
Abstract
Objective:
To investigate the application of modified elastic intramedullary nail and the outcomes between modified elastic stable intramedullary nailing and traditional elastic stable intramedullary nailing in children with distal tibial metaphyseal junction fracture.
Methods:
A retrospective study was conducted. From January 2018 to January 2021, a total of 36 children with distal tibial metaphyseal junction fracture were treated in our hospital. All of them were treated with closed reduction and elastic stable intramedullary nailing internal fixation. A total of 18 children were treated by modified elastic stable intramedullary nailing and 18 children were treated by traditional elastic stable intramedullary nailing. Postoperative imaging, clinical efficacy, and complications were analyzed.
Results:
The mean follow-up time was 20 (15–36) months in modified group and 22 (16–33) months in traditional group. There were no complications such as infection, loss of reduction, and unequal length of lower limbs in modified group while loss of reduction occurred in two cases in traditional group. In these two cases of loss of reduction, we preformed manual reduction and replacement of long leg casts, and there was no loss of reduction, and the patient achieved a good prognosis. In the last follow-up, American Orthopaedic Foot & Ankle Society score was used. In modified group, excellent outcome achieved in 17 cases, good outcome achieved in 1 case, and satisfactory therapeutic effect was achieved. In traditional elastic stable intramedullary nailing group, excellent outcome achieved in 14 cases, and good outcome achieved in 4 cases. There was no statistical difference in the scores between the two groups.
Conclusion:
It was concluded that modified elastic stable intramedullary nailing fixation is a safe and effective treatment.
Keywords
Introduction
Tibial fracture is one of the most common long bone fractures in children, accounting for about 15%. In addition, it is the second most frequent bone fracture that necessitates hospitalization. 1 For tibia fracture, most children only need to perform closed reduction and plaster fixation for 6–8 weeks which could achieve satisfactory outcome. For difficult circumstances such as failure of closure reduction, open fracture, and combined neurovascular injury and fracture nonunion, surgical therapy should be taken into consideration. At present, the preferred method of therapy for pediatric tibial shaft fractures is elastic stable intramedullary nailing (ESIN).
The diverging “C” shape’s six points might be used to produce an intramedullary splint that would provide biomechanical stability against bending, rotation, axial, and transverse. This technique offers the benefits of being minimally invasive, simple operation, hastening the healing of the fracture, and fewer complications.
However, there is a special type of tibial fracture in children known as distal tibial diaphyseal metaphyseal junction (DTDMJ) fracture, which is extremely challenging to treat due to its site close to the ankle joint and epiphyseal plate. DTDMJ was defined according to AO child fracture classification: a large square was made with the distal tibia-fibula epiphysis plate as the bottom side, and a small square was made with the distal tibial epiphysis plate. The tibial area beyond the intersection of the squares was called DTDMJ.2,3 Theoretically, the traditional ESIN double “C” shape internal fixation strength is unreliable for fractures in this region, since the “C” shape pre-bending region cannot obtain adequate internal support for DTDMJ fractures. As a result, unfavorable outcomes such as loss of reduction and even fracture re-displacement are more likely to occur. On the basis of the traditional double “C”-shaped ESIN, we made a simple improvement, that is, the intramedullary nails were not curved, but only crossed at the proximal tibia once; they now diverge instead of crossing at the distal tibia. In this study, we hypothesized modified ESIN technique was a good choice to treat DTDMJ fractures. We aim to provide a modified ESIN technique to investigate whether good postoperative outcome was achieved in children with DTDMJ fractures.
Patients and methods
A retrospective study was conducted on 36 children with DTDMJ fracture treated in our medical center from January 2018 to January 2021. All patients except for those with open fractures undergo manual reduction followed by surgical treatment if there is still a tendency of displacement. Pediatric patients with open fractures also undergo surgical treatment. All surgeries were performed by the same surgeon specialist. All patients were treated with closed reduction and ESIN internal fixation. A total of 18 children were treated by modified ESIN and 18 children were treated by traditional ESIN. In modified group, 11 of them were male and 7 were female. The age ranges from 5 to 14 years old, with an average of 9.5 years old. In traditional group, nine of them were male and nine were female. The age ranges from 6 to 14 years old, with an average of 10 years old. Patients with open fractures were excluded from the study. All patients were followed at least 12 months. Postoperative imaging, clinical efficacy, and complications were analyzed. AOFAS scores were recorded in the last follow-up.
Surgical procedure
Traditional ESIN technique was same as reported by Metaizeau et al. 4 The treatment procedure in modified group is as follows. The surgical diagram of the fracture fixed by modified elastic intramedullary nail was shown in Figure 1.
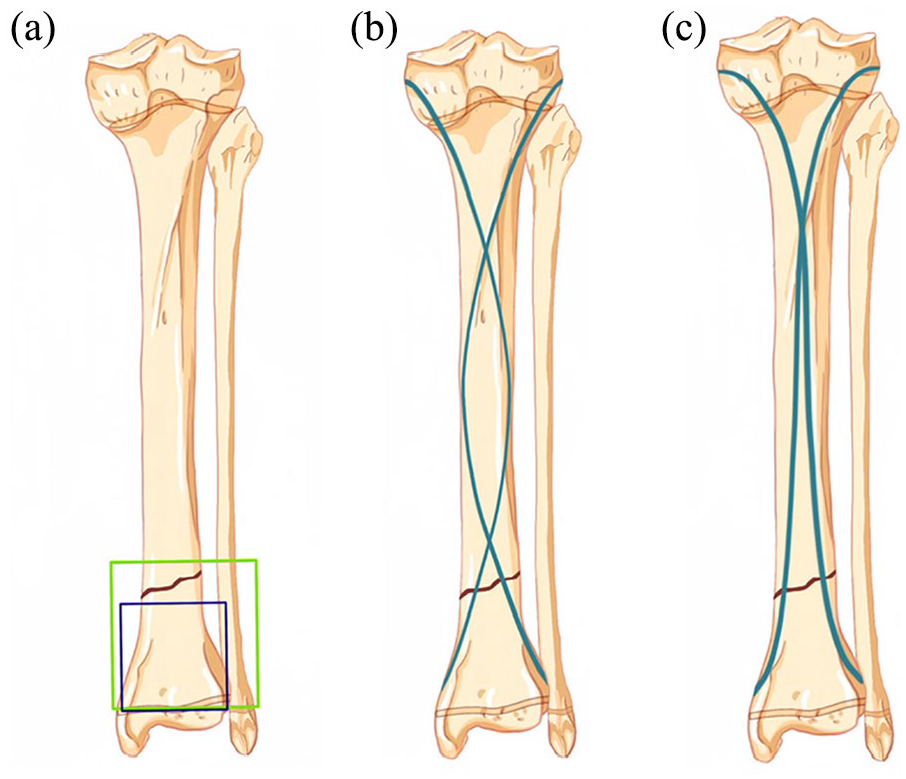
Diagram of distal tibial metaphyseal junction fracture. A large square (green) was made with the distal tibia-fibula epiphysis plate as the bottom side, and a small square (blue) was made with the distal tibial epiphysis plate. (a) Surgical diagram of the fracture fixed by traditional (b) and modified elastic intramedullary nail (c).
After satisfactory anesthesia (general anesthesia), the patient was placed in supine position. The affected limb skin was routinely disinfected and sterile sheets were laid. Tourniquet is usually not required. The ESINs (Forwos Medical, SNZ-01, Chongqing) with the narrowest diameter of 40% were selected including diameters of 2.5, 3, and 3.5 mm. During the operation, the insertion point was located and marked under C-arm fluoroscopy. A 2-cm longitudinal incision was made in the medial and lateral of proximal tibia, respectively, and a bony tunnel was created on both sides of the epiphysis at the 2 cm away from the proximal tibial epiphysis plate. The bone awl was angled with the tibial shaft at 45°. The pre-bent ESIN was inserted anteriorly from the proximal site. Under the guidance of C-arm fluoroscopy, two ESINs were inserted into the bone and stop at the proximal of fracture site. The surgeon reduced the fracture under traction of assistant. If reduction is difficult, Kirschner wire can be used to assist the reduction, or rotation of the intramedullary nail head can improve the reduction effect. After satisfactory reduction, two ESINs passed through the fracture site, and two ESINs were scattered at the distal end of the fracture and stick to the wall of the distal bone so that it could achieve compression support and fixation. When the tip of nail crossed the fracture, the nail was rotated to obtain an S-shaped fixation. The nails stopped at 0.5 cm proximal to the distal epiphyseal plate to avoid damage to the epiphyseal plate. The end of ESIN was bent and cut short, placed under the fascia, and the appropriate length was reserved for easy removal. The incision was sutured with absorbable thread and bandaged. After the operation, the cast of the affected limb was fixed with a long leg cast, and the tubular gypsum was replaced 2 weeks after the operation. The long leg cast was replaced by the short leg cast postoperative 3 weeks. We used a long leg cast with 90° of ankle dorsiflexion and 5°–10° of knee flexion. X-ray films were reviewed 6–8 weeks after the operation, and whether the cast was removed or not was determined according to the fracture healing. After the cast was removed, the patients were instructed to do active and passive functional exercise and ground loading. X-rays were repeated 3 and 6 months after the operation, and the clinical efficacy and complications were recorded. ESIN was removed 8–10 months after the fracture healed. Subsequently, the patients were reviewed once every 6 months to assess the presence of unequal lower limb deformity (Figure 2).
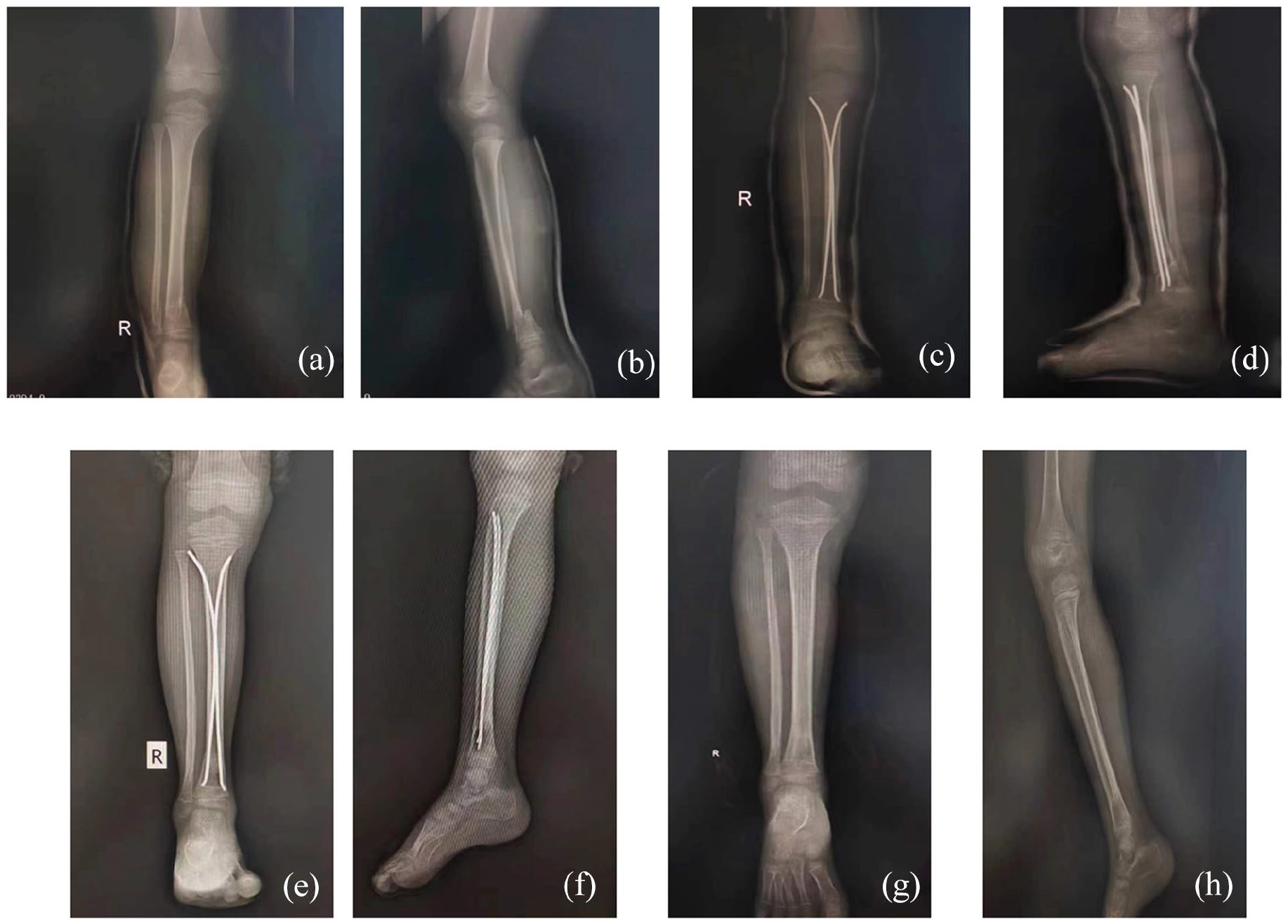
Preoperative X-rays of a 7-year-old boy with open distal tibial metaphyseal junction fracture after a fall (a, b). Immediate postoperative anteroposterior (c) and lateral (d) X-ray views showing closed reduction with modified elastic intramedullary nail fixation. At 6-month (e, f) and 1-year (g, h) follow-ups after surgery, respectively, the affected tibia is observed by X-rays with a satisfactory outcome.
Statistical analysis
The Prism software (Prism 8.0.2) was used to perform statistical analysis. Normally distributed test was tested by D’Agostino-Pearson test. If the data were normally distributed and the variance was homogeneous, it was expressed as axis. The unpaired T-test was used for comparisons in two groups. If it did not conform to normal distribution, it was represented by M (Q1, Q3) and Wilcoxon test was used. p < 0.05 was considered statistically significant.
Results
From January 2018 to January 2021, a total of 36 patients with DTDMJ fractures were treated in our hospital. The mean follow-up time was 20 (15–36) months in modified group and 22 (16–33) months in traditional group. The average age of the modified group was 9.5 ± 2.358 years. The average age of the traditional group was 10 ± 2.058 years. There was no statistical difference in age between two groups. There were no complications such as infection, loss of reduction, and unequal length of lower limbs in modified group while loss of reduction occurred in two cases in the traditional group. At last follow-up, AOFAS score 5 was performed. In modified group, excellent outcome achieved in 17 cases, good outcome achieved in 1 case, and satisfactory therapeutic effect was achieved with an excellent and good rate of 100% (Table 1). In traditional ESIN group, excellent outcome achieved in 14 cases, and good outcome achieved in 4 cases (Table 1). Loss of reduction happened in traditional group. Two weeks after operation, the swelling was relieved and the cast was loose. Angular displacement happened at the fracture site. After manual reduction, the long leg cast was replaced for 6 weeks and the position was satisfactory at the final follow-up. The AOFAS score in modified group was 98 (95, 100). The AOFAS score in traditional group was 98 (95, 99.25). There was no statistical difference in the scores between the two groups.
Outcomes assessed with AOFAS score in modified group and traditional group.
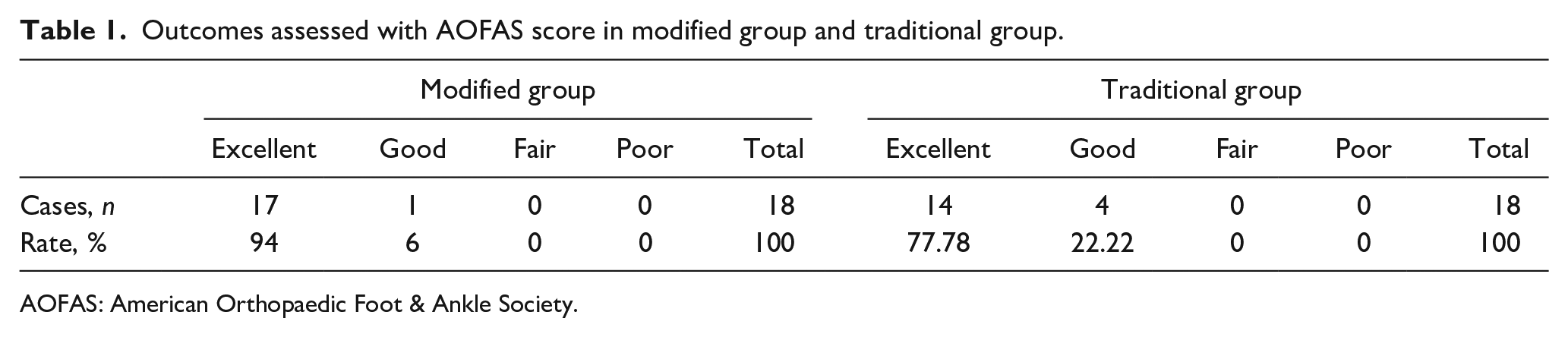
AOFAS: American Orthopaedic Foot & Ankle Society.
Discussion
DTDMJ fracture is relatively rare. It has been reported that incidence of DTDMJ fracture ranges from 0.35% to 0.45%. 6 In our hospital, the number of mid-shaft tibial fractures in children is about 70 per year. Due to its special anatomical structure, less local muscle, poor blood supply, close to the ankle joint and epiphyseal plate, and often associated with fibula fracture, if not properly handled, it might lead to ankle deformity and dysfunction and other adverse consequences. However, the treatment methods of such fractures have been reported in relevant literature, including traditional manual reduction and plaster fixation, Kirschner wire fixation, ESIN, rigid intramedullary nail, steel plate, and external fixator. However, due to the particularity of fracture, the optimal treatment plan is still not unified, and remains controversial. With the rapid development of minimally invasive technology, especially for special groups such as children, it becomes more increasingly significant. Kirschner wire is a common fixation method for proximal joint fractures in children. Kirschner wire in the treatment of distal tibial fracture was found that the fixation is simple and safe, besides the advantages including small trauma, quick postoperative recovery, satisfactory fixation effect, and the Kirschner wire is easy to remove. 7 However, fixation of Kirschner wire needs to pass through the distal epiphyseal plate of the tibia, especially in repeated penetration, which increases the risk of epiphyseal plate injury and leads to ankle deformity. Moreover, for DTDMJ fractures, the insertion angle of the Kirschner wire is required to be steeper and the operator is required to have higher technical requirements. Otherwise, effective fixation cannot be achieved and the learning curve is long. Ilizarov external fixator could achieve multi-plane fixation of 3D structure, with good stability, and it could achieve the advantages of minimally invasive treatment. Besides, the insertion nail can be used to assist the reduction during the operation. 8 However, the postoperative care is demanding, inconvenient to wear, and problems such as the needle tract infection and expensive still exist. 9 The application of plate in the treatment of distal tibial fractures can overcome the shortcomings of ESIN fixation stability, achieve effective and strong internal fixation, provide sufficient biomechanical strength, and reduce the risk of nonunion without excessive dissection of the periosteum. 10 There is no need for external fixation after operation, and early functional exercise is conducive to rehabilitation. However, due to the fracture line is close to the epiphyseal plate in DTDMJ fracture, the risk of iatrogenic epiphyseal plate injury still exists while increasing the effective fixation distance of the plate. Moreover, plate removal is more traumatic, and plate stress shielding leads to an increased risk of re-fracture after implant removal. Rigid intramedullary nail might increase the risk of iatrogenic epiphyseal plate injury and patients older than 14 years old with DTDMJ fractures can benefit from rigid intramedullary nailing.
In view of the limitations of the above methods, ESINs can be a good choice to treat with DTDMJ fractures. The application of ESIN has been described by Prévot et al. 11 and the emergence of traditional techniques by Metaizeau et al. 4 has brought about earth-shaking changes in the minimally invasive treatment of long bone fractures of limbs in children. The benefits of ESIN include elastic fixation, minimally invasive, simple operation, and speedy recovery. It has become the preferred option for the treatment of tibial shaft fractures in children. 12 Traditional ESIN double “C” internal fixation has become the first choice for children with long diaphysed bone fractures. In our study, both traditional and modified ESINs achieved good outcomes for DTDMJ fractures. However, it should be noticed that for DTDMJ fractures, the role of ESIN three-point fixation was not effective. So, it might increase the risk of insufficient fixation after reduction, leading to reduction loss, fixation instability, and other adverse consequences. In our study, loss of reduction and fixation instability occurred in two cases of traditional ESIN group. In this group of cases, the traditional double “C”-shaped ESIN was simply modified. ESIN only crossed once in the proximal tibia and dispersed at the distal end, which increased the effect of compression support and fixation after fracture reduction with better stability, and achieved satisfactory curative effect. Although the theoretical basis of ESIN is to achieve three points of support for intramedullary nailing, traditional techniques could not provide effective support for the fracture area of DTDMJ. Besides, the fixation strength is not enough, which is easy to cause reduction loss or fracture re-displacement. In view of this, we carried out a simple modification on the basis of the traditional ESIN, only crossing the proximal tibia once, and diverging the distal tibia, theoretically increasing the compression support fixation strength of the DTDMJ fracture area, and achieved satisfactory clinical treatment results. No cases of re-displacement or reduction loss were found after the operation. The same method has been reported by Harly et al., a total of 13 patients with DTDMJ fracture achieved good therapeutic effect. 13 In terms of stability, we use this method to play a pressurized support role, without increasing the amount of ESIN. Although there was no statistical difference in the scores between the two groups, it has been found that loss of reduction happened in traditional ESIN group which suggested that modified ESIN might solved this nodus of DTDMJ fracture. In addition, for older children with high body mass index, the rate of fracture re-displacement is higher. For DTDMJ fracture, some cases might require traditional ESIN technique to cross the distal epiphyseal plate to increase its stability. Although there is no clinical evidence of adverse consequences from epiphyseal plate injury, the risk of epiphyseal plate injury should not be ignored. 14 In our study, we did not choose to cross epiphyseal plate to reduce the risk of epiphyseal plate injury. Remarkably, we need to point out that although the theory of modified ESIN keeps the advantages of traditional technology including minimally invasive, safe, fixed with flexibility, and a divergent ESIN pressure, cast support should be provided. Besides, it has been reported that stabilization of associated fibula fractures did not significantly impact the clinical, radiographic, and pedobarographic outcomes of the children with displaced distal tibial metaphyseal fractures who were surgically treated. 15 In our opinion, it should be noted that if there is no shortening or angulation deformity of the fibula after reduction and fixation of the tibial fracture, internal fixation is not necessary, only cast support is applied. If there was shortening or angulation deformity of the fibula after reduction and fixation of the tibia, we performed internal fixation with Kirschner wires or flexible medullary nails to achieve stability.
In our study, casting is necessary and it is used for 6 weeks after surgery. For DTDMJ fractures, ESIN cannot achieve strong internal fixation, and two to three ESINs from different directions are required to increase fixation strength if necessary. Due to the natural hyperactivity of children, postoperative tube cast fixation is still very important. The stability of ESIN can be improved by increasing the amount of ESIN, and the treatment effect of ESIN is satisfactory. 16 It has been found that four ESINs were directly used to treat distal tibial fractures in children. The stability of the fracture area was increased and there was no external fixation with plaster after operation, and immediate weight bearing was allowed, and good treatment effect was achieved. 17 Since only two ESINs were used, we thought postoperative cast and tube-type cast fixations are still crucial. In addition, cast fixation can not only control pain, but also be necessary if fibular fracture is involved. For the cases without fibular fracture, because the fracture is close to the distal end, and the fixation is not rigid fixation, combined with the poor compliance of postoperative management of children, the cast fixation has little impact on the joint, and we assisted with cast fixation to prevent displacement.
The limitations of this study are the small number of cases and retrospective study. Since the DTDMJ fractures are rare in pediatric orthopedic, randomized controlled trial study with large samples is needed to confirm the effectiveness of this method in future. In addition, biomechanical studies also need to be performed to demonstrate the stability of modified ESINs. Besides, our study included patients younger than 14 years of age, a relatively wide age range, and future studies with smaller age range are needed to investigate treatment effects. At the same time, we only evaluated radiographic healing at the last follow-up. Future studies need to be improved.
Conclusion
The modified ESIN has achieved satisfactory results in DTDMJ fractures. There were no postoperative complications such as infection, loss of reduction, and unequal length of lower limbs, and the ankle function of the affected limb was satisfactory at the last follow-up. Although there may be several ways to achieve such a favorable outcome, we believe that closed reduction with modified ESIN is a viable treatment option for distal tibial epiphyseal junction fractures in children.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241242251 – Supplemental material for Modified elastic intramedullary nail internal fixation for distal tibial metaphyseal junction fracture
Supplemental material, sj-pdf-1-cho-10.1177_18632521241242251 for Modified elastic intramedullary nail internal fixation for distal tibial metaphyseal junction fracture by Wanlin Liu, Zhenqun Zhao, Rui Bai and Chenyang Meng in Journal of Children’s Orthopaedics
Footnotes
Acknowledgements
The authors are very grateful for the guidance and assistance of professor Darko Antičević who provided throughout the research process.
Author contributions
W.L., Z.Z., C.M., and R.B. carried out the studies, participated in collecting data, and drafted the manuscript. C.M. and R.B. performed the statistical analysis and participated in its design. W.L., Z.Z., C.M., and R.B. participated in acquisition, analysis, or interpretation of data and drafted the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All the children’s families signed consent forms, and the study was approved by the Ethics Committee of Inner Mongolia Medical University (approval no. YKD2021010921).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Inner Mongolia (grant no. 2021MS08024) and the Natural Science Foundation of Inner Mongolia Medical University (grant no. YKD2021MS037).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.