
Abstract
Purpose:
Septic arthritis of the hip in children and adolescents is a common condition requiring timely diagnosis and intervention. Surgical irrigation and debridement is typically performed through the anterior approach because of concerns about injury to the medial femoral circumflex artery leading to avascular necrosis. While there are multiple studies investigating the sequelae of anterior and medial approaches for reduction of developmental dislocation of the hip, none have compared these approaches for the pediatric septic hip. We hypothesize that there will be no significant difference in the rate of avascular necrosis when comparing the medial and anterior approaches to the septic hip in pediatric patients.
Methods:
A retrospective review was performed of pediatric septic hips treated with irrigation and debridement through either a medial or anterior approach at a single institution over an 18-year period of time. The primary outcome measure was the development of avascular necrosis.
Results:
Thirteen of 164 patients (7.9%) developed avascular necrosis. Avascular necrosis was noted in 9 of 101 patients who had anterior approach and 4 of 63 patients who underwent medial approach (p = 0.76). The average age for patients developing avascular necrosis was 10.0 years old versus 6.8 years old in patients who did not develop avascular necrosis (p = 0.01). The average follow-up was 3.3 years in patients with avascular necrosis versus 1.5 years for patients who did not develop avascular necrosis (p = 0.01).
Conclusion:
Medial approach to the pediatric septic hip does not increase the rate of avascular necrosis compared to the anterior approach.
Level of evidence:
Retrospective comparison study, Level III
Introduction
Septic arthritis of the hip is a common and potentially devastating condition in pediatric patients. It affects approximately 4–8 per 100,000 children per year with peak age ranging from 2 to 6 years old. 1 Prompt diagnosis and emergent interventions are essential for favorable outcomes.1–4 Historically, the anterior approach to the hip has been utilized in part due to surgeon familiarity and in part in order to minimize risk for development of avascular necrosis (AVN). Although there are many studies in the literature addressing the sequelae of various approaches to the pediatric hip as it pertains to developmental dysplasia of the hip (DDH), none have investigated these approaches in patients with a diagnosis of septic arthritis of the hip.5–10
The most commonly used approach to the pediatric hip is the modified Smith–Petersen approach which should not put the blood supply to the femoral head at direct risk, although AVN may occur due to contact forces or extreme positioning of the hip after reduction of DDH. Another approach commonly used in the treatment of DDH is the medial approach. Various medial approaches have been described especially in arthroscopy, with the approach between the adductor longus and pectineus and between pectineus and femoral artery and vein are the most common.11–13
However, a drawback of the medial approach is the potential risk to the blood supply of the proximal femoral epiphysis due to the proximity of the medial femoral circumflex artery (MFCA), the primary blood supply to the femoral head, as it courses posteromedially between the iliopsoas tendon and pectineus.14–17
This study aims to evaluate the incidence of AVN in the anterior and medial surgical approaches to the hip in pediatric patients with septic arthritis of the hip. We hypothesize that there will be no significant difference in the incidence of AVN between the two approaches.
Materials and methods
Study design
After receiving Institutional Review Board approval, we conducted a retrospective review at a single children’s hospital. Patients ages 0–18 years old who underwent irrigation and debridement (I&D) of the hip due to concern for sepsis between 2004 and 2022 were identified. Concern for septic arthritis was defined by at least two of four Kocher criteria or radiographic evidence (i.e. hip effusion on ultrasound or magnetic resonance imaging [MRI]). Patients without postoperative follow-up, those with pre-existing AVN, and those who underwent I&D using an approach other than the anterior or medial approaches were excluded. Need for repeat drainage was deemed necessary if the patient had continued symptoms or maintained inflammatory markers. Concomitant infection was typically diagnosed by an infectious disease physician or hospitalist physician. The database consisted of a total of 181 cases of pediatric septic hip. A total of 17 patients were excluded for inaccessible records, and 17 cases were repeat surgeries in the same hip leaving a final cohort of 147 cases in 143 patients for review. A total of 85 males and 62 females with an average age of 6.7 years old were included in the study. Mean follow-up was 1.6 years (interquartile range [IQR]: 48 days to 2.4 years). Ninety-one hips underwent anterior approach, and 56 hips underwent medial approach. Our primary outcome measure was the development of AVN as determined by radiographic evaluation by an orthopedic surgeon or radiologist. AVN was defined as a range of proximal femur alterations resulting from bony changes in the proximal femoral epiphysis including sclerosis, fragmentation, and collapse.
Each patient underwent open I&D of the hip by one of five pediatric fellowship-trained orthopedic surgeons using an anterior or medial approach. The attending surgeon determined the choice of approach. We defined the anterior approach as any approach lateral to the femoral neurovascular bundle yet medial to the tensor fascia latae. This included the standard anterior approach and the anterolateral approach. Likewise, we defined the medial approach as any approach medial to the femoral neurovascular bundle. This included the medial approach and the anteromedial approach.
The majority of medial approaches were performed in the following fashion. A transverse incision is made at the groin crease overlying the adductor longus. The plane between the adductor longus and pectineus is bluntly dissected. The deeper dissection lies between the adductor brevis and pectineus muscle. If this plane is difficult to identify, it can be verified by noting the anterior branch of the obturator nerve lying on the adductor brevis. At this point, the medial femoral circumflex is frequently encountered passing anterior to posterior along the capsule. The MFCA is located distal to the ideal capsulotomy location. Careful sweeping with a Kittner dissector on top of the hip capsule can further delineate the anatomy before the capsular incision is made. The capsule is incised and a small angiocath is used to irrigate the joint.
Statistical analysis
Cox proportional hazards regression models were used to estimate the association between approach, gender, location of presentation, whether repeat I&D, duration of symptoms before surgery (time from onset of symptoms to surgery), time to surgery (time from hospital presentation to surgery), age, length of stay, and AVN, adjusted for age and gender. Culture data were presented without statistical analysis as there is a large number of categories with only a few patients in each category.
Results
A total of 147 hips undergoing I&D for hip septic arthritis via anterior or medial approach were evaluated. Of the 147, 13 (8.8%) developed AVN (Table 1). Nine of 91 (9.9%) cases underwent an anterior approach developed AVN. Four of 56 (6.3%) cases underwent a medial approach developed AVN (p = 0.54). The average duration of symptoms in cases that developed AVN was 5.7 days, compared to 3.5 days in cases without AVN (p = 0.27).
Associations between demographic and clinical characteristics and AVN among septic hip patients.
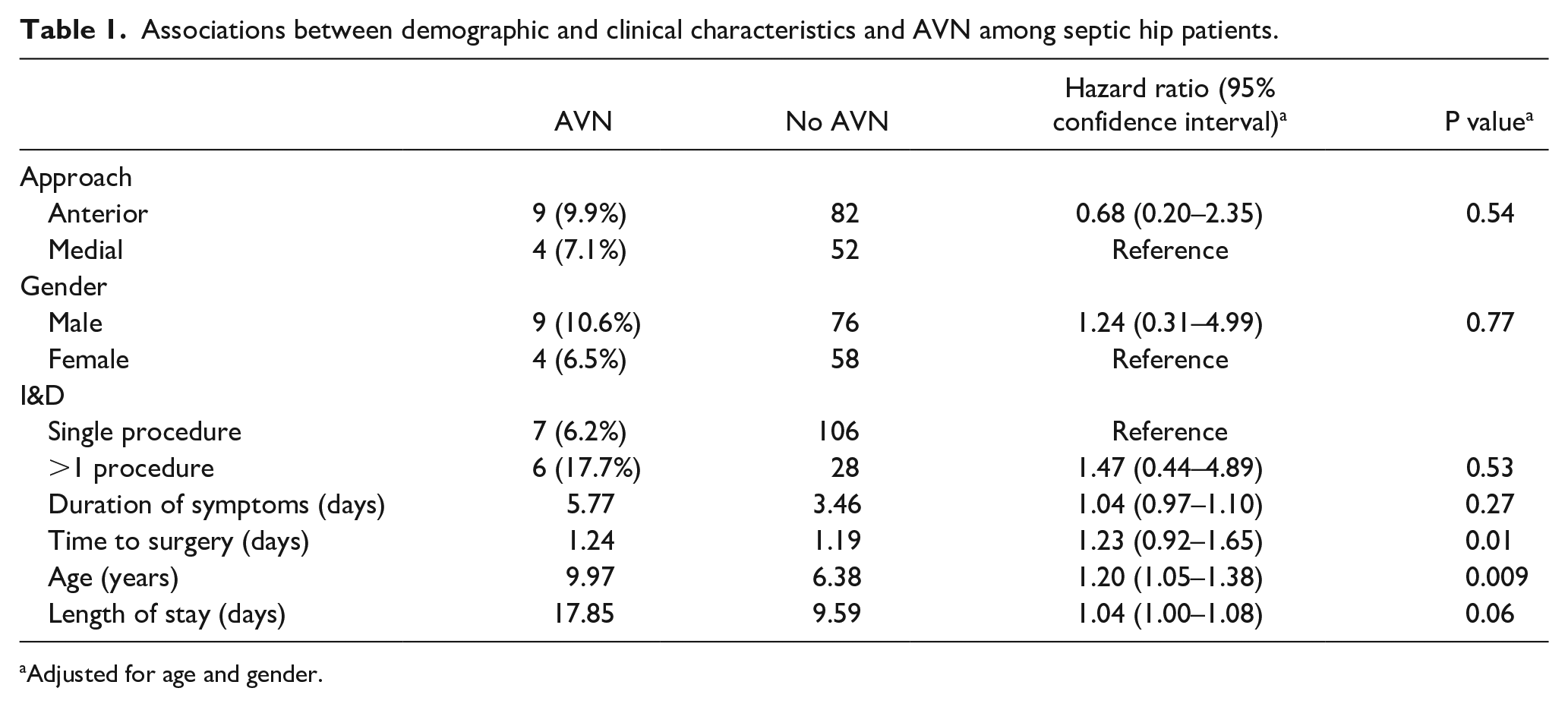
Adjusted for age and gender.
The average age for patients developing AVN was 10.0 years old versus 6.4 years old in patients who did not develop AVN (p = 0.009). The average time to surgery was 1.24 days in cases with AVN compared to 1.19 days in cases without AVN (p = 0.01). Average length of stay for patients who developed AVN was 17.9 days compared to 9.6 days in those who did not develop AVN (p = 0.06). The average follow-up was 40.1 months in patients with AVN versus 18.0 months for patients who did not develop AVN (p < 0.01). All hips that developed AVN had follow-up over 3 months, compared to only 80 of the 134 hip without AVN (p < 0.001).
Of those with AVN, six presented to the emergency department, five were transfers from outside hospitals, and two presented to the clinic (p = 0.17). Six of the 13 patients with AVN required repeat I&D versus 28 of the 134 hips in the group that did not develop AVN (p = 0.53).
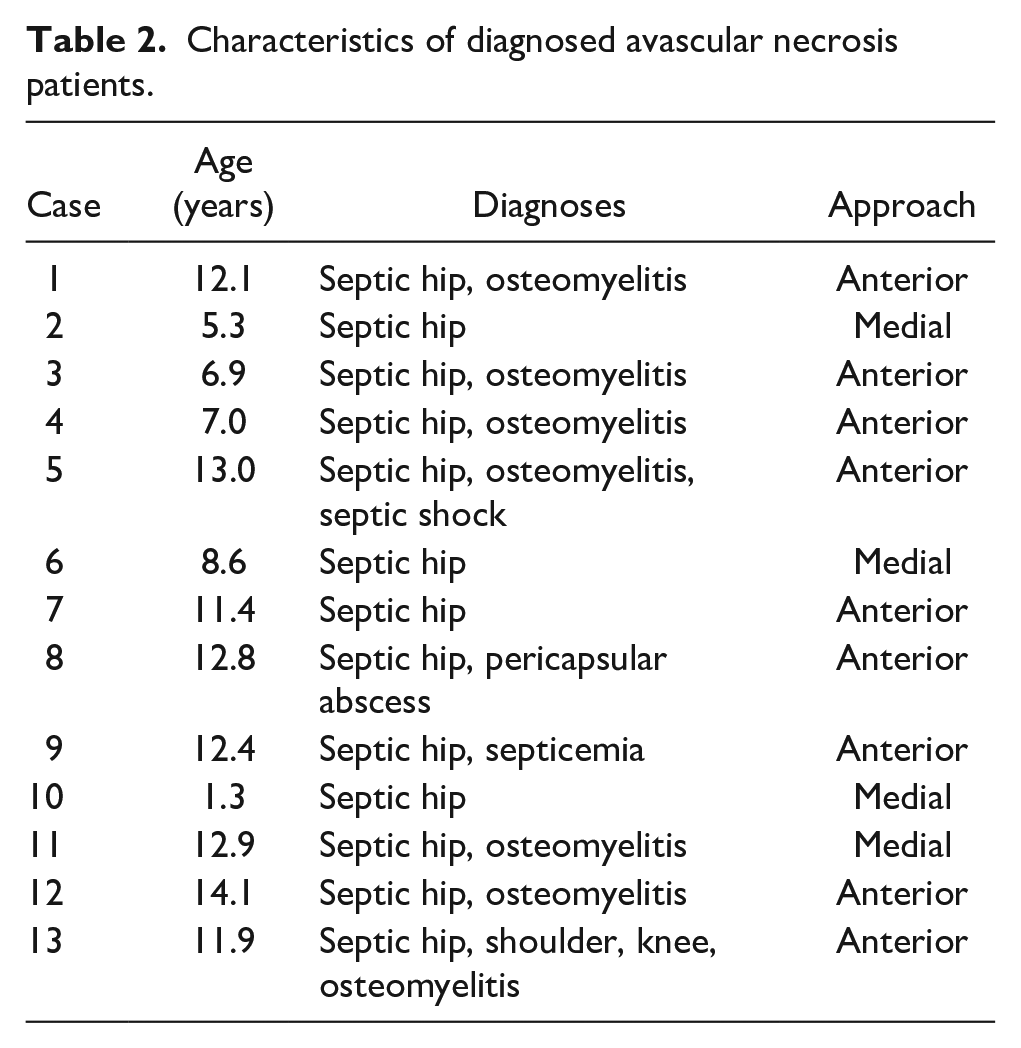
Nine of the 13 cases with AVN had diagnoses in addition to septic hip (i.e. osteomyelitis, other septic joint, sepsis, etc.) compared to 47 of the 134 without AVN (p = 0.03) (Table 2) (Figure 1).
Characteristics of diagnosed avascular necrosis patients.
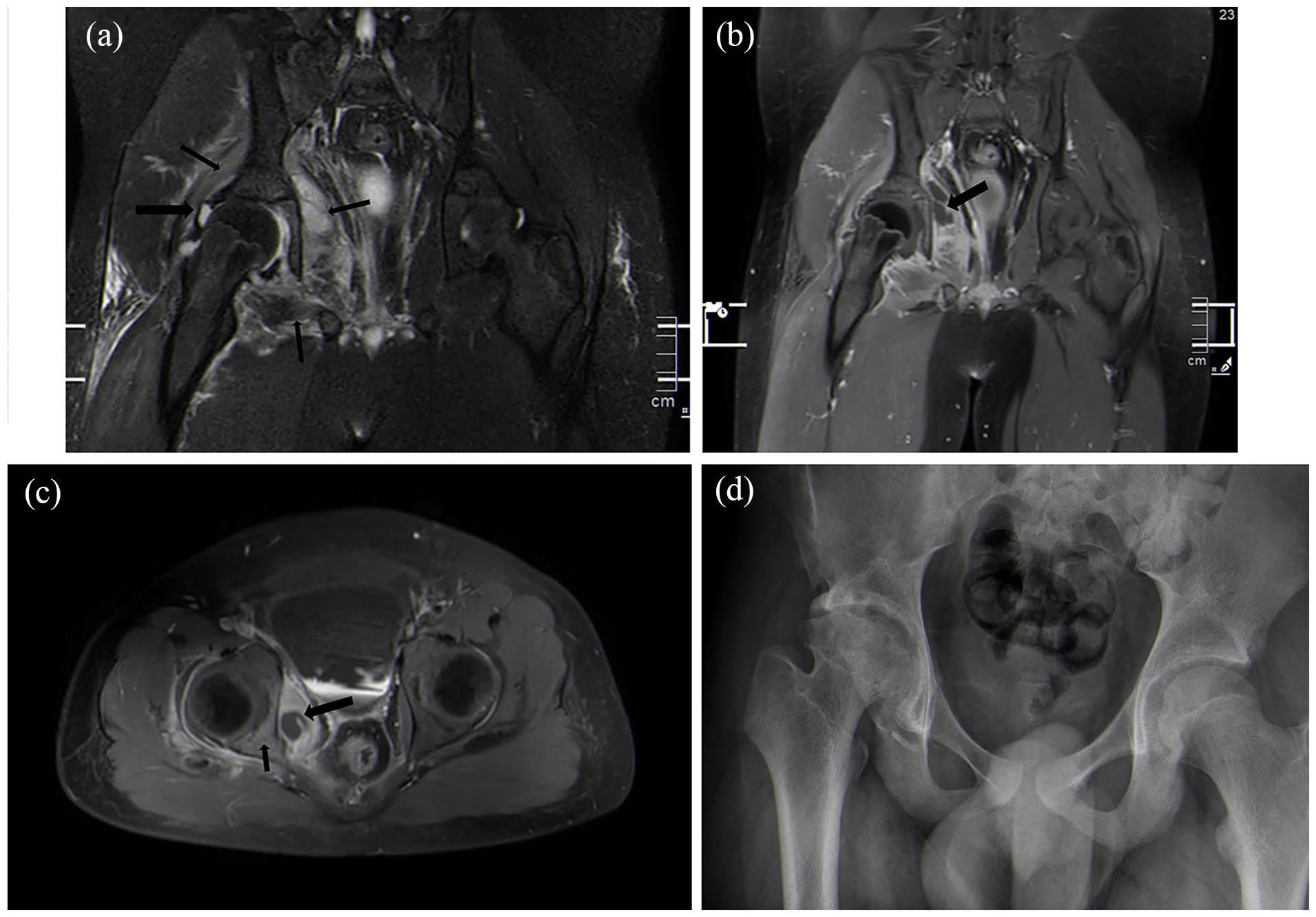
(a) Coronal T2 images of the pelvis in 11-year-old male with significant delay in presentation for fevers and right hip pain. Note right hip effusion (large arrow) and myositis (small arrows). (b) Post-contrast T1 coronal image discloses myositis with intrapelvic abscess (arrow). (c) Post-contrast T1 axial image discloses intrapelvic abscess (large arrow) and osteomyelitis of posterior column of acetabulum (small arrow). (d) Anteroposterior pelvis radiograph 2 years after initial presentation discloses evidence of AVN with femoral head irregularity and evidence of chondrolysis with joint space narrowing.
The following culture data were obtained from wound and/or blood culture: no growth (56.5%), MRSA (23.2%), MSSA (9.6%), Streptococcus pyogenes (2.1%), Streptococcus pneumoniae (2.1%), Group B Streptococcus (1.4%), coagulase-negative Staphylococcus (0.7%), Pseudomonas (0.7%), Gram-negative rods (0.7%), Gram-positive rods (0.7%), Haemophilus species (0.7%), rare Gram-negative rod (0.7%), and Candida parapsilosis (0.7%).
Discussion
Septic arthritis of the hip is a potentially devastating and life-altering disease affecting pediatric patients. Accurate diagnosis, prompt irrigation, and debridement are crucial to preserving the hip joint. Destruction of the hip may begin as early as 8 hours after inoculation. 18 Whether by direct release of bacterial toxins or enzymes, cytokines inducing matrix metalloproteinases, or increased capsular pressure leading to ischemia of the femoral head, the hip joint is under attack from the moment it becomes infected. 19 To our knowledge, this is the first study to compare the anterior and medial approaches for rates of AVN in pediatric septic hip.
There is abundant evidence evaluating anterior versus medial surgical approach in pediatric hips, but most of the literature is in regards to open reduction of DDH. Rates of AVN following medial approach for DDH range from <10% to 67%, though most report between 10% and 45%.5,9,10 The anterior approach is reported to have between 0% and 36% rate of AVN.5,9,10 Hoellwarth et al. 7 compared anterior and medial approach for open reduction of DDH and found no difference between the two groups in terms of development of AVN. Ucar et al. 5 found that 20% of patients with DDH who underwent an open reduction of the hip using a medial approach developed AVN.
To date, this is the first study comparing anterior and medial approaches for pediatric septic hip. We found no statistical difference between the two groups regarding the incidence of AVN. Advantages of the medial approach include a cosmetically pleasing scar and avoidance of risk to the lateral femoral cutaneous nerve.
It is interesting to note that length of hospital stay was a significant factor in the development of AVN, suggesting increased severity of initial illness in those who subsequently developed AVN (17.8 vs 10.5 days, p = 0.007). Furthermore, those who developed AVN also were more likely to have multiple diagnoses present at the time of I&D (p = 0.03). These findings are in agreement with Periasamy et al., 20 who found a significant association between episodes of sepsis and the development of AVN. All of this would seem to indicate that patients may suffer AVN from causes other than intracapsular pressure. Those with more severe disease may suffer perturbations in the normal inflammatory cascade that can give rise to thrombosis. 21 Thrombosis of the epiphyseal blood supply may combine with capsular pressure to increase the risk of AVN.
In this study, it was noted that the average age of patients with AVN was 10.0 years compared to 6.8 years in patients without AVN (p = 0.009). This is in keeping with Periasamy, who noted an increased prevalence of AVN with increasing age. 20
This study is limited by its retrospective nature and small patient cohort. It was not randomized and there were no pre-determined selection criteria to determine which patients underwent anterior or medial approach. This introduces potential bias as surgeons were allowed to choose the approach with which they were most comfortable. Furthermore, performance bias may be present if patients undergoing anterior and medial approaches were treated differently. There were a small number of patients who had insufficient radiographic follow-up to rule out AVN. However, given that our institution is the only freestanding children’s hospital in the state, and given the lack of orthopedists in the community who would likely manage pediatric hip conditions, it is unlikely that patients with symptoms of AVN would present elsewhere.
Pediatric septic hip is a potentially devastating disease that may have long-term sequelae, AVN being one of the most debilitating. This study indicates that the risk of AVN is not significantly different between the medial and anterior approaches. Our results indicate that increased hospital length of stay is associated with the development of AVN. This may be a proxy for severity of illness. Both medial and anterior approaches to pediatric septic hips are safe as long as respect is given to the anatomy and care is taken to preserve the blood supply to the developing femoral head.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241262167 – Supplemental material for Is choice of approach associated with risk of avascular necrosis in pediatric septic hip?
Supplemental material, sj-pdf-1-cho-10.1177_18632521241262167 for Is choice of approach associated with risk of avascular necrosis in pediatric septic hip? by Shrey Nihalani, Francis Cruz, Jacob K Hawkins, Branum Gage Griswold, Scott E Mabry, Gerald McGwin, Shawn R Gilbert and Michael J Conklin in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Gerald McGwin for his assistance in statistical review.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB
Ethical approval for this study was obtained from University of Alabama at Birmingham IRB (IRB-300006500).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.