
Abstract
Purpose
The morphology of the proximal femur has been extensively studied in the adult population. However, no literature providing a comprehensive evaluation of the anatomy in paediatric patients exists. The current study aims to characterize such anatomy in skeletally-immature patients, examine potential differences between genders, and analyze how these anatomical parameters change with age.
Methods
Cadaveric femurs from the Hamann-Todd Osteological Collection were examined. Specimens with open physes and no skeletal disease or deformity were included for analysis. Age and gender were recorded for each specimen. Each femur was photographed in standardized modified axial and anteroposterior views. In all, 14 proximal femoral anatomical parameters were measured from these photographs. Comparisons between genders and age were calculated.
Results
A total of 43 femurs from ages four to 17 years met inclusion criteria. The majority were female (56%); no difference existed in age between genders (p = 0.62). The specimens had a neutral mean neck-shaft angle (130.7º) and anteversion (12.8º), and the sphericity of the ossified femoral heads was symmetrical. Male specimens had significantly higher alpha angles (p = 0.01), posterior offset (p = 0.02), neck width (p = 0.04) and head-neck length ratio (p = 0.02) values than female specimens. Strong positive correlations exist between length/size parameters and age, while negligible correlations were noted for angular measurements.
Conclusions
This study establishes reference values for a comprehensive list of anatomical parameters for the skeletally-immature ossified proximal femur. It highlights gender differences in morphology and demonstrates that angular characteristics remain relatively stable while length parameters generally increase with age.
Level of Evidence
Level III Diagnostic
Introduction
The embryological development of the human hip starts as a collection of mesoderm in the lower limb bud that begins to share morphological characteristics with the adult hip around the eighth week of gestation. 1 Much of the continued anatomical development of the hip is influenced by mechanical stresses induced by various muscular attachments, such as the gluteus medius to the greater trochanter and the iliopsoas to the lesser trochanter, as well as containment of the femoral head within the acetabulum. 2 The proximal femur, in particular, is susceptible to myriad paediatric and adult disorders. Conditions such as femoroacetabular impingement and Legg-Calve-Perthes disease, congenital pathologies including proximal focal femoral deficiency, as well as malignancies and trauma such as femoral neck and intertrochanteric hip fractures, among numerous other maladies, affect this portion of the femur.1,3,4 An extensive vocabulary has been developed to describe the anatomy of the proximal femur, ranging from length measurements like femoral head diameter, angular parameters such as neck-shaft angle and version, and relational dimensions including anterior and posterior offset.
The anatomy of the proximal femur in the adult population has been extensively reported. Toogood et al 5 analyzed 375 adult cadaveric femurs in order to provide a global assessment of proximal femoral morphology and comparisons between gender and age. Similarly, Unnanuntana et al 6 performed a limited evaluation of the anatomy of adult femurs, specifically comparing genders and race, based upon only five measurements (neck-shaft angle, femoral head diameter, horizontal and vertical offset, and the distance from the lesser trochanter to the centre of the femoral head). Moreover, Young et al7,8 conducted studies comparing the left and right proximal femurs and found substantial symmetry among adults. Bixby et al 9 performed a cross-sectional investigation examining CT scans of paediatric hips, but only analyzed adolescent subjects and limited their assessment to alpha angle, femoral head diameter, offset and epiphyseal extension. To date, there is no literature providing a comprehensive evaluation of proximal femoral anatomy in the paediatric population.
The purpose of the present study was to determine the proximal femoral morphology in skeletally-immature patients with open physes to define normal reference ranges, compare the anatomy between male and female patients and to analyze how proximal femoral morphology changes with age.
Materials and methods
Cadaveric femurs were assessed from skeletons in the Hamann-Todd Osteological Collection in Cleveland, Ohio. These specimens were derived from unclaimed human remains from the Cleveland city morgue in the early 1900s. Skeletons were included in the present study if they had open proximal femoral physes, as evidenced by separation of the femoral head epiphysis and greater trochanteric apophysis from the femoral neck/shaft. Specimens were excluded from analysis if the femurs were not intact, there was a history or clinical evidence of skeletal disease or gross deformity that impacted skeletal development, or if the age or gender was not recorded.
As described by Toogood et al, 5 every femur which met inclusion criteria was digitally photographed in standardized modified axial and anteroposterior positions. In this arrangement, the femoral neck was perpendicular to the sight line of the camera with the femoral shaft oblique to the camera. In order to accurately reconstruct the proximal femur, the femoral head epiphysis and greater trochanteric apophysis were reattached using a layer of evenly-distributed adhesive putty < 1 mm thick (Fig 1). Borders of the femoral head/greater trochanter and shaft were typically congruent and fit together in a lock-and-key fashion like a 3D puzzle piece. If a discrepancy existed when reconstituting the physis, the specimen was excluded from analysis. In a similar manner, the distal femoral condylar components were also reattached in order to facilitate an accurate evaluation of the femur.

Technique for reconstructing femoral components in each specimen: (
Demographic information, including the age at death and gender, were recorded for each cadaveric specimen. ImageJ software (version 1.48, National Institutes of Health, Bethesda, Maryland) was used to assess 14 anatomical parameters of the proximal femur from the photographs of each specimen (Figs 2, 3 and 4). These included neck-shaft angle, anteroposterior head diameter, neck length, head-neck length ratio, anterior offset, posterior offset, offset ratio, anterior offset ratio (AOR), lateral head width, neck width, head-neck width ratio, version, alpha angle and beta angle. A calibration ruler placed in each digital photograph was used to convert pixels to millimetres, and all measurements were performed using previously established techniques.5–7
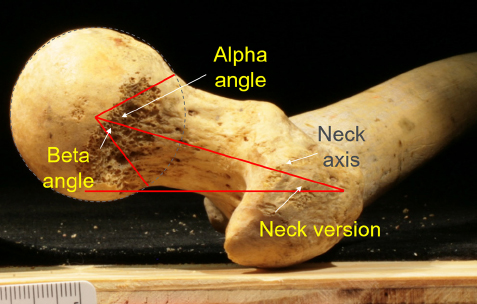
Angular measurements obtained from each specimen. Dotted line represents a best-fit circle around the femoral head.
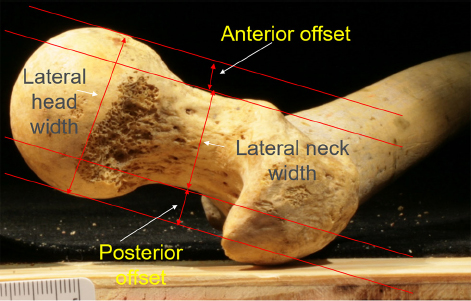
Length measurements on modified axial view.
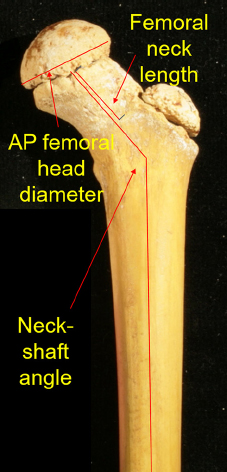
Measurements obtained on anteroposterior view.
The anterior offset was calculated as the distance between a line drawn along the anterolateral edge of the femoral neck and another parallel line tangent to the anterolateral aspect of the femoral head. In a similar fashion, posterior offset was calculated as the distance between a line drawn along the posterolateral edge of the femoral neck and another parallel line tangent to the posterolateral aspect of the femoral head. Offset ratio refers to the ratio of the anterior to posterior offset values. The AOR is equal to the anterior offset divided by the femoral head diameter. Version was calculated as the angle between a line parallel to the floor and a line through the long axis of the femoral neck. This definition of version, described and used by Toogood et al, 5 is slightly different to the more traditional definition as the apparent angle of the femoral neck and bicondylar plane when the femur is viewed parallel to the femoral shaft. The bony alpha angle was measured with the aid of a best-fit circle using the method described by Toogood et al. 5 Beta angles were calculated using this same method, but were based off of the posterior (rather than anterior) cortex. The neck-shaft angle, anteroposterior head diameter, neck length and head-neck length ratio were based upon measurements on the anteroposterior views, while the lateral head width, neck width, and the head-neck width ratio were based upon the modified axial views.
All statistical analyses were performed using SPSS (version 16.0.1, Chicago, Illinois). Unpaired Student's t-tests were implemented to compare differences between genders. The Pearson Correlation Coefficient (‘r’) was calculated to assess for changes in each of the 14 anatomical parameters with increasing age and p-values are two-tailed with p < 0.05 as the threshold for statistical significance.
Results
A total of 43 femurs met the inclusion criteria from the osteological collection. Of these, 19 (44%) were male and 24 (56%) were female. Overall, these specimens ranged in age from four to 17 years old. Male femurs had a mean age of 11.2 years (sd 4) while female femurs had a mean age of 10.6 years (sd 3.5). There was no significant difference in the ages of each gender cohort (p = 0.62).
Table 1 illustrates the mean values of each of the 14 anatomical parameters for the entire study population. The specimens had a neutral mean neck-shaft angle of 130.7° (neither varus nor valgus) with a version of 12.8°. The sphericity of the ossified femoral heads was symmetrical, with similar mean alpha and beta angles of 49.5° and 44.8°, respectively, as well as a similar mean anteroposterior head diameter (34.4 mm) and lateral head width (33.5 mm). Moreover, the anterior (mean 6.4 mm) and posterior (mean 7.1 mm) offset values were also similar with an offset ratio of 0.9.
Overall measurements of entire population
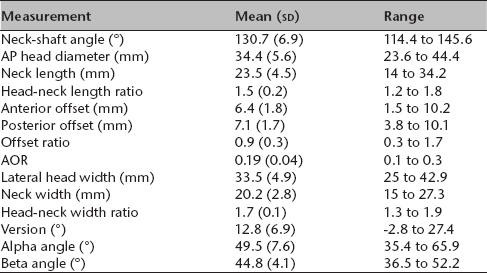
AP, anteroposterior; AOR, anterior offset ratio
All measurements were stratified by gender. As noted in Table 2, male specimens (mean 52.9°) had significantly higher alpha angles compared with their female counterparts (mean 46.9°) (p = 0.01). Additionally, male specimens had significantly higher mean posterior offset (7.8 mm versus 6.5 mm) and neck width (21.1 mm versus 19.4 mm) values than female specimens (p = 0.02 and 0.04, respectively). While male specimens had a significantly higher head-neck length ratio (p = 0.02), female specimens had a higher offset ratio (p = 0.01). There were no significant differences between genders in terms of the other recorded anatomical measurements, including neck-shaft angle, anteroposterior head diameter, neck length, anterior offset, AOR, lateral head width, head-neck width ratio, version and beta angle.
Measurements stratified by gender
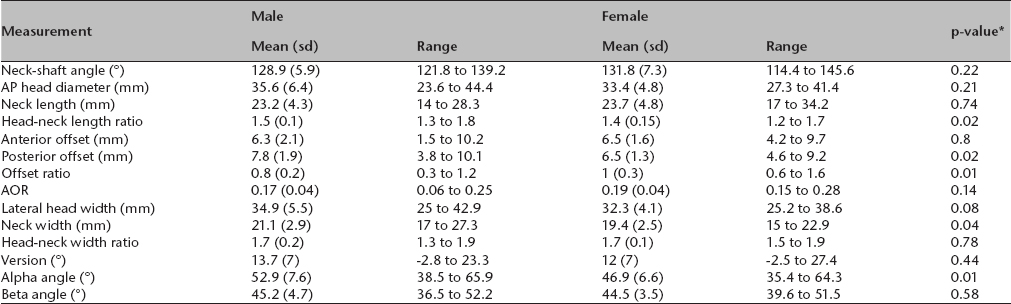
AP, anteroposterior; AOR, anterior offset ratio
Calculated using the Unpaired Student's t-test
Table 3 shows the correlations of each of the measurements with respect to age. Strong positive correlations were found for anteroposterior head diameter (r = 0.85), neck length (r = 0.78), anterior offset (r = 0.69), posterior offset (r = 0.69), lateral head width (r = 0.83) and neck width (r = 0.66). This indicates that length/size parameters generally steadily increased with age. Negligible correlations were noted for neck-shaft angle, version and alpha angle (r = 0.09 for each), while a weak negative correlation was found for beta angle (r = -0.29). This suggests that angular measurements remain relatively constant over time.
Correlation of anatomical parameters with respect to age
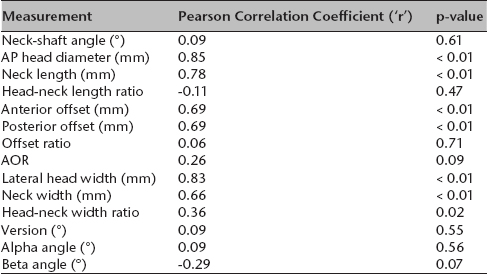
AP, anteroposterior; AOR, anterior offset ratio
Discussion
The present study provides reference values for a comprehensive list of anatomical parameters of the paediatric proximal femur (Table 1). A partial assessment of the geometry of the proximal femur has been reported in previous studies by Toogood et al 5 in an adult population and by Bixby et al 9 in a paediatric cohort. However, Bixby et al's 9 study only assessed adolescent subjects ages 12 to 18 years, and limited their assessment to alpha angle, femoral head diameter, offset and epiphyseal extension. As such, there is insufficient knowledge to characterize the relationship of multiple morphologic parameters of the paediatric femur. Using cadaveric specimens, we attempted to: 1) create a set of reference values for normal paediatric proximal femoral anatomy; 2) characterize differences in these parameters between genders; and 3) assess the natural history of morphologic characteristics of the paediatric proximal femur that are identified to change over time.
Due to the extensive measurements assessed in this study, comparative data were not available for all parameters. However, when available, our data is consistent with previously-reported data, supporting the validity of the methodology of this study which was performed in accordance with known standards of femoral assessment. 6 Bixby et al 9 reported median alpha angles in paediatric males between 41° and 52° (52° on an anterosuperior CT section plane) and 39° to 49° in female patients (49° on anterosuperior section). These are similar to our findings of 52.9° in male and 46.9° in female femurs (p = 0.01). Furthermore, their study reported no difference between genders regarding anterior offset but found posterior offset to be higher in male patients (7.6 mm versus 7.3 mm), similar to our study (7.8 mm versus 6.5 mm, p = 0.02).
The present study identified multiple statistically significant differences between skeletally-immature male and female femurs including head-neck length, posterior offset, offset ratio, neck width and alpha angle. Among these, all values were significantly larger in the male group, with the exception of offset ratio; since posterior offset was increased in males, while anterior offset was not significantly different between groups, this led to a decreased offset ratio in the male cohort (0.8 versus 1.0, p = 0.01). The generally larger skeletal framework of boys/men may account for the other stated differences.
Furthermore, this data identifies several femoral parameters that have strong correlations with age. These parameters include anteroposterior head diameter, neck length, anterior offset, posterior offset, lateral head width and neck width. Head-neck width ratio was found to have a moderate correlation with age (r = 0.36). Of note, it is important to identify morphological parameters that were not found to have a correlation with age. These included neck-shaft angle, head-neck length ratio, offset ratio, AOR (weak correlation), version and alpha angle. Understanding these changes in femoral morphology over time can be generalized into the statements that length and size parameters, as expected, increase with age and, conversely, angular parameters remain relatively constant throughout skeletal development. Of note, we found that femoral version was not correlated with age (r = 0.09, p = 0.55). These data are in contrast to the reported natural history of femoral version which is believed to typically decrease from 40° at birth to 15° at skeletal maturity. 3 We found a mean version of 12.8° (sd 6.9°, -2.8° to 27.4°) with an age range between four and 17 years. Our data may be inconsistent with previously reported trends due to the unequal distribution of our data with most femurs being ten years or older, and only seven femurs under the age of eight years (due to the rarity of such young skeletal remains). It is possible that evaluation of a larger subset of infant or toddler proximal femurs could reveal a different trend.
The data and trends highlighted in the present study provide the surgeon with quantitative standards to assist with restoring the geometry of the proximal femur, such as in cases of reconstruction for congenital deformities or fractures. Additionally, these data help clarify the natural history of the changes in multiple morphologic parameters that have been used to in diagnosing multiple orthopedic conditions. Femoroacetabular impingement, a recently identified cause of early onset osteoarthritis, may cause bony and cartilaginous damage secondary to femoral head asphericity (cam-type) or acetabular deformity (pincer-type). 10 Radiographic parameters for diagnosing femeroacetabular impingement have been suggested, although radiologists may be cautious of diagnosing it based on imaging studies as it is largely a clinical diagnosis. 11 Still, radiographic parameters such as alpha angle, offset and physeal extension have been used to suggest the presence of femeroacetabular impingement in a paediatric population. Previously, alpha angle thresholds for cam-type femeroacetabular impingement have been proposed at 50°, 12 50.5°,13,14 55°13,15,16 and higher. Our data reports a mean bony alpha angle of 49.5° (sd 7.6°, 35.4° to 65.9°), further supporting previous assertions that lower alpha angle threshold values may over-predict femeroacetabular impingement in paediatric populations. Recent literature has suggested that paediatric femeroacetabular impingement may develop due to localized anterolateral epiphyseal extension at the peripubertal proximal femoral growth plate, leading to development of femeroacetabular impingement near the time of skeletal maturity. 17 As such, the alpha angle may be inappropriate for diagnosing femeroacetabular impingement in a younger patient population, especially as radiographs cannot account for the cartilaginous portion of the proximal femur. Our data suggest a very strong correlation between anteroposterior head diameter and age (r = 0.85), further supporting the notion that alpha angle may become more acute as the femoral head grows, and use of the bony alpha angle for femeroacetabular impingement diagnosis in a paediatric population may over-diagnose cam-type femeroacetabular impingement, particularly when lower alpha angle value thresholds are utilized for diagnosis.
This study, however, has limitations. Data collection was conducted on cadaveric specimens from a collection of human skeletal remains. These specimens were collected between 1912 and 1938, and as such are suspect to decay as well as to metabolic diseases affecting bone quality during the life of these individuals. Care was taken to exclude any specimens from the study that could not be properly recreated or where bone disease was clearly present. Nonetheless, the nature of the osteological collection makes it impossible to account for the cartilaginous portion of bone which could affect study results. Furthermore, the relatively small sample size of this study and lack of clinical data regarding the specimens, including cause of death, makes generalizability of these results to a modern population more challenging. Future studies with larger sample sizes should be performed to confirm these reference values in a paediatric population, and use of MRI analysis could be used to allow for assessment of the cartilaginous portions of the femur within this population.
In conclusion, this study provides a comprehensive assessment of 14 morphological parameters of the paediatric proximal femur. These data establish a set of reference values that may be used to assist radiologists and orthopaedic surgeons in the diagnosis or treatment of many conditions affecting youths, including femeroacetabular impingement. Our data also highlight several significant differences in femurs of male and female patients during the period leading to skeletal maturity. Furthermore, a strong correlation is found with length and size parameters of the paediatric femur as a function of age, whereas angle parameters remain relatively constant as the proximal femur grows.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical Approval: This article does not contain any studies with human participants or animals performed by any of the authors.