
Abstract
Purpose:
Fractures occurring at the metaphyseal–diaphyseal junction of the distal humerus in children are not commonly documented in the literature. Until this moment, there is no gold standard technique regarding its management and most surgeons treat it as a regular supracondylar humerus fracture by conventional pinning. This systematic review explores the relevant literature to assess the efficacy of different techniques.
Methods:
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Our literature search encompassed several online databases, including PUBMED/MEDLINE, Scopus, Web of Science Core Collection, and Google Scholar. Data from articles that met our general inclusion criteria were extracted and categorized into treatment method groupings. Functional and cosmetic outcomes, demographic characteristics, and complications were the main parameters used to analyze the data.
Results:
Ten retrospective studies met our inclusion criteria with a total of 178 participants of unilateral pediatric distal humerus metaphyseal–diaphyseal junction fractures. Most literature chose closed reduction and percutaneous pinning in seven articles, followed by elastic stable intramedullary nail technique used in three articles, then conservative treatment was chosen in two articles, while only one article used lateral miniplate and assisted K-wire and another article used combined closed reduction and percutaneous pinning and intramedullary K-wire. As regards the operation time; elastic stable intramedullary nails had the shortest time with a mean of 39.7 min (range: 37.5–41.9 min), while closed reduction and percutaneous pinning had the longest time with a mean of 75.47 min (range: 55.9–92.1 min). The shortest healing time was observed in miniplate with a mean of 7.2 weeks, while the most prolonged was in conservative management with a mean of 12 weeks and closed reduction and percutaneous pinning was a mean of 10 weeks. Regarding Flynn’s criteria, all participants received excellent and good except in closed reduction and percutaneous pinning; 13 cases were fair and 2 cases were poor. Regarding complications, the most commonly observed complication after metaphyseal–diaphyseal junction fracture was cubitus varus, the highest incidence was in conservative management (33% of cases), followed by closed reduction and percutaneous pinning (10.9% of cases), the least incidence was observed in elastic stable intramedullary nails (3.77% of cases), and none of the cases treated with mini plate developed this complication. Other complications were observed only with closed reduction and percutaneous pinning; 8.5% of cases developed fixation loss, 6.2% of cases had a significantly reduced range of motion, and one case refractured.
Conclusion:
Pediatric distal humerus metaphyseal–diaphyseal junction fractures should be distinguished from the more prevalent supracondylar humerus fractures, as conventional pinning techniques are associated with a higher incidence of complications and increased both operative and healing times.
Keywords
Introduction
The Supracondylar humerus fracture is the most frequent pediatric elbow fracture, comprising approximately 17% of all childhood fractures and 58% of all pediatric elbow fractures. 1 It is typically described as fractures proximal to distal humeral condyles passing through the thin cortical bone of the olecranon fossa. The most common cause of fracture is a fall onto an outstretched hand during sports and recreational activities. The peak incidence is among the 4–9-year-old age group. Displaced fractures are generally managed by closed reduction and pinning either lateral pins or crossed lateral and medial pins. 2
Fractures at the metaphyseal–diaphyseal junction (MDJ) of the distal humerus, situated proximal to the olecranon fossa were first described by Fayssoux et al. 3 MDJ fracture is very rare, approximately 3% of supracondylar humerus fractures. 3 Two horizontal lines are drawn in the anteroposterior plain X-ray of the distal humerus, the first line lies where the width of the humeral shaft begins to expand, while the second line is at the upper boundary of the olecranon fossa. A fracture occurring between these two lines is classified as an MDJ fracture of the distal humerus 4 (see Figure 1).
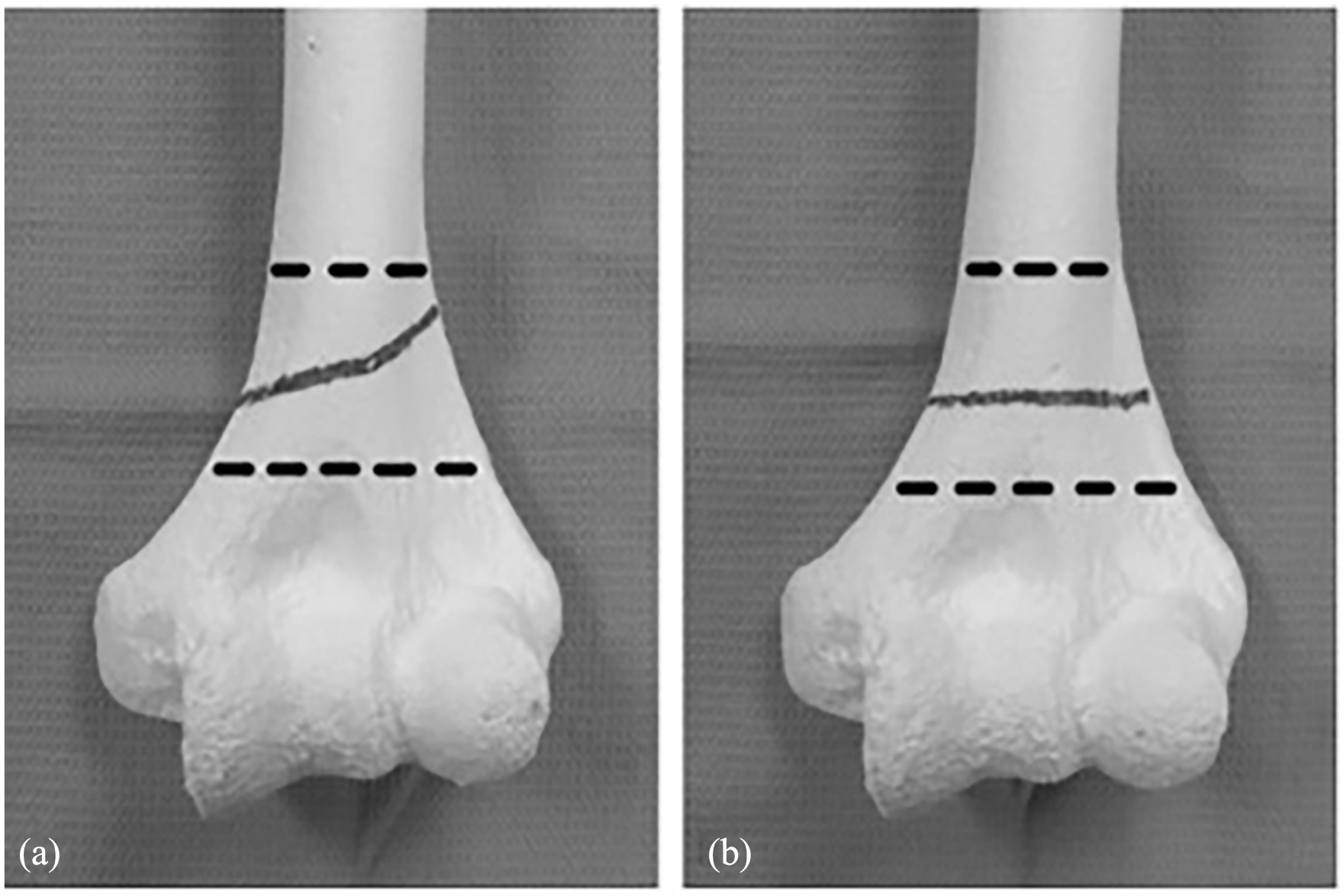
Dotted lines demarcate the metaphyseal–diaphyseal area. (a) Oblique fracture pattern and (b) transverse fracture pattern.
MDJ fracture should be differentiated from typical supracondylar humerus fracture as the fracture line passes just above the olecranon fossa where the bone’s cross-sectional area is significantly reduced than that in the supracondylar area. This makes achieving adequate fixation challenging, as the pins often intersect at a high fracture level with a trajectory almost parallel to the humeral axis, leading to decreased axial and rotational stability.3,5
The above-mentioned criteria of MDJ fracture require its management by classic pinning because regular supracondylar fractures are associated with a higher incidence of failure and postoperative complications.6,7 In the past two decades, numerous techniques have been described for the management of pediatric distal humerus MDJ fracture; however, none of these techniques is defined as a gold standard for the management of MDJ fracture. This study will analyze and compare different management techniques.
Methods
Search strategy
Published studies before February 2024 regarding MDJ fracture were first identified through a wide search via relevant databases including PUBMED/MEDLINE, Scopus, Web of Science Core Collection, and Google Scholar. A variety of medical subject headings was used to identify the relevant articles including (metaphyseal diaphyseal or metaphyseo-diaphyseal or high supracondylar or supra-olecranon) and (Pediatric or Children or immature bone).
Population, intervention, comparison, and outcome
Population, intervention, comparison, and outcome (PICO) was defined as follows. P: displaced distal humerus MDJ fracture in children with immature bone; I: closed reduction and percutaneous pinning (CRPP); C: other fixation techniques in studies that meet our inclusion criteria; O: clinical outcome (functional and cosmetic), healing time, operative time, and complications including fixation loss, iatrogenic nerve injury, refracture, and cubitus varus.
Study selection
Two reviewers independently conducted a literature search for studies including the management of distal humerus MDJ fractures in pediatric patients. The searches followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Any disagreements were resolved through discussion with a third researcher.
Eligibility criteria
Studies were only included in the review if they are: (1) human subjects studies, (2) distal MDJ fracture, (3) open physis, (4) include some of the outcomes mentioned above. (5) minimum 9 months follow-up (the time between the fracture and the final assessment).
Studies were excluded if they are: (1) biomechanical studies, (2) typical supracondylar humerus fracture, (3) case reports, (4) closed physis, (5) case series of less than five cases.
Statistical analysis
To characterize the research and the patient’s demographics and outcome measures, descriptive statistics including mean, standard deviation, median, range, percentage, and when applicable the 95% confidence interval were utilized. Statistical analysis was conducted using Review Manager software (RevMan version 5.4.1 for Windows). Effect sizes for dichotomous data were calculated using random-effect models and reported as event rates. Mean values of continuous data were compared with a t-test. Each effect size was accompanied by a 95% confidence interval. Heterogeneity was assessed using the I² statistic, ranging from 0% (indicating complete consistency) to 100% (indicating complete inconsistency).
Results
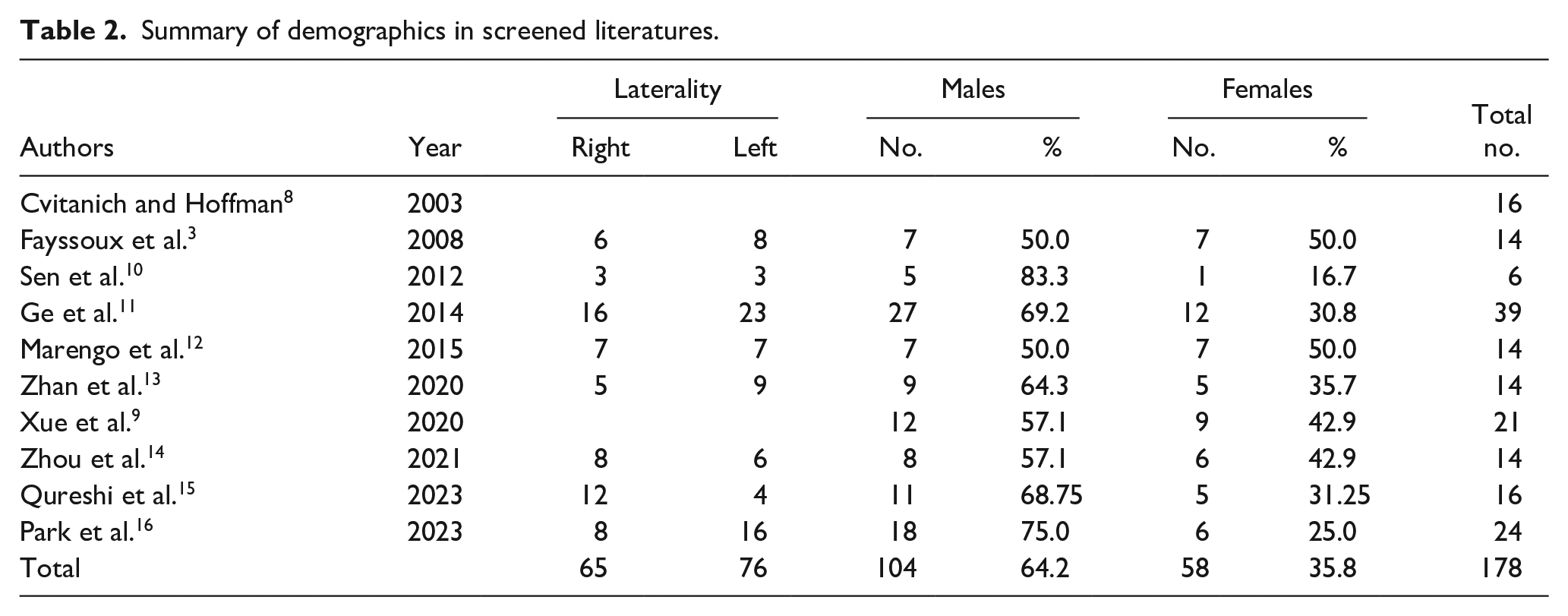
Ten studies in literature had fulfilled the study criteria and were included in this study according to the illustrated PRISMA figure. In this study, 178 participants in the 10 studies included unilateral pediatric distal humerus MDJ fractures; they were 104 males (64.2%) and 58 females (35.8%), one study 8 did not mention gender. Males were much more dominant than females. Regarding laterality, 65 cases (46.1%) were right-sided and 76 cases (53.9%) were left-sided, two studies did not mention laterality8,9 (see Figure 2 and Tables 1 and 2).
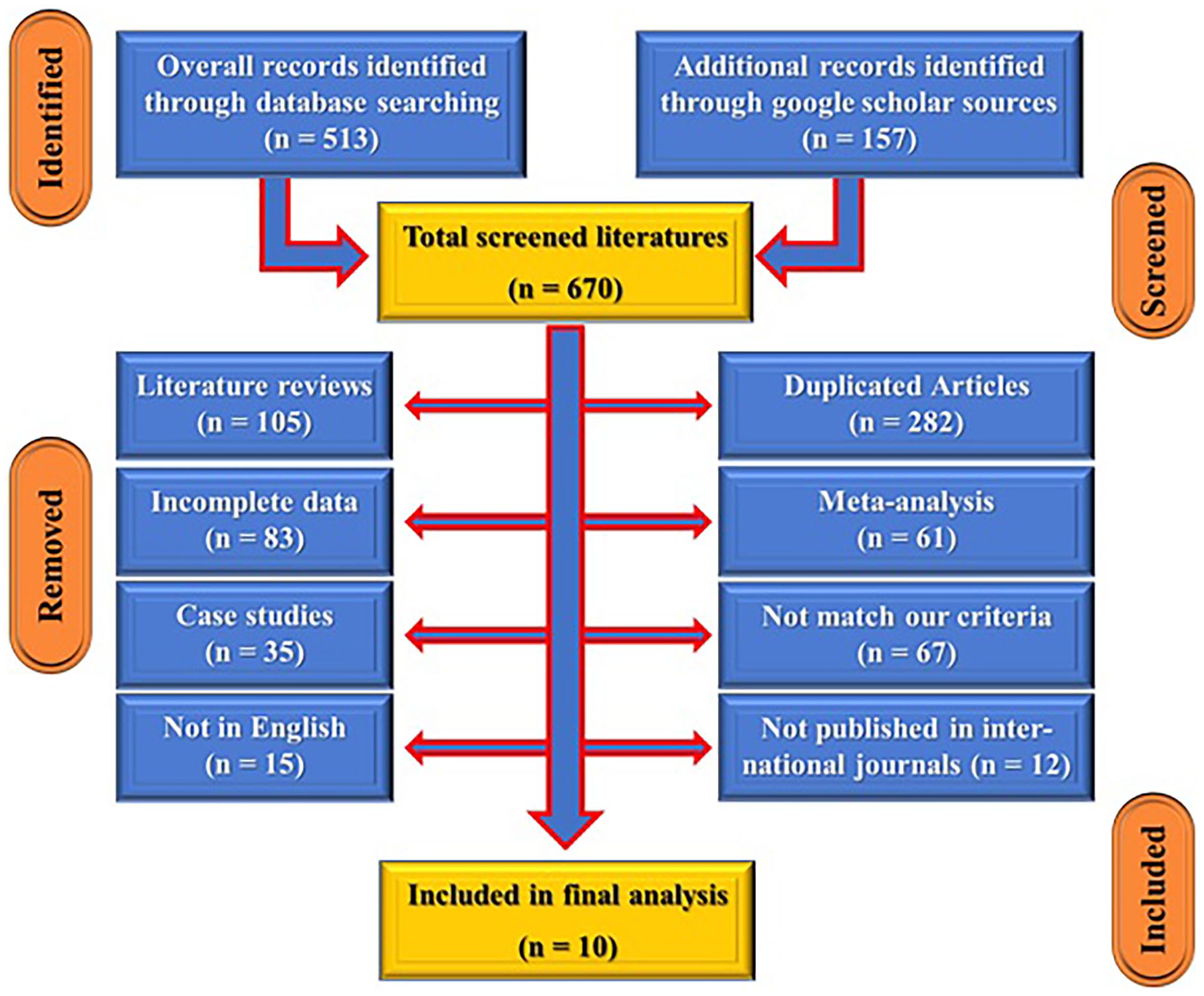
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) search strategy for our study selection.
Summary of the included studies.
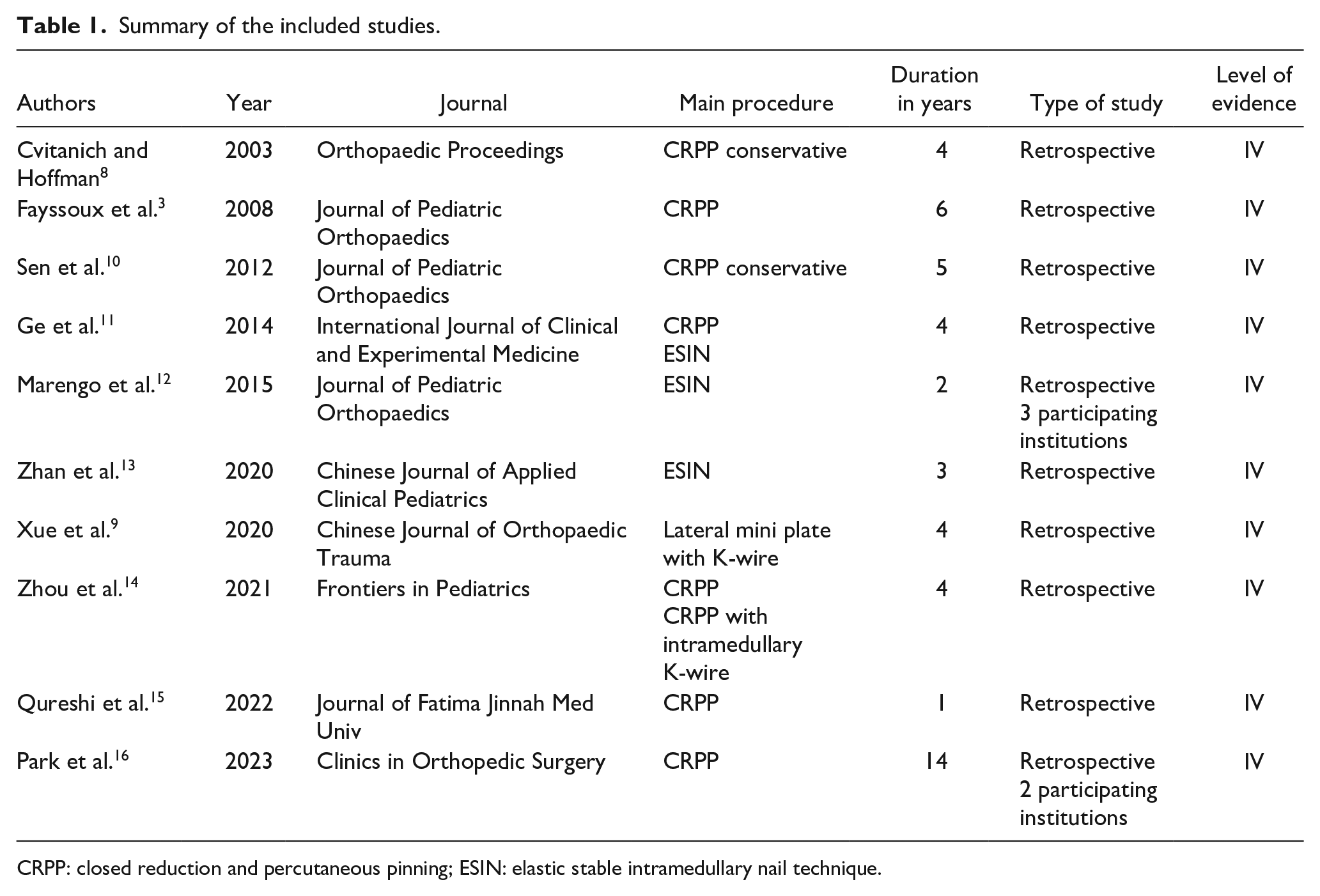
CRPP: closed reduction and percutaneous pinning; ESIN: elastic stable intramedullary nail technique.
Summary of demographics in screened literatures.
The mean age of patients ranged between 4.5 and 9.7 years with a mean ± SD of 6.207 ± 1.757 years. Study duration (the number of years retrospectively reviewed for MDJ fractures in each article) ranged between 1 and 14 years with a mean of 4.7 ± 3.56 years.
Mechanism of fractures were mentioned in eight study literature where 113 patients (80.7%) had a fall and 27 patients (19.2%) had road traffic accidents.
Fracture patterns were mentioned in six study literature; 85 fractures were oblique in 43 patients (50.6%), 33 transverse fractures (38.8%), and 9 comminuted fractures (10.6%). The follow-up period of all studies ranged from 1 to 2 years with a mean of 1.357 ± 0.476 years (see Table 3).
Patients and study characteristics in the studied literatures.
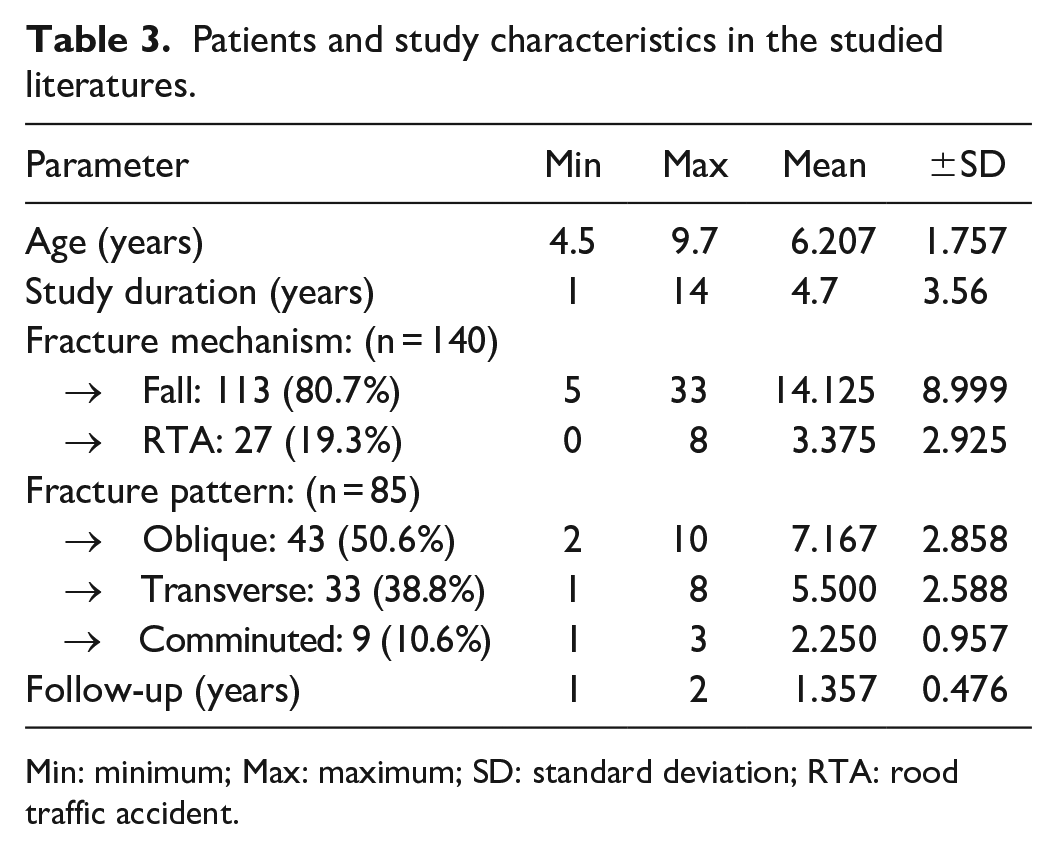
Min: minimum; Max: maximum; SD: standard deviation; RTA: rood traffic accident.
Most of the literature chose the CRPP technique in seven articles (70%) done for 94 patients (52.81%), followed by elastic stable intramedullary nail (ESIN) technique used in three articles (30%) done for 48 patients (26.97%). Conservative treatment was done in two articles (20%), which was performed for 9 patients (5.056%); whereas only one article (10%) used lateral miniplate and K-wire for 21 cases (11.79%) and one article (10%) used combined CRPP and intramedullary (IM) K-wire for 9 cases (3.37%) (see Table 4 and Figures 3–6).
Different treatment modalities in the studied literatures.
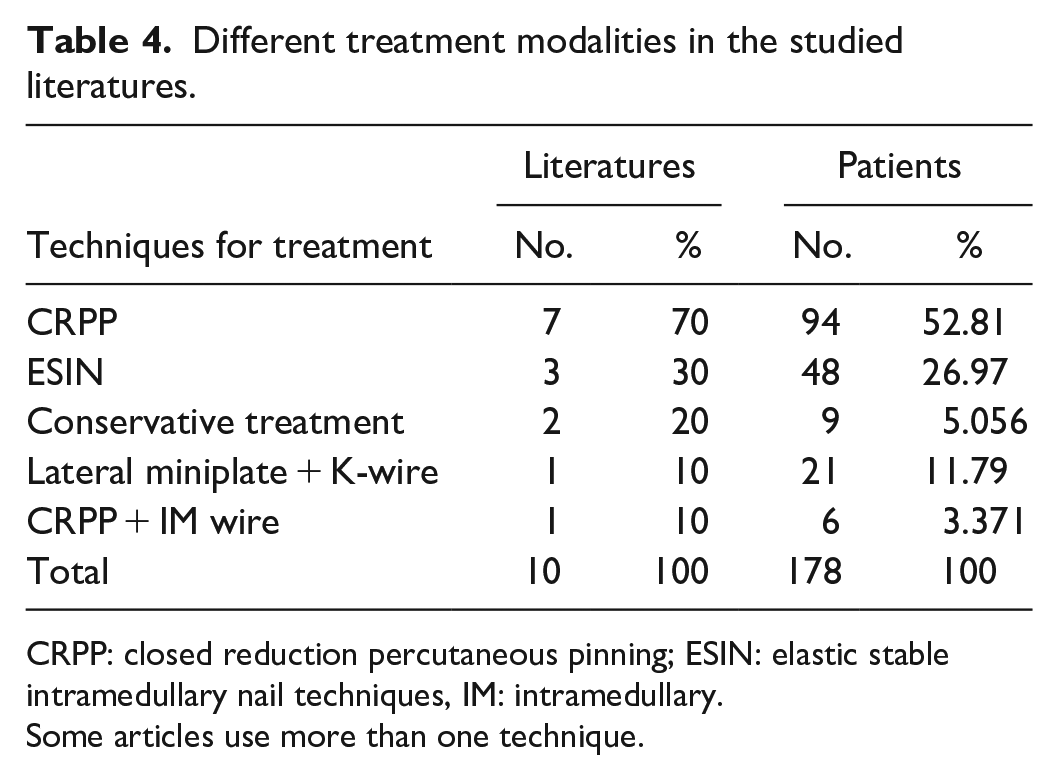
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail techniques, IM: intramedullary.
Some articles use more than one technique.
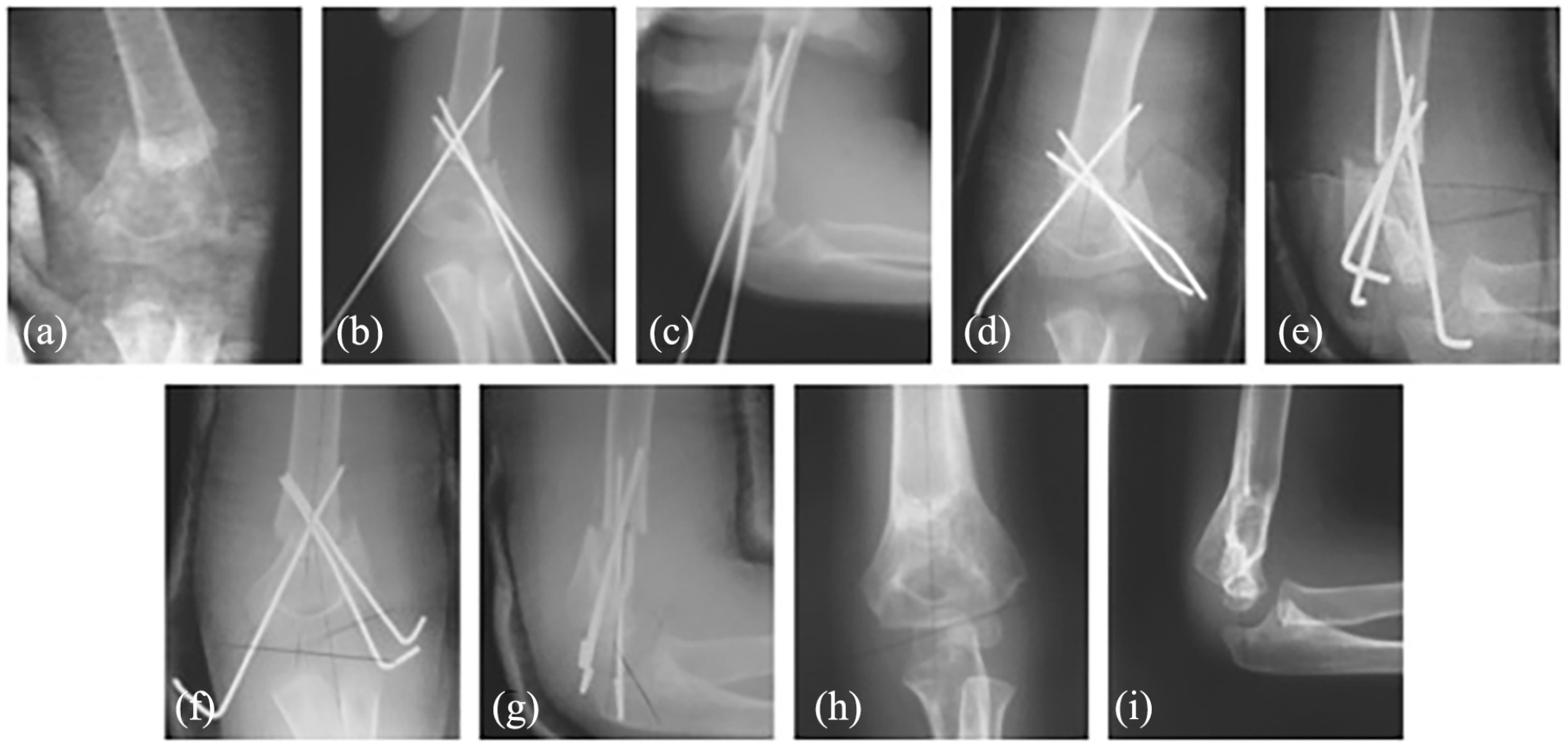
CRPP. (a) Preoperative X-ray, (b, c) postoperative X-ray, and (d, e) 1-week follow-up. There has been a loss of fixation in the coronal and sagittal planes. (f, g) Radiographs after revision and (h, i) 9-month follow-up showing healing on slight extension.
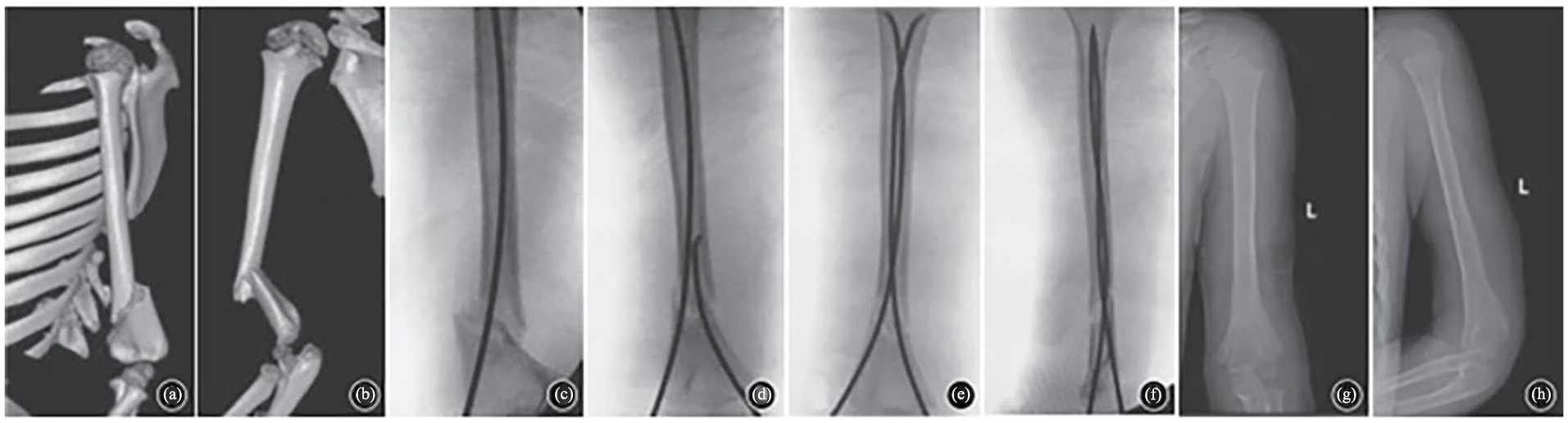
ESIN. (a, b) Preoperative CT, (c–f) intraoperative fluoroscopic images, and (g, h) 9-month follow-up with hardware removal.
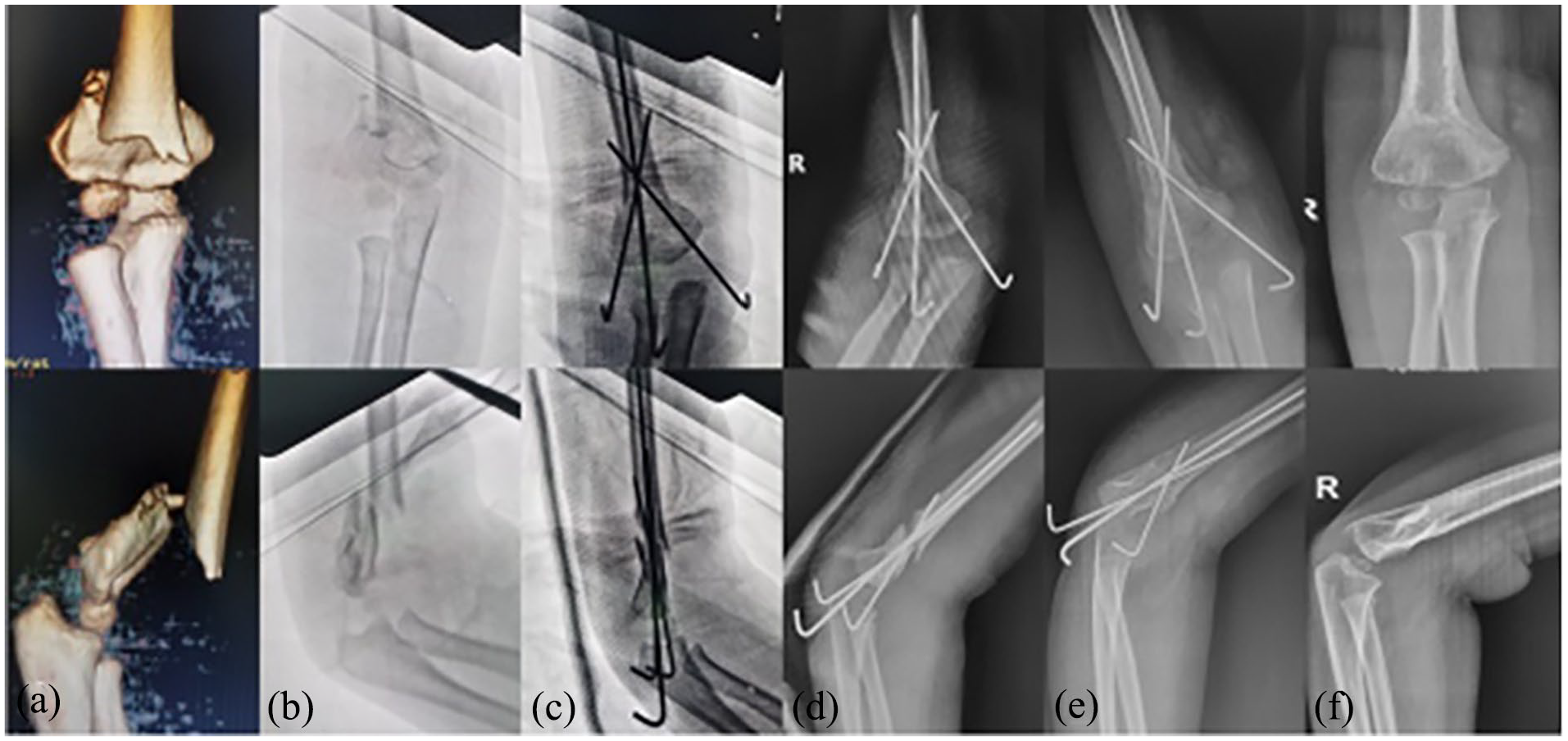
Crossed-pinning with IM K-wire. (a) Preoperative CT, (b) preoperative X-ray, (c) intraoperative post-fixation, (d) 1 day after surgery, (e) 4 weeks postoperatively, and (f) 12 months postoperative follow-up.
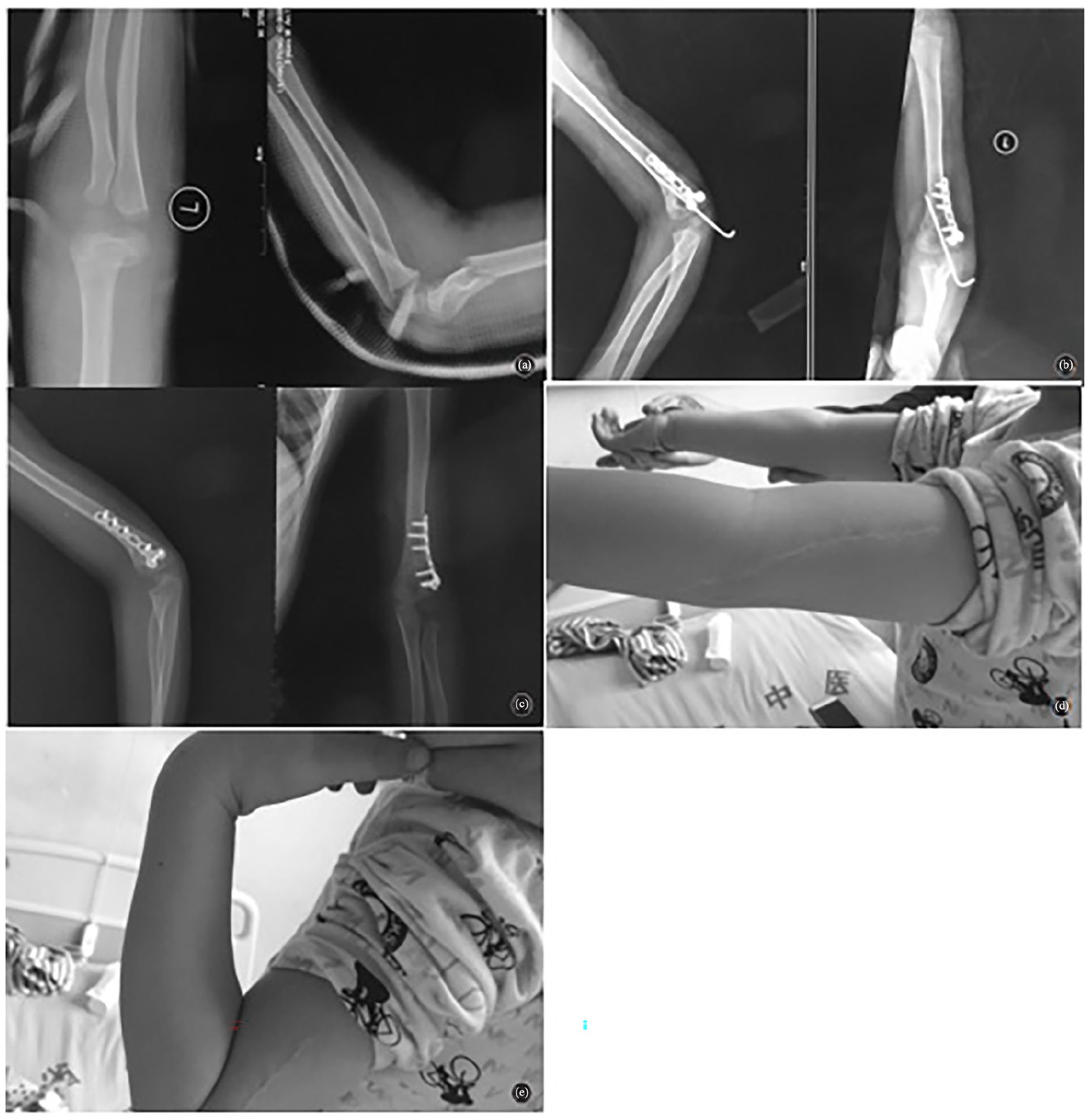
Lateral mini plate and assisted K-wire. (a) Preoperative X-ray, (b) 2 days postoperative, (c) 6-month follow-up, (d) full extension at 6 months, and (e) full flexion at 6 months.
Regarding the operation time, CRPP had the most prolonged time with a mean of 75.47 min (range: 55.9–92.1 min), while ESIN had the lowest time with a mean of 39.7 min (range: 37.5–41.9 min). CRPP + IM wire was mentioned in one study (Zhou et al., 2021) 14 with a mean time of 41.67 min (see Table 5).
Operative times in the studied literatures.
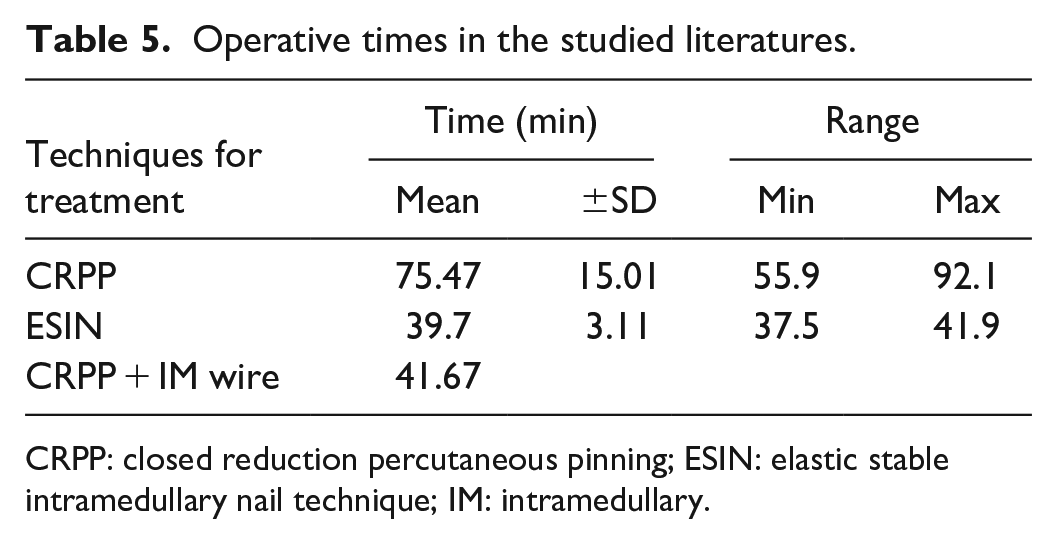
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail technique; IM: intramedullary.
Regarding healing time, the shortest healing time was for miniplate with a mean of 7.2 weeks, the longest was for conservative management with a mean of 12 weeks, while ESIN and CRPP had a mean of 7.9 and 9.97 weeks, respectively (see Table 6).
Healing times of treatment procedures in the studied literatures.
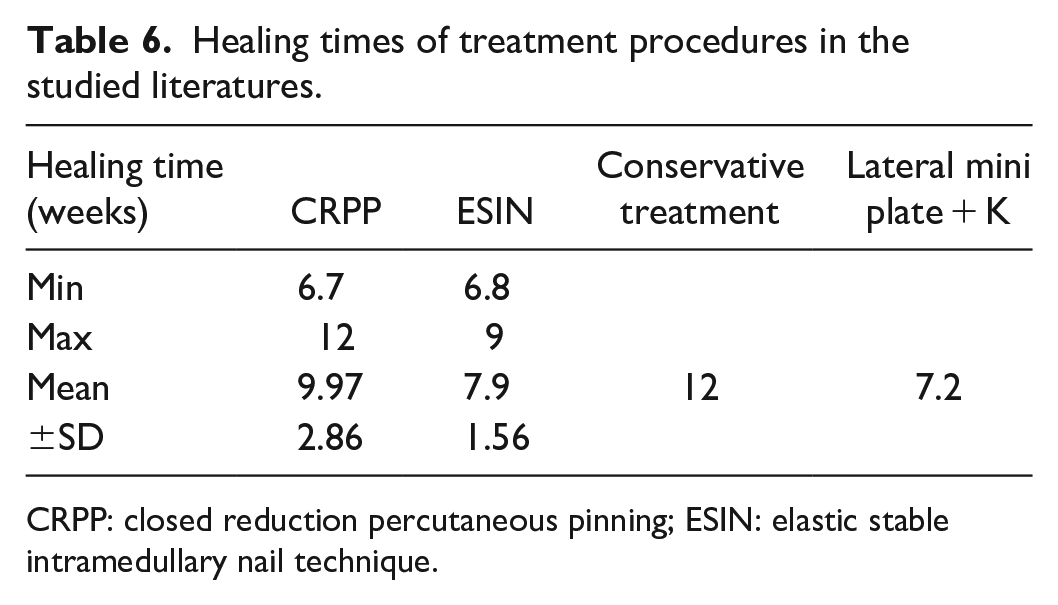
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail technique.
There is a significant difference regarding healing time between different treatment procedures (p < 0.05) except between ESIN and lateral miniplate + K-wire, it was insignificant (p > 0.05; see Table 7).
Test of significance of healing times between different treatment groups.
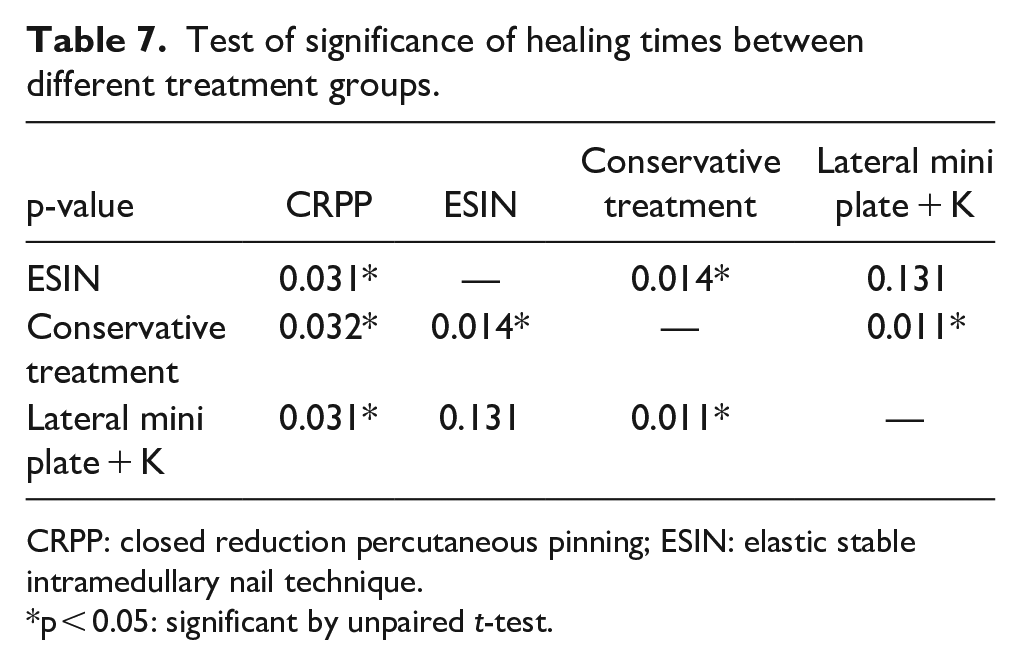
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail technique.
p < 0.05: significant by unpaired t-test.
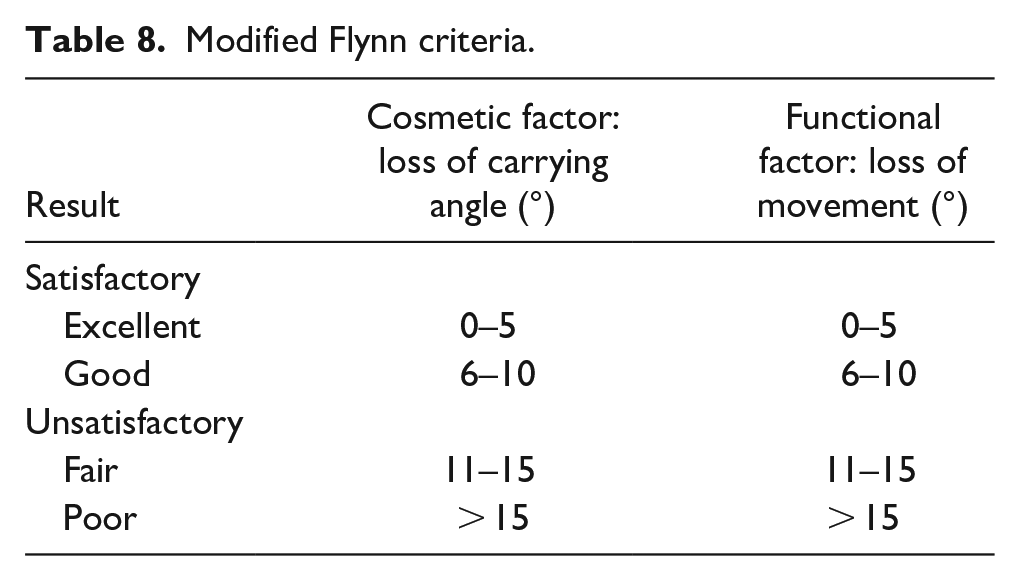
Regarding Flynn’s criteria (which is widely accepted for outcome assessment of pediatric supracondylar fractures), it combines functional outcome (loss of range of motion) and cosmetic outcome (loss of carrying angle) 15 In the CRPP method, the outcomes mentioned in four articles were as follows: 25/49 (51%) cases were excellent, 9/49 cases (18.4%) were good, 13/49 cases (26.5%) were fair, and 2/49 cases (4.08%) were poor. In the ESIN method, 13/14 cases (92.9%) were excellent and 1/14 cases (7.14%) were good in one article only. In conservative treatment patients, 5/6 cases (83.3%) had an excellent outcome and 1/6 cases (16.7%) had a good outcome in one article only. In lateral mini plate + K wire, 19/21 cases (90.5%) show excellent outcomes and 2/21 cases (9.52%) show good outcomes in one article only. In CRPP + IM wire technique, 4/6 cases (66.7%) showed excellent outcomes and 2/6 cases (33.3%) had good results in one article only. In this study, we will consider results of excellent and good as satisfactory outcomes (see Tables 8–11, Figures 7–10).
Modified Flynn criteria.
Comparison of different treatment procedures regarding Flynn criteria.
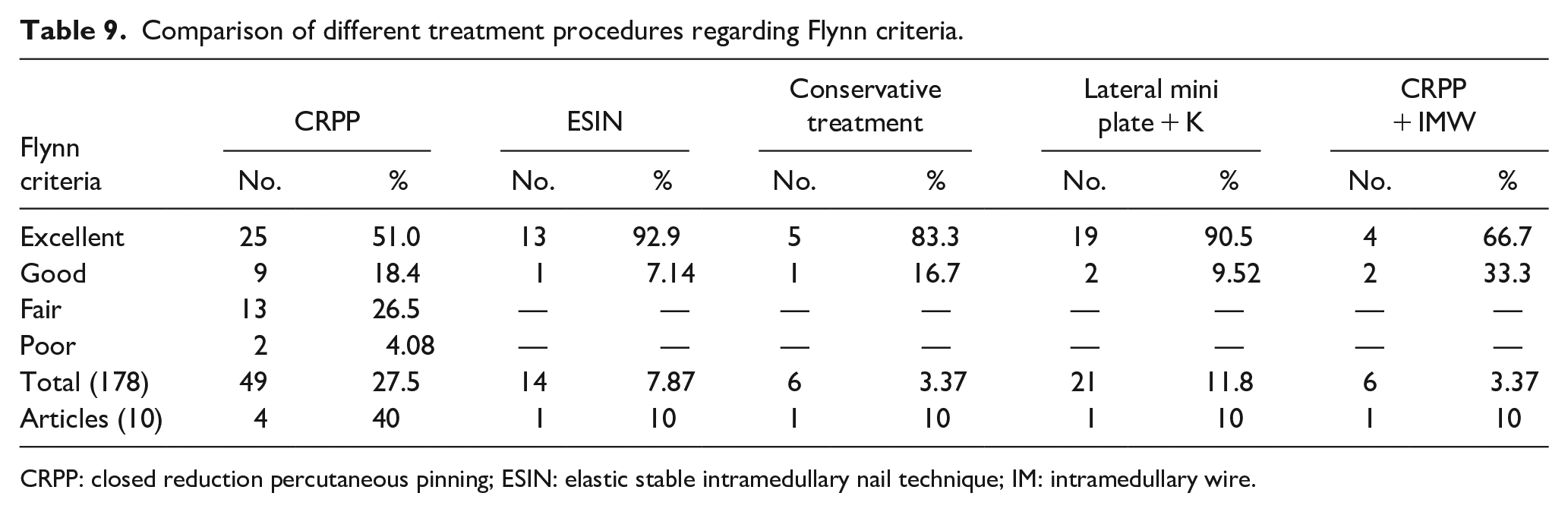
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail technique; IM: intramedullary wire.
Meta-analysis for satisfactory outcome (excellent, good) after closed reduction percutaneous pinning (CRPP) technique.
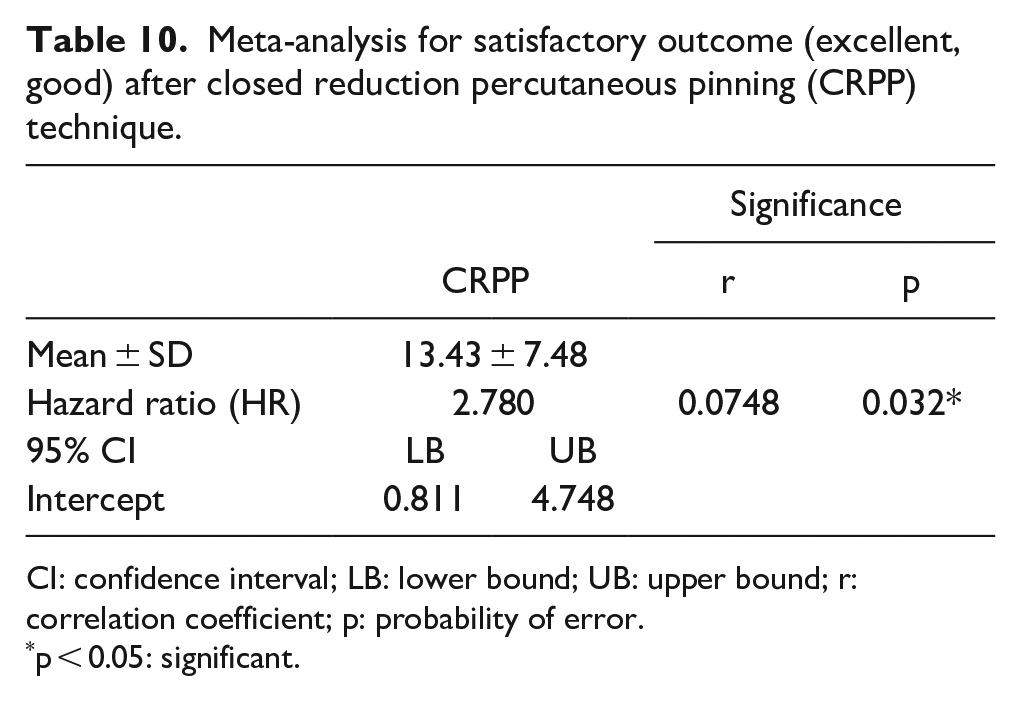
CI: confidence interval; LB: lower bound; UB: upper bound; r: correlation coefficient; p: probability of error.
p < 0.05: significant.
Meta-analysis for satisfactory outcome (excellent, good) after elastic stable intramedullary nail (ESIN) techniques.
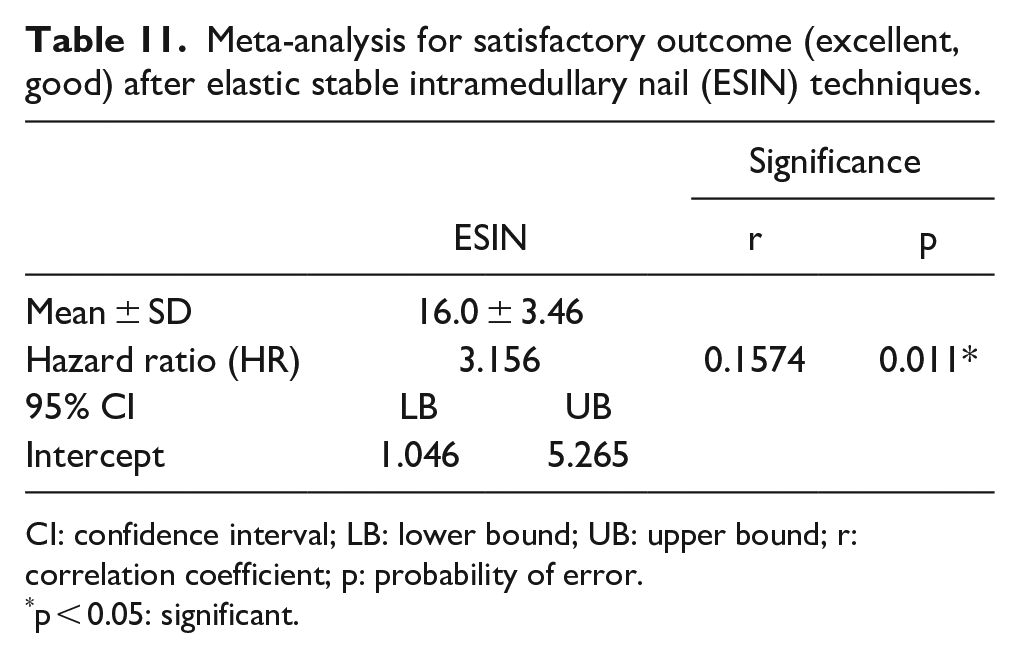
CI: confidence interval; LB: lower bound; UB: upper bound; r: correlation coefficient; p: probability of error.
p < 0.05: significant.
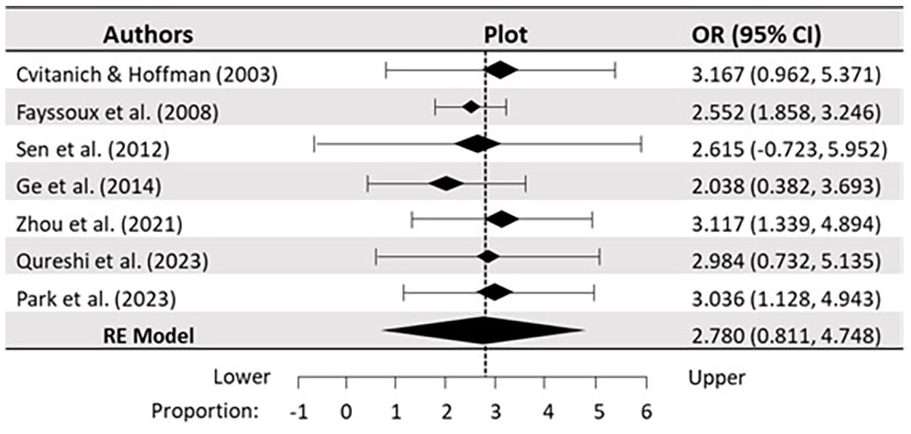
Forest plot for a postoperative satisfactory outcome for the CRPP technique in the studied literature. Pooling of studies using random-effects method (REM) with 95% CI. There is a considerable heterogeneity (I 2 = 76.5%) with statistically significant difference (p < 0.05) in the longitudinal comparison of seven studied literatures.
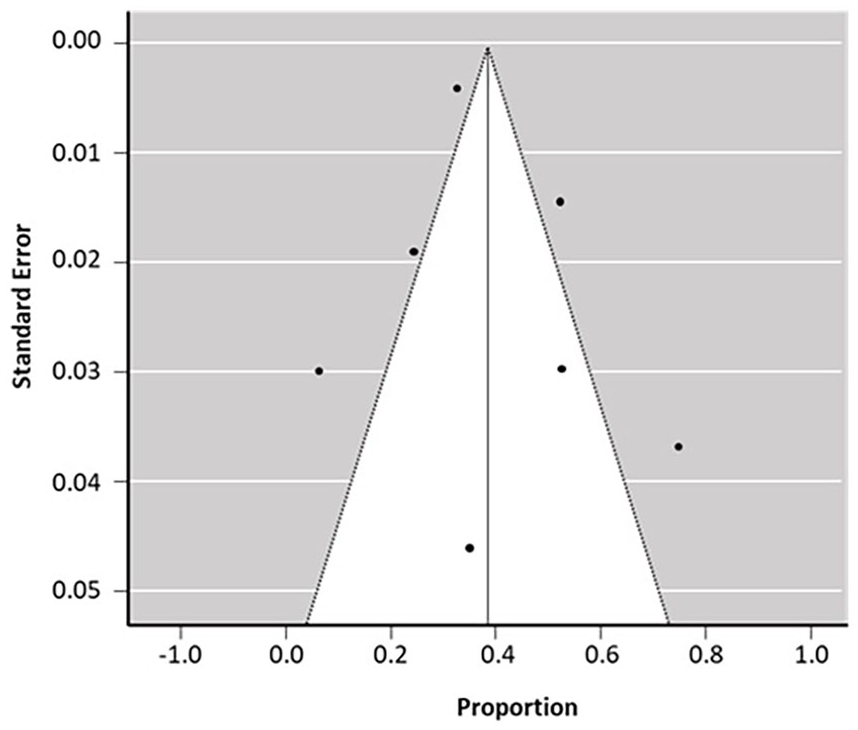
Funnel plot for the postoperative satisfactory outcome of CRPP procedure in seven studied literatures. There is no evidence of publication bias with a symmetrical funnel plot. Rank correlation test and regression analysis for funnel plot asymmetry were statistically significant (r = 0.0748, p = 0.032) for transverse comparison of the studied literature.
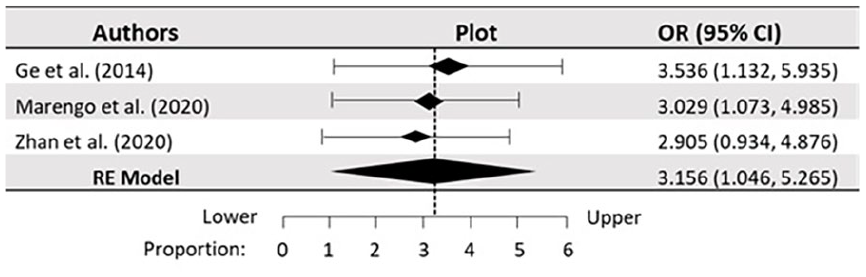
Forest plot for a postoperative satisfactory outcome for ESIN technique in the studied literature. Pooling of studies using random-effects method (REM) with 95% CI. There is considerable heterogeneity (I 2 = 85.9%) with statistically significant differences (p < 0.05) in the longitudinal comparison of the three studied literatures.
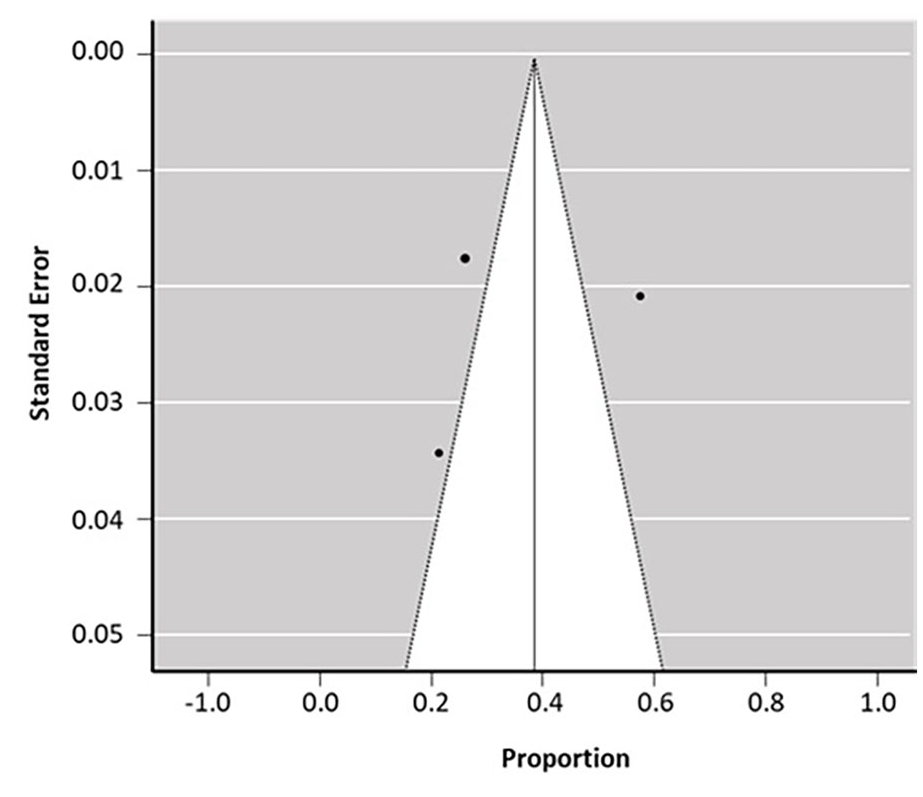
Funnel plot for the postoperative satisfactory outcome of ESIN technique in three studied literature. There is no evidence of publication bias with a symmetrical funnel plot. Rank correlation test and regression analysis for funnel plot asymmetry were statistically significant (r = 0.1574, p = 0.011) for transverse comparison of the three studied literatures.
The higher rate of complications observed in this study was cubitus varus in 19/30 complications (63.3%), most of them were observed in CRPP group 14/129 cases (10.9%) in seven articles, followed by conservative treatment group in 3/9 cases (3%) in one article, then ESIN group in 2/53 cases (3.77%) in two articles. CRPP had additional complications; of seven articles (129 cases), 11 (8.53%) had fixation loss, 8 (6.2%) had reduced range of motion of the limb, one (0.78%) had radial nerve injury, and another one (0.78%) was refractured (see Table 12).
Incidence of complications of different treatment procedures in the studied literatures.
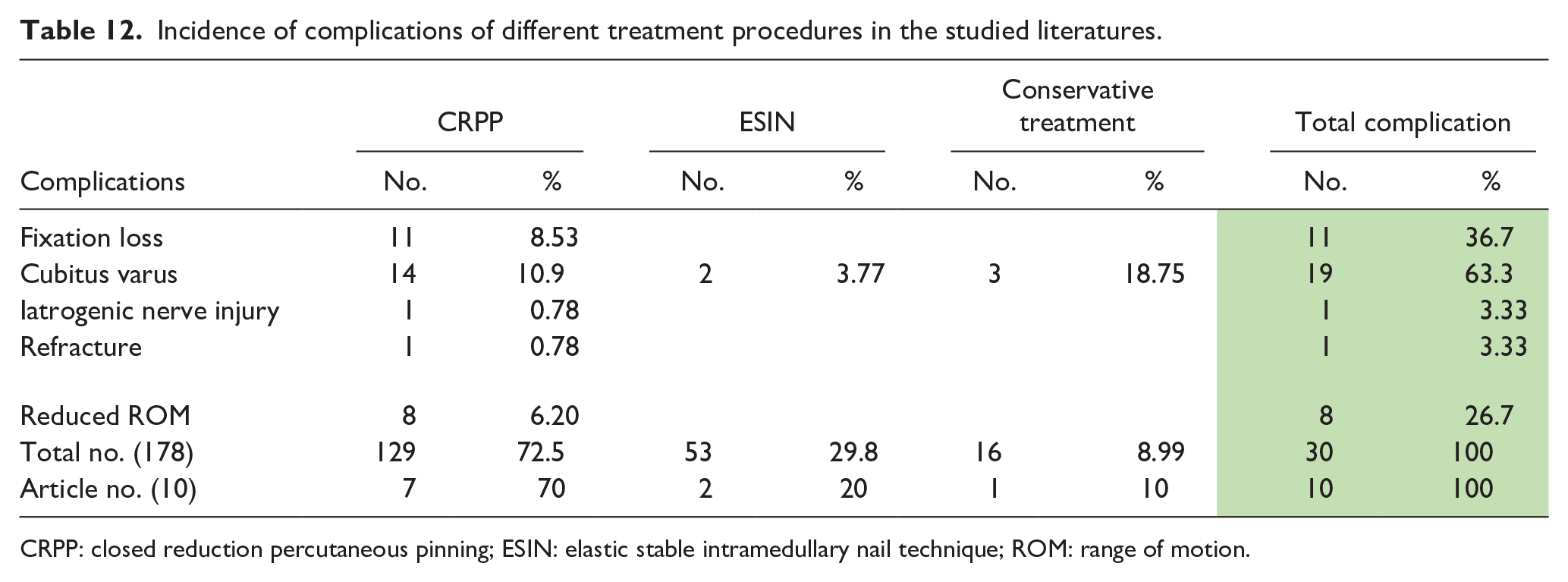
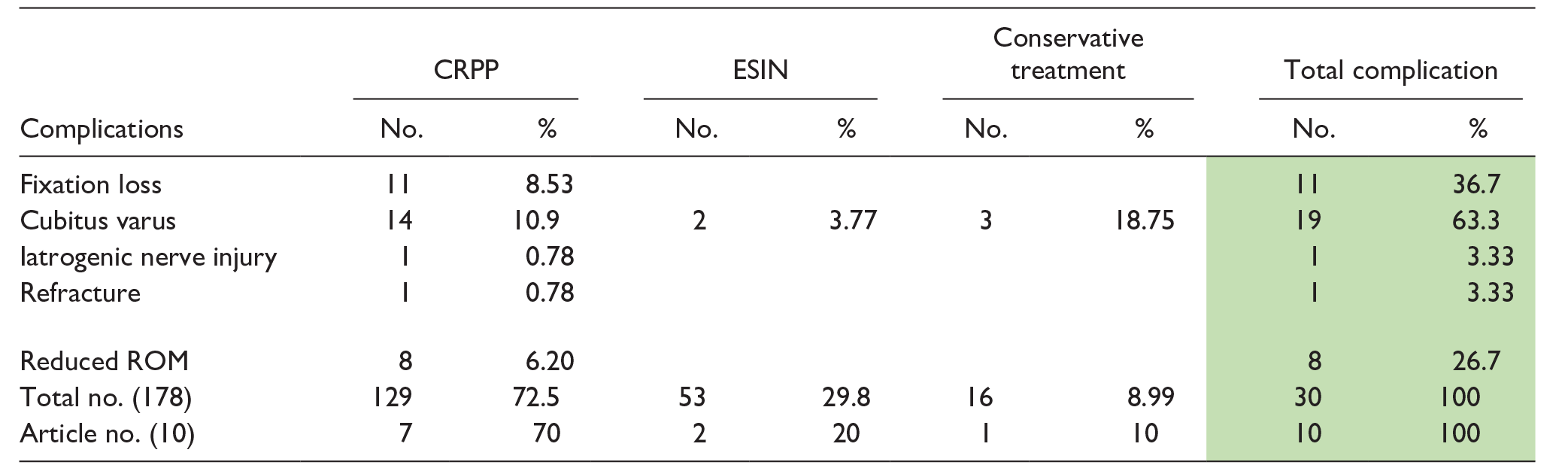
CRPP: closed reduction percutaneous pinning; ESIN: elastic stable intramedullary nail technique; ROM: range of motion.
Discussion
MDJ fractures are rare elbow fractures in children, characterized by their specific location, which is inherently unstable. Unlike humeral supracondylar fractures, MDJ fractures occur in a region with a smaller cross-sectional area and more delicate periosteum. Consequently, MDJ fractures pose unique challenges that are not typically seen when treating standard supracondylar fractures.3,10–18
Remodeling is very limited in the distal humerus fracture compared to the proximal humerus and shaft fractures, as distal humerus physis contribution in growth is very limited, unlike the proximal humerus physis that has a major contribution in growth. 19 Also, remodeling power is minimal in coronal plane deformities (varus/valgus), which are common with MDJ fractures, unlike sagittal plane deformities that lie in the plane of joint movements, that is, flexion and extension. 20
Due to the higher fracture lines in MDJ fractures, the angle at which the pin must cross the fracture is so acute that the pin tip ends up nearly parallel to the inner cortical surface of the opposite cortex. This orientation makes it challenging to achieve proper cortical purchase. 18
In this review, we focused on 10 pieces of literature that met our inclusion criteria to study the efficacy of different management techniques regarding operative difficulties, clinical outcomes, and complications. It is well known that the conventional pinning technique when used for regular supracondylar fractures is very reliable in terms of technical feasibility, adequacy of fixation, early rehabilitation, and less liability of complications such as the need for open reduction, fixation loss, delayed or non-union making it the gold standard for the management of regular supracondylar humerus.
This explains why most authors (7/10 pieces of literature) chose the CRPP technique, however, it was associated with the longest operative time with a mean of 75.47 ± 15.01 SD minutes and the highest incidence of complications; of 129 patients treated with CRPP, 11 (8.53%) had fixation loss, 14 (10.9%) developed cubitus varus, 1 patient refractured, 1 patient developed iatrogenic ulnar nerve injury, and 15 patients had unsatisfactory cosmetic and functional outcome according to Flynn criteria (fair and poor results).3,8–16
This is why concerns have been raised about the trial of different management techniques. ESIN was the second most common technique in 3/10 studied literature, 48 (26.9%) patients. It had the shortest operative time with a mean of 39.7 ± 3.11 min, healing time was a mean of 7.9 ± 1.56 SD weeks, none of the patients developed fixation loss, refracture, iatrogenic nerve injury, only two patients developed cubitus varus in two studied literature. Considering this adequate sample size, we could assume that ESIN is a good alternative technique for the management of MDJ fractures.12,13
Xue et al. 9 in his study used lateral mini plate and assisted K-wire, it was associated with the shortest healing time with a mean of 7.2 weeks, and the study did not report any complications with satisfactory functional and cosmetic outcomes according to Flynn criteria (19 excellent and 2 good). In another literature including six (3.37%) patients, Zhou et al. 14 used a central long intramedullary wire with two cross-pinned wires. This technique carries the advantage of closed reduction as placement of the intramedullary wire first helped maintain the reduction until placement of the cross-pinned wires. The study did not report any complications with excellent outcomes for all six patients according to Flynn’s criteria. However, despite the positive results, this small sample size (six patients) makes it difficult to judge the efficacy of the technique.
Non-operative management has been adopted by two studied literature, Cvitanich & Hoffman 8 and Sen et al., 10 with a total of nine (5.1%) patients. Cvitanich & Hoffman in their study reported that 3/4 (75%) cases developed cubitus varus, while Sen et al. reported only 1/6 cases developed cubitus varus and a very long healing time with a mean of 12 weeks. In a review of these results, which show a high degree of heterogeneity, we could not judge the efficacy of conservative management.
Our systematic review and meta-analysis analyze different techniques used for the management of pediatric distal humerus MDJ fracture. Before 2008, there was no clear definition for MDJ fractures until Fayssoux et al. 3 did their study. Since then, many authors tried different techniques. To the best of our knowledge, until this moment, there is no gold standard technique for management of MDJ fractures.
We performed electronic research through the available online databases, 10 studies with a total of 178 patients met our inclusion criteria; 7 studies performed CRPP, 3 studies performed ESIN, 2 studies conservative management, one study performed lateral mini plate, and one study performed two cross pinned wires with third IM wire. We performed data extraction from the 10 studies and did statistical analysis. We found that the conventional CRPP method used for regular supracondylar humerus fracture is associated with the longest operative time due to difficulties in obtaining adequate bone purchase and maintaining reduction, also it was associated with the highest incidence of complications such as loss of reduction, ulnar nerve injury, cubitus varus, and decreased range of motion.
Three studies used ESIN techniques, none of the participants developed any complications except for two cases that developed cubitus varus and it was associated with the shortest mean operative time. Two studies used conservative management, cubitus varus developed in 3/4 cases in one study and 1/6 cases in another study. One study reported a very long healing time with a mean of 12 weeks and a prolonged rehabilitation period. One study performed lateral mini-plate, showed the shortest healing time, and none of the complications were reported. Another study was done on two cross-pinned wires with a third IM wire, it reported no complications with excellent outcomes. However, we could not judge the efficacy of a technique tried only in one study with a small sample size.
This study has some flaws. First, because of the rarity of literature, our search strategy was diverse; six studies were retrospective observing one technique and four studies were retrospective comparing two different techniques; also we included two English translated literature and the time frame of the study was wide; the oldest literature published in 2003. Second, the results data extracted from the literature show heterogeneity. Third, there is no single definition for healing time, some literature depended on radiological consolidation, and other studies depended on wires removal and return to activity. Fourth, we could not include the effect of fracture patterns on the outcome due to the lack of data in most literature. Fifth, the large difference in sample size between different techniques limits the statistical power and the study strength.
Conclusion
Pediatric distal humerus MDJ fractures should be distinguished from the more prevalent supracondylar humerus fractures. CRPP is associated with poor outcomes, higher incidence of complications, and increased both operative and healing times. On reviewing the adequacy of sample size and raw data of the three studied literature that used ESIN, we conclude that this technique is a reliable method of fixation when technical feasibility is available. We recommend further studies on nonoperative management, mini plate, and cross-pinning with intramedullary wire.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241262169 – Supplemental material for Management of pediatric distal humerus metaphyseal–diaphyseal junction fracture: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521241262169 for Management of pediatric distal humerus metaphyseal–diaphyseal junction fracture: A systematic review and meta-analysis by Ahmad Saeed Aly, Ahmed Mohsen Mohamed and Mohamed Ahmed AL Kersh in Journal of Children's Orthopaedics
Footnotes
Author contributions
A.S.A. conceived and designed the study, and collected data. A.M.M. was involved in literature search, and to manage cases. M.A.A.K. contributed toward acquisition, analysis, and interpretation of data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.