
Abstract
Purpose
Loss of pin fixation in supracondylar fractures can occur with failure to achieve bicortical fixation. Bicortical fixation may be challenging for those pins that attempt to penetrate the diaphyseal cortex, where the bone is thick. Lateral-entry Steinmann pins may allow for better penetration through cortical bone because they are more rigid than typical Kirschner wires.
Methods
A retrospective review of 16 children with type III supracondylar fractures treated by a single surgeon using Steinmann pins was undertaken. The average age at presentation was 6 years. Following closed reduction, all fractures were maintained with three lateral-entry pins. At least one Steinmann pin was placed in the lateral column of the distal humerus in each pin construct.
Results
Follow-up radiographs indicated a mean Baumann's angle of 72.9° (range 64°–82°). There was no statistically significant change in the Baumann's angle or axial alignment at final follow-up. All but one fracture healed in an anatomic position on the lateral view.
Conclusions
Steinmann pins placed through a lateral-entry point are effective in controlling the reduction of high-grade supracondylar fractures. The fixation is excellent and avoids potential ulnar nerve complications of medial entry.
Introduction
Supracondylar fractures are the most common upper extremity fractures in children [1]. Unstable fracture patterns typically require closed reduction and percutaneous pin fixation [2]. Loss of fracture reduction can be associated with three technical errors in pin fixation [3]: Failure to engage both fragments with two or more pins Failure to achieve bicortical fixation Failure to achieve adequate pin separation at the fracture site
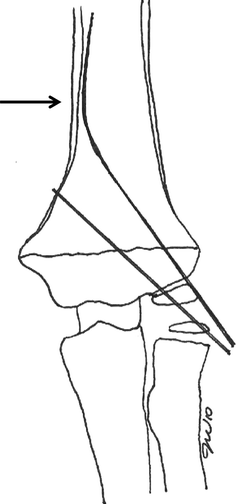
Failure to achieve bicortical fixation can occur when a Kirschner wire attempts to penetrate the thick cortical wall of the medial diaphysis (arrow). The wire bends and becomes intramedullary
In order to avoid the type B error, larger diameter Steinmann pins may be beneficial. The additional stability of a larger pin contracting to stabilize supracondylar humerus fractures has been previously studied [4]. The typical size of the pins used for the fixation of supracondylar fractures is 1.6 mm (1/16 inch) diameter. Increasing the diameter of the third, most lateral pin, to 2 mm or 2.5 mm in diameter may allow for rigid fixation of the shaft of the humerus at the far side. This stronger pin theoretically allows for better penetration and fixation in the thicker bone of the distal humerus shaft. This is particularly important in unstable fracture patterns, especially in larger or older children. We retrospectively reviewed our experience with lateral-entry Steinmann pins in the treatment of displaced pediatric supracondylar fractures.
Methods
Children with significantly displaced supracondylar humerus fractures who presented to a tertiary care pediatric hospital between July 2007 and July 2009 were identified. Patients who underwent closed reduction and percutaneous pinning of closed extension type III supracondylar fractures by a single surgeon (JW) were included in the study. Children with closed physes, open fractures, and flexion-type supracondylar fractures were excluded. Those fractures that required open reduction were also excluded. This study was approved by our medical school institutional review board.
Demographic information was collected on each patient, including age and gender at surgery. Operative reports were reviewed to identify the number of Steinmann pins used in each case.
Following closed reduction of the supracondylar fracture, fracture stabilization was achieved using a lateral-entry three-pin configuration [2]. A 1.6-mm K-wire was placed first, just lateral to the olecranon fossa. In the described three-pin lateral construct, the first pin placed was in the most medial position. Depending on the surgeon's preference, a second K-wire or Steinmann pin was placed just lateral to the first pin. At least one of these pins crossed through the central column (olecranon fossa) [5]. The third and most lateral pin in each case was a Steinmann pin placed into the lateral column. The Steinmann pin entered the distal humerus with full speed on forward drive of the power drill. Once the Steinmann pin abutted the far cortex, the power drill was placed in reverse. With a gentle push, the pin would penetrate the far cortex, instead of becoming intramedullary.
All pins were placed with bicortical fixation in either a parallel or divergent fashion, so as to have a pin spread of more than 2 mm at the fracture site. Once fracture fixation was complete, the stability of the fracture was checked using fluoroscopy [6].
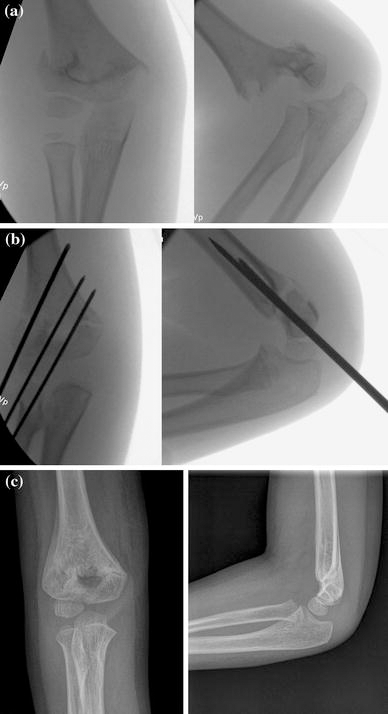
The reduced fracture was imaged using a technique with the arm stationary on a hand table and the flouroscopy tube was moved to obtain anteroposterior (AP) and lateral views (Fig. 2), as described by Leitch et al. [7]. This technique minimizes the loss of reduction in unstable supracondylar fracture patterns, as the extremity is moved from AP to lateral positioning. Additionally, this method facilitates the placement of a large pin in the humerus of a small child while using the lateral view to maintain the pin between the anterior and posterior cortices. This may be particularly helpful in a teaching setting.

A long-arm bivalved cast was applied over the sterile dressing with the elbow in 90° of flexion and the forearm in neutral rotation. The fluoroscopic images were saved for comparison with postoperative radiographs.
Patients were typically discharged on the first postoperative day and returned for clinical and radiographic examination 1 week later. Repeat films were obtained at the 4-week postoperative visit, prior to removal of the cast and pins. When acceptable healing had been achieved, the pins were removed and motion was encouraged. Clinical evaluations at the final visit 4 weeks post pin removal were conducted as described by Flynn et al. [8]. Radiologic assessments were conducted at the time of wire removal and at final follow-up on AP and lateral views. Postoperative AP and lateral radiographs were compared with those taken at the time of wire removal and at final follow-up. Baumann's angle [9] and the relation of the anterior humeral line to the capitellum [10] were recorded. When the anterior humeral line intersected the capitellum, a score of “0” was given. When the capitellum was posterior to this line (extended), it was scored “−1”. Anterior positioning (flexed) was scored “+1”. Axial malalignment was also noted clinically and radiographically.
Statistical analysis using SPSS version 18.0 was used to assess changes in Baumann's angle. A P value <0.05 was considered to be statistically significant.
Results
Sixteen children were identified with closed type III extension supracondylar fractures during the study period. All patients were treated with at least one lateral column Steinmann pin. The average age at presentation was 6 years (range 22 months–9 years). There were 11 boys and 5 girls. All children had three pins placed in a parallel or divergent pattern. One or two Steinmann pins were utilized in each pin configuration (median: one Steinmann pin).
All pins were removed in the office without any complications at 4 weeks postoperatively. There were no wound infections noted in this series. None of the patients presented with limited elbow motion at final follow-up. There were no neurovascular injuries before or after surgery. No patient returned to the operating room for fracture remanipulation before healing. Clinically evident carrying angle, epiphyseal, or elbow hyperextension deformities were not observed in any case at the last follow-up.
Intraoperative AP and lateral radiographs were compared to those taken at 4 weeks postoperatively (Fig. 3). The mean Baumann's angle (±standard deviation [SD]) was 72.56 ± 5.77° (range 64°–82°) immediately after surgery, and 73.37 ± 5.82° at 4 weeks postoperatively (Table 1). There was no statistically significant change in the Baumann's angle at the 4-week visit (P = 0.62).
Data summary
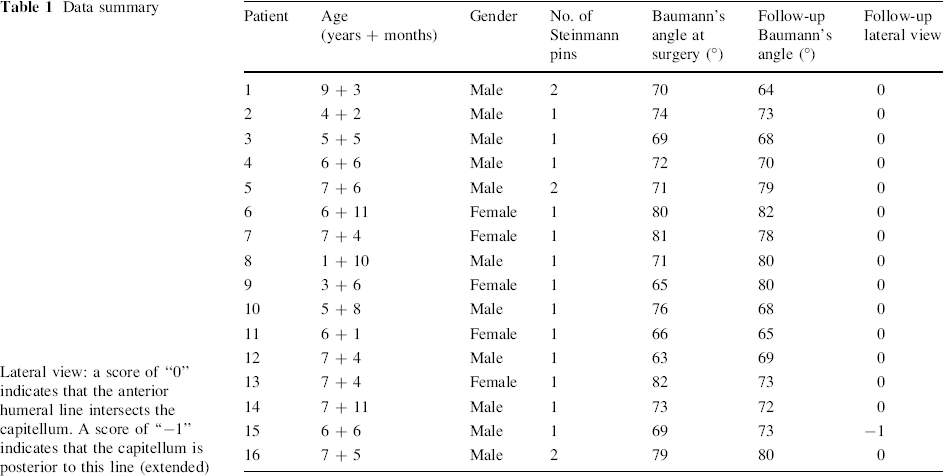
Lateral view: a score of “0” indicates that the anterior humeral line intersects the capitellum. A score of “−1” indicates that the capitellum is posterior to this line (extended)
No axial plane changes were noted clinically or radiographically upon the assessment of intraoperative and final imaging studies. On the final lateral radiographs, all patients except one had a score of “0” for the relationship of the anterior humeral line to the capitellar epiphysis, indicating anatomical reduction. This patient had slight extension of the distal fragment, but no significant range of motion limitation.
The clinical outcomes of all patients at the final follow-up visit were evaluated using the cosmetic and functional criteria of Flynn et al. [8]. According to these cosmetic criteria, all patients achieved a satisfactory outcome.
Discussion
Supracondylar humeral fractures are the most common elbow fractures in children and represent 65.4% of pediatric upper extremity fractures [1]. Optimal fracture fixation in displaced pediatric supracondylar humerus fractures creates a construct that is stable enough to resist axial rotation, as well as flexion, extension, varus, and valgus displacement of the distal fragment. The ideal construct can avoid postoperative deformity, which is reported to be as high as 17% [2].
Although closed manipulation and percutaneous Kirschner wire stabilization is the gold standard for the management of displaced supracondylar fractures of the humerus in children, the optimal pin configuration is still not clear [2]. Biomechanical studies have shown that crossed pinning provides a more stable configuration, especially against torsional loading, yet, the medial pin can be associated with iatrogenic ulnar nerve injury (1–6%).
Retrospective and prospective clinical studies have established the effectiveness of lateral-entry pin fixation alone for the treatment of supracondylar fractures of the humerus in children. These studies have confirmed that lateral-entry pin fixation provides adequate fracture stabilization while avoiding the risk of ulnar nerve injury. Surgeons who choose to use lateral-entry pins alone must be aware that adequate stabilization, while equally effective, requires attention to detail.
Three laterally placed pins are recommended for type III supracondylar fractures, especially in larger and older children. Sankar et al. [3] reported no loss of fixation in fractures fixed with three lateral-entry pins as compared to 16.7% loss of fixation in type III fractures fixed with two pins. Skaggs et al. [11] similarly reported no loss of fixation following the use of three lateral-entry pins for the fixation of extension type II and III supracondylar humeral fractures of the distal humerus.
According to Sankar et al. [3], the loss of fixation was due to a technical error associated with pin placement at the time of the initial procedure. They identified three types of error: type A error was defined as the failure to engage both fragments by two pins or more; type B error as the failure to achieve bicortical fixation with two pins or more; type C error as inadequate pin spread (<2 mm at the fracture site) to control rotation.
Diederichs et al. [12] reported that the medial cortex of the distal humerus is thicker and has greater trabecular bone density than the lateral cortex. Hence, a standard 1.6-mm lateral-entry Kirschner wire may bend due to its flexibility when it hits the medial cortical wall. Instead of penetrating through the bone, it skives along the cortex, stays inside the tube of bone, and becomes intramedullary. A pin in this position provides poor fixation, as it has only penetrated through one cortex of bone.
Srikumaran et al. [4] compared the use of larger diameter (>1.8-mm) to smaller diameter pins (<1.8-mm) in the stabilization of supracondylar humeral fractures and concluded that larger pin diameters may provide better stability and sagittal alignment, but may be associated with a higher rate of infection.
The primary limitation of this study is the small sample size. Furthermore, this study is retrospective in nature and represents the experience of one surgeon. Longer follow-up will be required to determine whether a larger diameter smooth pin can cause any growth disturbances in the distal humerus.
The pin configuration described addresses the type B error [3] by using a larger sized (2- and 2.5-mm) Steinmann pin as the lateral most pin. There was also no loss of AP reduction between the intraoperative and postoperative periods. We feel that the use of the lateral-entry Steinmann pin improved the stability of the fixation. This was not associated with an increased risk of pin site infection, difficulty in the removal of the pin in the outpatient clinic, or stress fractures following pin removal.
Steinmann pins placed through a lateral-entry point are effective in controlling the reduction of high-grade supracondylar fractures. The fixation is excellent and avoids potential ulnar nerve complications of medial entry.
Footnotes
Acknowledgments
The authors would like to thank E. O'Brian Smith, PhD (Texas Children's Hospital, Houston, Texas) for his assistance with the statistical analysis.The authors have no financial relationship with the organization that sponsored the research. The authors have full control of the primary data and allow the journal to review the data, if requested.