral shaft, avoiding the risk of stress-shielding with stem fixation in an immature bone.
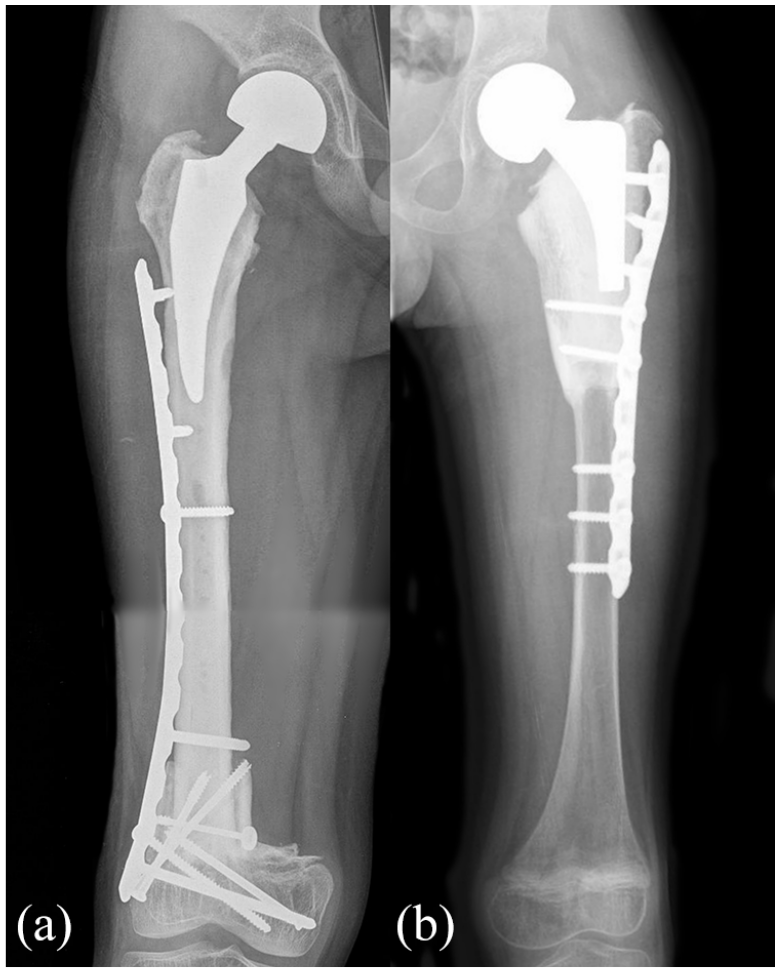
All surgeries were performed through a lateral approach, with the patient in supine position. The median length of proximal femur resection was 15 cm (6–29). We used nonirradiated proximal femur allografts harvested under sterile conditions, stored at −80°C in our center bone bank and selected according to the diameter of the femoral shaft, to achieve the best anatomic match. After en bloc resection of the tumor, the osteoarticular allograft was thawed in a warm antibiotic solution using rifampicin 250 mg per liter of saline solution, sectioned to the proper length and shaped to receive the femoral stem. In three patients, the length of reconstruction was less than 1/3 of the native femoral length, in five patients, between 1/3 and 2/3, while in two patients was more than 2/3. A step cut osteotomy was performed in five allografts while a transverse osteotomy in the other five. A short stem was cemented inside the graft in all cases, paying attention not to cross the osteotomy with cement and stem, and finally the composite prosthesis was fixed to the host femur with a locking compression plate. In six cases, fixation was performed with a short plate positioned under the great trochanter while, in four cases, a long plate extended over the great trochanter was employed (Figure 1). In none of our patients an acetabular cup was implanted. In six patients, a bipolar head was used, with a diameter ranging between 39 and 46 mm, while in four patients a ceramic unipolar head was used with a diameter ranging between 32 and 40 mm (Figure 2). The choice between unipolar and bipolar head was done according to the native acetabular width and availability of size of bipolar cups. Finally, the abductors and the psoas tendons were sutured to the graft by nonabsorbable sutures.

This figure shows the two types of APCs with short stem assembling used in this study. (a) Fixation performed with a short plate positioned under the great trochanter. (b) Fixation performed with a long plate extended over the great trochanter.
This figure shows the two types of prosthesis heads used in proximal femur APCs. (a) Bipolar head. (b) Unipolar head.
All patients received perioperative antibiotic prophylaxis with intravenous vancomycin (1 g every 12 h) combined with tobramicin (1 mg/kg every 8 h) until 2010 and with piperacillin and tazobactam (4.5 g every 8 h) from 2010 to now, according to our institution’s protocol, which was continued until drainages removal. After surgery, all patients were mobilized with two crutches wearing an ischial weight-bearing brace, allowing controlled passive movements of the knee and ankle. Partial weight-bearing was allowed after initial evidence of callus formation on X-rays; full weight-bearing was given after evidence of osteotomy healing. We defined graft-host bone union as the evidence on X-rays of a bridging callus around the osteotomy in at least three cortices.
All patients were periodically reviewed according to oncological follow-up, undergoing clinical and radiological examination. The functional outcome was evaluated using MSTS score system. 24 In all patients, the union of the graft was radiographically assessed, and complications and failures were recorded during follow-up. Survival of the reconstruction was determined according to Kaplan-Meier method, including revision surgery for any complications and removal of the APC as endpoints indicating failure. Kaplan-Meier curves and survival proportions were computed using R version 4.1.2 via the package Survival version 3.5. A log-rank test was used to compare the survival distributions. Significance was set at p < 0.05.
The present study was approved by our local institutional review board.
Results
At last clinical control, at median follow-up of 100 months (26–270), seven patients were continuously disease-free (CDF, 70%). Two patients with high-grade osteosarcoma developed lung metastasis and died after 33 and 26 months, respectively (DOD, 20%). Another patient with diagnosis of Ewing’s sarcoma developed bone metastasis in the contralateral proximal tibia 29 months after primary surgery and was treated with proximal tibia resection, prosthetic reconstruction and chemotherapy, remaining disease free at last follow 68 months later (no evidence of disease, 10%). The overall survival of the patients, with death as endpoint, was 80% (95% confidence interval [CI] 59–100) at 5 and 10 years.
During follow-up, nine complications that required surgical revision were assessed in six patients (60%) after a median of 34 months (6–130) from primary surgery, while APC removal was required in three patients (30%) after a median of 46 months (40–123).
One patient had aseptic wound dehiscence 6 months after index surgery, treated successfully with surgical debridement.
There were three nonunions but only two (20%) were surgically treated. One patient had nonunion of the graft 27 months after primary surgery, then healed after autologous iliac crest graft augmentation and new plate fixation. Another patient had nonunion 15 months after index surgery, initially treated with autologous graft augmentation and then healed after augmentation with autologous vascularized fibula graft 12 months after first surgical revision. Last, one patient with osteosarcoma had a nonunion 18 months after primary surgery but it was not treated due to diffuse metastatic disease. Interestingly, all the patients who developed nonunion had a short fixation plate, while none of the patients with long fixation plate had nonunion. Moreover, two of them did not have a step cut osteotomy. The other patients achieved union between graft and host bone after a median of 8 months (6–21).
There were two fractures (20%), both traumatic, occurred, respectively, 40 and 46 months after primary surgery. The first one was treated with APC removal and reconstruction with a new APC with smooth long-stem cementless prosthesis fixed with long plate; the other one underwent APC removal and reconstruction with a modular proximal femur endoprosthesis with cemented stem. Both patients had short plate fixation.
In one patient, a cementless acetabular cup was implanted 17 years after primary surgery due to a symptomatic superolateral acetabular wear.
A limb-length discrepancy (LLD) ranging from 1 to 9 cm was assessed in nine patients (90%) at last clinical control. In one patient, a 9 cm hypometria (with both femoral and tibial shortening) was treated with a tibial lengthening by external fixation reaching a residual 1.5 cm shortening; in two patients both with 4 cm hypometria, the LLD was managed with APC removal due to partial resorption of the graft and reconstruction with modular endoprosthesis in one, and with femoral lengthening using a retrograde expandable nail in the other. In other patients, mild LLD was conservatively managed with an orthosis.
In both patients with APC removal and revision with a modular endoprosthesis, part of the allograft bone was retained (Figure 3). No deep infections nor dislocations were observed.
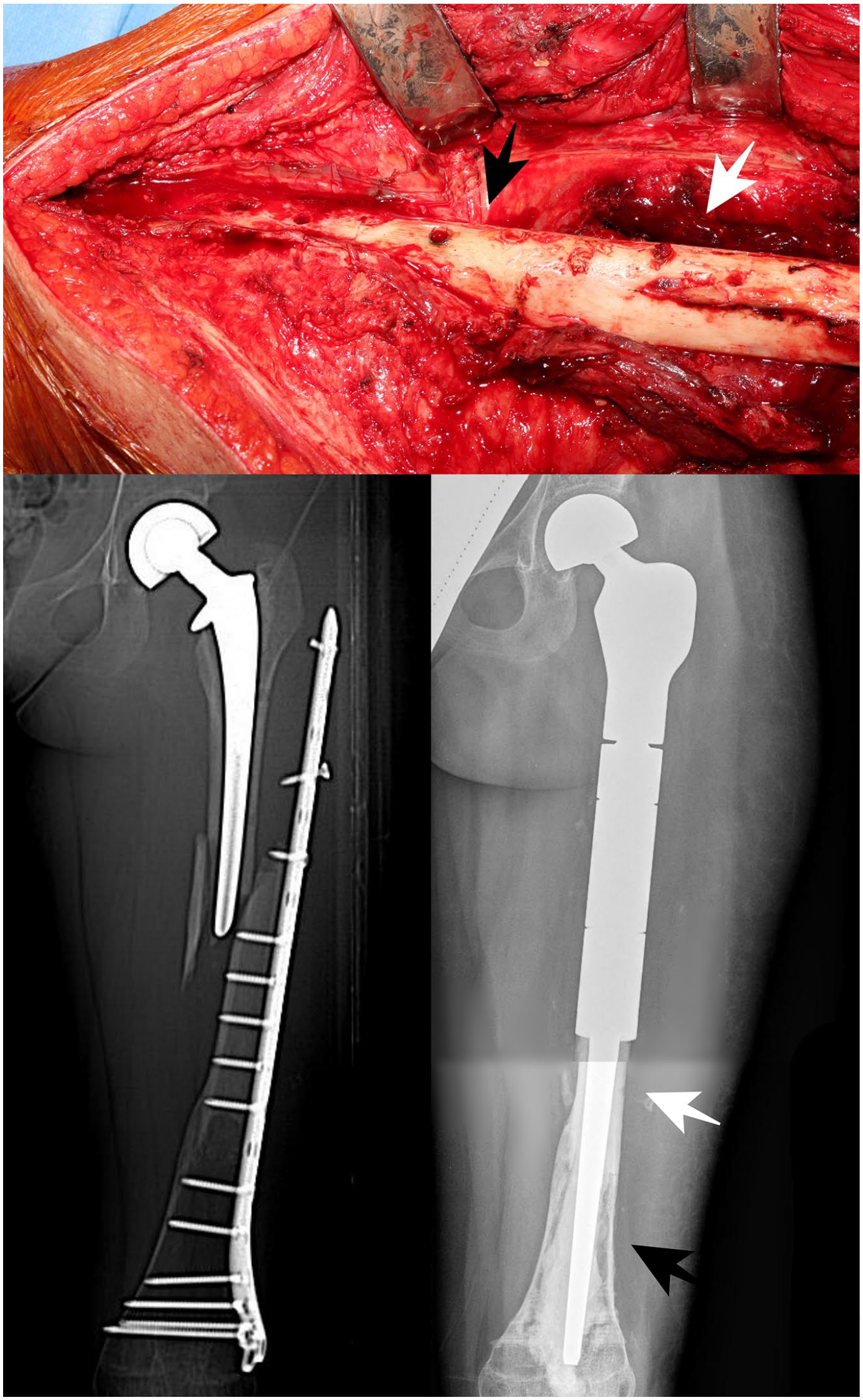
This figure shows the host bone (black arrow) and the allograft bone partially retained (white arrow) after APC removal and revision with a modular endoprosthesis in a patient who had a traumatic fracture.
At last follow-up, the median MSTS score was 28 (20–30), but considering only living patients at last clinical control, the mean MSTS score was 29 (27–30). In these population, function and walking ability ranged between 4 and 5 points: emotional acceptance, pain, and supports scored 5 points in all patients, while gait ranged between 3 and 5 points.
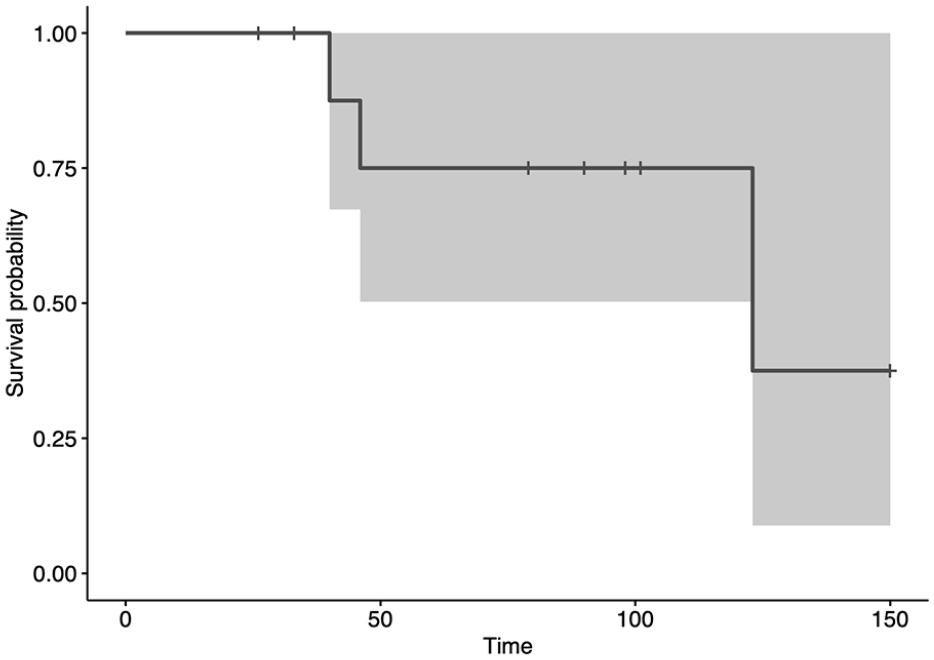
The revision-free survival of the reconstructions, with failure requiring revision surgery as endpoint, was 57% (95% CI 33%–100%) at 5 and 10 years (Figure 4). The overall survival of the reconstructions, with removal of APC as endpoint, was 75% (95% CI 50%–100%) at 5 and 10 years (Figure 5).
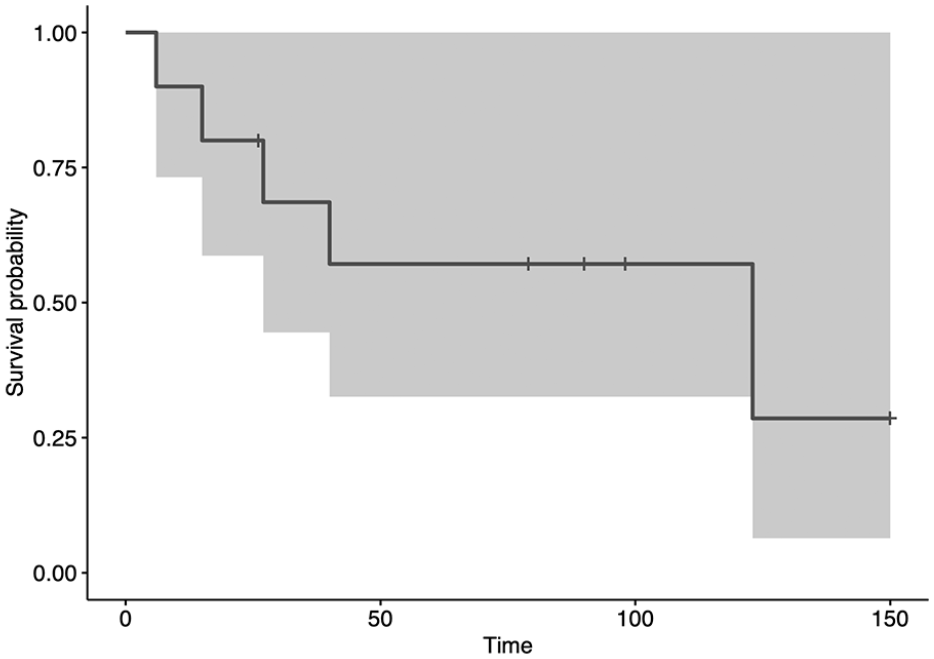
This graph shows revision-free survival, with surgical revision for any complication as the endpoint. The survival was 57% (95% CI 33%–100%) at 5 and 10 years. The gray area represents the CIs.
This graph shows graft removal-free survival, with graft removal for any complication as the endpoint. The survival was 75% (95% CI 50%–100%) at 5 and 10 years. The gray area represents the CIs.
Discussion
The ideal reconstruction following proximal femur bone tumor resection in skeletally immature patient remains a matter of debate. The challenge in this population is to restore a functional hip with a long-term durable reconstruction. However, in view of the high risk of further revision surgeries, bone stock preservation seems a desirable option. Indeed, compared with adults, proximal femur reconstructions in pediatric population showed a significant higher failure rate. 2
Several reconstructive options have been described in growing patients, such as massive osteoarticular allografts,11,12 recycled autograft-prosthesis composites,13,14 combination between massive allograft and vascularized growing fibula autograft, 15 expandable prosthesis,1,2,16 –18 and APCs.2,9,10
Proximal femoral massive allografts allow soft tissue attachment and bone stock restoration once achieved bone union, but they are burdened by a high risk of fracture and failure.11,12 Recycled APCs, both frozen or irradiated, represent an attractive option with several advantages such as low cost, precise matching, no risk of transmission of infective disease, preservation of bone stock, and biologic soft tissue attachment. Excellent functional results and graft survival of 50%–85% at 10 years were reported with recycled APCs,13,14 but the major drawback of this technique is related to the limited histological examination of chemo-induced necrosis and surgical margins. 25 Moreover, only few cases of pediatric reconstruction with this method are described in literature.13,14 Manfrini et al. 15 in 1997 replaced the proximal femur in a 4-year-old child after resection of an Ewing’s sarcoma with an autogenous fibula graft placed inside a modeled massive allograft, using the proximal fibular physis to reproduce the femoral head. In spite of providing potential growth and remodeling of the fibula head, this biologic solution is technically very demanding, and no case series are reported in literature so far.
Currently, expandable prosthesis and APCs represent the most widely used reconstructions after proximal femur sarcoma resection in skeletally immature patients.1,2,9,10,16 –18 Expandable endoprosthesis can be used to avoid leg-length discrepancies, even though proximal femur contributes for only 30% of the total femoral growth.8,18 However, lengthening prostheses can be quite invasive in young children, requiring a minimum femoral resection length and sufficient residual distal femur for fixation and they are burdened by a high risk of loosening and structural failure.1,2,17,18 Belthur et al., 1 in a series of nine children with proximal femur expandable prosthesis, reported a high complication rate in surviving patients. In their series, 1 two patients required three revisions for loosening of acetabular cup, concluding that bipolar or unipolar head is recommended. Groundland et al., 2 in a systematic review of limb-salvage reconstruction in pediatric patients, observed that proximal femur endoprosthesis had the highest failure rate (55%) compared to other prosthetic reconstruction in lower limb; the most frequent failure modes were aseptic loosening and infection, both reaching 13.8%.
Proximal femur APCs have many advantages over endoprosthesis such as improved function and gait, restoration of bone stock, biological attachment of tendons, and load-sharing properties of the allograft once achieved union.5 –7 Muscolo et al. 10 reported a series of proximal femur APCs with short stem and compression plate. This approach is very suitable in skeletally immature patients, maintaining unviolated the host distal femur and minimally affecting the osteotomy site allowing load sharing once union has been achieved.10,22 Moreover, this method can be adapted to proximal femur reconstruction in children with short residual femur bone length and narrow femoral canal. Many authors reported their experience with APC reconstruction of proximal femur after bone tumor resection in adults,5 –9 most of them using long-stem prosthesis, but only few cases of APC reconstruction of proximal femur in skeletally immature patients are described in literature.2,10,26 Groundland et al., 2 in the above-mentioned systematic review, considering 14 pediatric patients, reported a failure rate of 28.5% with an infection rate of 14.3% and an incidence of loosening and structural failure both of 7.1%. The overall failure rate of proximal femur APCs was lower than metallic endoprosthesis (28.5% versus 55%), and proximal femur APCs in children had the highest functional results (86.8%) among APC reconstructions of lower limb. 2 In our series, surgical revision for complication was required in six patients, leading to an APC removal in three patients. The revision-free survival of the reconstructions, with failure requiring revision surgery as endpoint, was 57% at 5 and 10 years while the overall survival of the reconstructions, with removal of APC as endpoint, was 75% at 5 and 10 years. All complications, except one, occurred within the first 40 months after index surgery (Figure 4) and 75% of the patients retained the APC at 10 years from primary surgery (Figure 5). Nonunions and fractures were the observed complications in our series, while infections or dislocations did not occur. All patients who developed nonunion or fracture had a short fixation plate, while none of the patients with long fixation plate had mechanical complications. Muscolo et al. 10 reported a higher failure-free survival in patients with a plate spanning at least half of the femoral stem. We observed this measure in all our patients, but when a long plate extending over the great trochanter was used, no failures occurred.
One of the major advantages of APCs over modular prosthesis is the restoration of bone stock once union is achieved, in particular in children who are at high risk of requiring further revision surgeries. Wilke et al., 27 in a series of adult patients with proximal femur APC revision for an aseptic cause, retained a part or the entire allograft only in 26% of patients claiming that the aim of preserving bone stock should not be a justification for their use. Differently, considering only skeletally immature patients, we partially retained allograft bone in two of the three patients (66%) that required APC removal. As known, even after several years, allograft internal repair by creeping substitution is incomplete, even though the proportion is higher in pediatric patients. 22 Nevertheless, although partially repaired, the allograft is still suitable to maintain bone stock in sight of further surgeries. Moreover, none of our patients had host bone reabsorption, as reported by some authors using long-stem APCs,8,28 that could lead to an additional host bone sacrifice in revision surgery.
Another interesting issue to consider in proximal femur replacement in skeletally immature patients is the progressive acetabular wear. Proximal-lateral migration of the femoral head has been observed in children after hemiarthroplasty following tumor resection29,30 leading to a revision rate between 20% and more than 80%. This acetabular dysplasia has been related to three factors: increased potential for acetabular remodeling, particularly in young children far to closure of the triradiate cartilage; increased pressure and wear of the acetabular dome by the prosthetic head; the muscular imbalance due to the weakening of the hip abductors, which are no longer able to contrast the intact hip adductor muscles. 29 Indeed, a more severe migration of the femoral head was seen in children younger than 11 years and in those with proximal femur than total femur replacement.29,30 According to these findings, we observed proximal-lateral migration of the prosthetic head in all patients with resection no longer than 2/3 of the native femoral length, and more evident dysplasia in patients treated before 9 years of age. Although frequently observed in our cases, only one patient (10%) developed a symptomatic proximal-lateral acetabular wear that required a cementless acetabular cup implant 17 years after primary surgery, while the other patients remained asymptomatic. The prevention of acetabular dysplasia in skeletally immature patients with hemiarthroplasty after proximal femur resection is still matter of debate. Authors proposed several solutions such as the use of more varus prosthesis with increased offset, 29 the routine reaming of the acetabulum to deepen the cup, 18 and to keep the affected limb slightly shorter than the contralateral to maintain the hip in relative abduction. 30 The last two solutions in our opinion are not routinely recommended; the first one represents a quite invasive solution in a growing acetabulum, while the second will lead to an increased LLD. In our series, LLD ranging from 1 to 9 cm was assessed in nine patients (90%), but only in three (30%) it was surgically managed while, in the others, mild LLD was managed with an orthosis. These findings are in accordance with the skeletal immaturity of our patients, and with the contribution of less than 30% of the proximal femur growth plates to the longitudinal growth of the femur.
This study certainly present limitations: first, this is a retrospective observational study of patients treated over a 20 years period of time. However, patients were treated at a single institution by the same orthopedic team; second, we included patients with different follow-up ranging between 26 and 270 months, with consequent possible bias due to different observational time; third, we include a relative low number of patients, that did not allow an accurate statistical analysis of factors influencing failure rate. However, the procedure was performed in a very selected series of pediatric patients affected by rare tumors of the proximal femur.
In conclusion, APC with short stem and compression plate represents an effective reconstructive option after proximal femur resection for primary bone tumors in children and growing patients. This technique offers the following advantages in pediatric age: restoration of bone stock; biological attachment of tendons; feasible in very young children with short and narrow residual distal femur. The use of long compression plate, extended over the proximal part of the greater trochanter, was seen to reduce failure rate. Despite the high rate of mechanical complications in the first years, APC represents a long-lasting durable reconstruction with excellent functional results.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241269338 – Supplemental material for Allograft-prosthesis composite after proximal femur bone tumor resection in pediatric age: Is it effective in preserving bone stock?
Supplemental material, sj-pdf-1-cho-10.1177_18632521241269338 for Allograft-prosthesis composite after proximal femur bone tumor resection in pediatric age: Is it effective in preserving bone stock? by Domenico Andrea Campanacci, Roberto Scanferla, Francesco Muratori, Federico Scolari, Guido Scoccianti, Angela Tamburini and Giovanni Beltrami in Journal of Children’s Orthopaedics
Footnotes
Authors contributions
D.A.C., R.S., and F.M. collected the data and wrote the paper; F.S. and G.S. performed the survival analysis and contributed to data collection; G.S., A.T., and G.B. supervised the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board approval
Ethical approval for the present retrospective observational study was obtained from Comitato Etico Regione Toscana—Area Vasta Centro; ref. 10197/2017. All the patients gave their informed consent to participate in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.