
Abstract
Purpose:
We aimed to investigate whether globally decreased enhancement on post-reduction gadolinium-enhanced magnetic resonance imaging can predict avascular necrosis after open or closed reduction for developmental dysplasia of the hip.
Methods:
We retrospectively analyzed 83 patients (94 hips) who underwent open or closed reduction, with a minimum 5-year follow-up. There were 79 females (84%) with a median age of 7.2 months (interquartile range, 4.8–12). Femoral head enhancement on post-reduction gadolinium-enhanced magnetic resonance imaging was evaluated, and the most recent radiographs were graded using the Kalamchi and MacEwen avascular necrosis classification. Logistic regression was employed to identify predictors of avascular necrosis, and diagnostic performance was calculated.
Results:
Of the 94 hips, 51 (54%) exhibited normal enhancement, 20 (21%) had asymmetric enhancement, 11 (12%) had focal decreased enhancement, and 12 (13%) showed global decreased enhancement. At the final follow-up, 63 hips (67%) had no avascular necrosis, and 31 (33%) developed avascular necrosis: 13 (14%) Grade 2, 7 (7%) Grade 3, and 11 (12%) Grade 4 severe avascular necrosis. Multivariate analysis revealed no significant association between globally decreased enhancement, age, type of reduction, or abduction angle with the development of any avascular necrosis or severe avascular necrosis. Sensitivity was low for hips with any avascular necrosis (13%) and severe avascular necrosis (36%), while specificity was 87% and 90%, respectively.
Conclusions:
Globally decreased enhancement on post-reduction gadolinium-enhanced magnetic resonance imaging does not necessarily indicate long-term avascular necrosis development following closed or open reduction for developmental dysplasia of the hip. Treatment decisions should not solely rely on this finding. Further research is needed to improve imaging accuracy and assess whether modifying treatment in response to enhancement patterns can reduce avascular necrosis risk.
Level of Evidence:
Diagnostic, level 3 retrospective cohort.
Introduction
Avascular necrosis (AVN) of the femoral head is a significant complication that can arise following closed or open reduction treatment for developmental dysplasia of the hip (DDH) and lead to severe long-term sequelae, including proximal femoral growth disturbance, persistent acetabular dysplasia, and hip osteoarthritis.1,2 Thus, early diagnosis of patients at risk for AVN is crucial for ensuring appropriate management and family counseling.
Post-reduction gadolinium-enhanced magnetic resonance imaging (PRGE-MRI) allows qualitative assessment of femoral head enhancement following closed reduction for DDH; however, its ability to predict the development of AVN remains controversial.3 –8 The existing literature focuses on closed reduction, and the only study that incorporated open reduction included nine patients, limiting the generalizability of the results. 8 Moreover, longer follow-up studies are needed, as radiographic deformity may take several years to detect.2,9,10 While concerns have been raised about the safety of gadolinium due to its potential for accumulation and neurotoxicity in the developing brain,11 –13 there is limited evidence linking gadolinium deposition to long-term adverse effects or neurotoxicity in children with normal renal function.14,15
The study had two primary research questions: (1) Does globally decreased enhancement on PRGE-MRI associate with the development of AVN after open or closed reduction? (2) What is the diagnostic accuracy of globally decreased enhancement on PRGE-MRI in detecting or ruling out AVN in the long term, including sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV)?
Methods
Study population and surgical treatment
A retrospective study was performed on patients who underwent closed or open reduction for DDH at a tertiary pediatric hospital between 2000 and 2018. We initially identified a cohort of 510 patients with a hip dislocation (Figure 1). Of these, 124 patients with non-idiopathic DDH, 109 treated at external institutions, 15 with traumatic dislocations, and 54 who did not meet the minimum postoperative follow-up requirement of 5 years were excluded. In addition, 77 patients who did not undergo a PRGE-MRI after the application of the spica cast were excluded from the study. After these exclusions, 131 patients with a potential minimum follow-up of 5 years were eligible. Following these exclusions, 131 patients remained eligible based on the potential for a minimum of 5 years of follow-up. However, 44 patients (34%) were lost to follow-up and did not complete the 5-year assessment, resulting in a final study cohort of 83 patients (66%) with a minimum follow-up of 5 years (mean follow-up: 10 ± 3 years), including a total of 94 hips. Of these, 79 patients (84%) were female, and the median age at the time of reduction was 7.2 months (interquartile range (IQR), 4.8–12.0 months). Among the 94 hips, 49 (52%) underwent closed reduction and 45 (48%) underwent open reduction via the anterior (26/45 hips) or medial (19/45 hips) approach. No demographic difference existed between patients treated with closed versus open reduction, and subsequent surgery was performed in 24 hips (26%; Table 1).
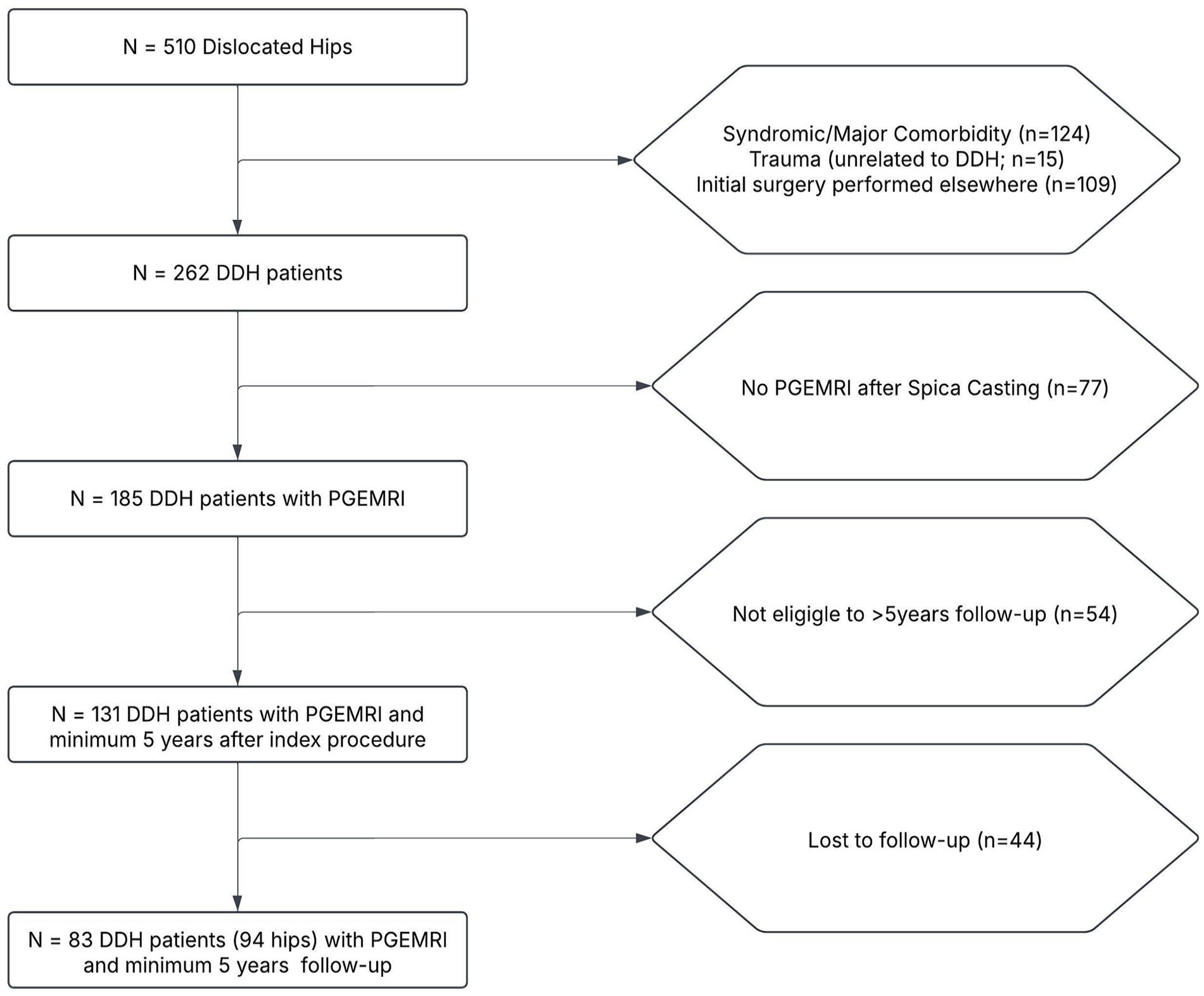
Study cohort selection for inclusion based on PRGE-MRI and minimum 5-year follow-up after closed or open reduction for the treatment of DDH.
Demographic characteristics of the overall study cohort and patients undergoing open/closed reduction.
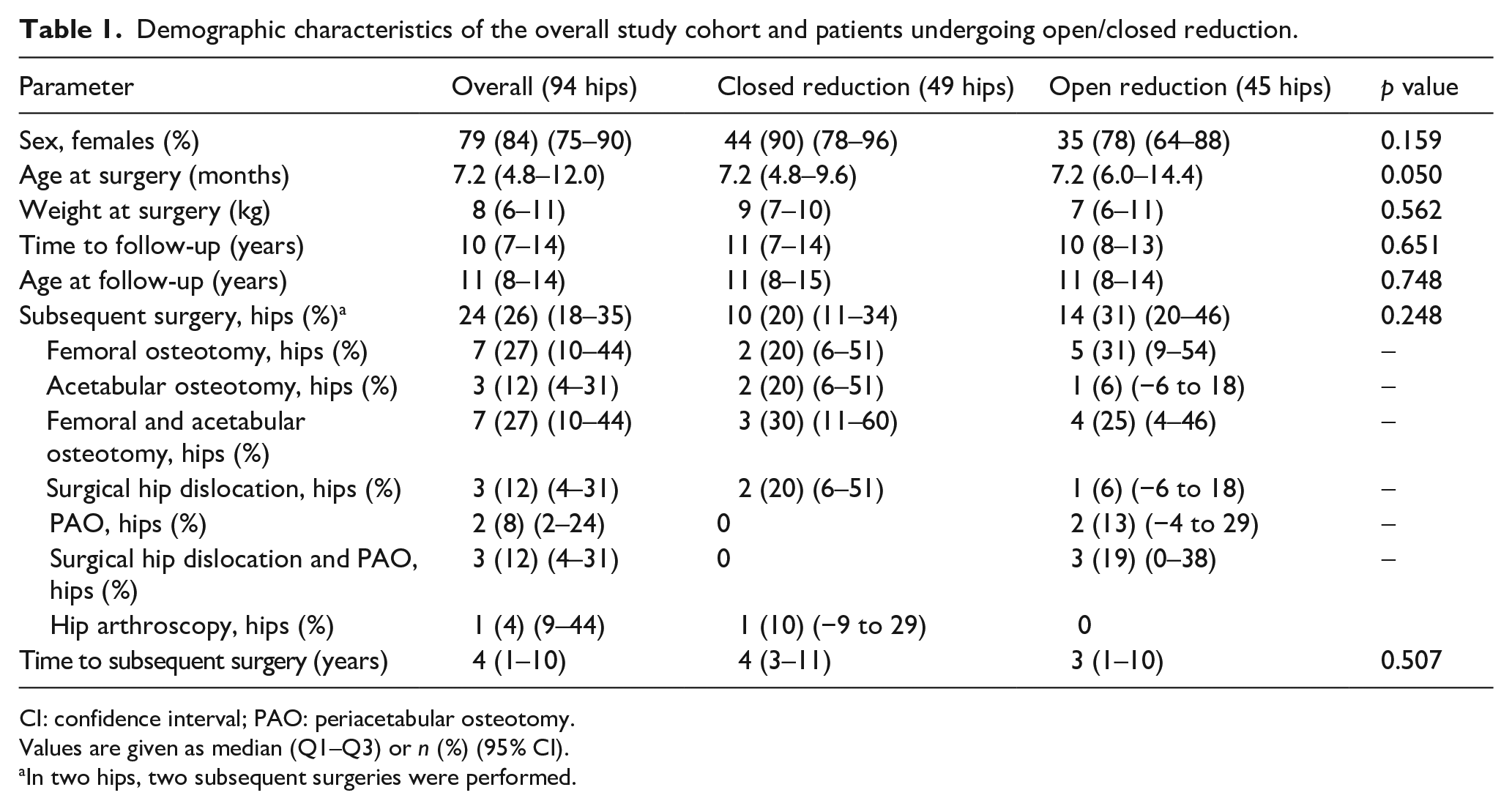
CI: confidence interval; PAO: periacetabular osteotomy.
Values are given as median (Q1–Q3) or n (%) (95% CI).
In two hips, two subsequent surgeries were performed.
During the study, PRGE-MRI results were shared with the surgeon, but treatment decisions were based on the quality of reduction due to uncertainty about the significance of decreased enhancement. Patients had follow-up appointments after 4–6 weeks for cast change. The cast was removed ~3 months post-surgery, and abduction bracing was worn at night for 6–12 months.
PRGE-MRI protocol
PRGE-MRI was performed on two different 1.5 T scanners (Siemens Medical Solutions, Erlangen, Germany, and General Electric, Milwaukee, WI, USA) within 24 h following reduction, following a previously established protocol. 4 The median time between closed or open reduction completion and postoperative MRI acquisition was 4 h (IQR, 2–6 h). The majority of hips—70 hips (74%)—underwent MRI within 6 h post-reduction. An additional 12 hips (13%) were scanned between 6 and 12 h, one hip (1%) between 12 and 18 h, and 11 hips (12%) between 18 and 24 h. We used a posterior surface coil and injected 0.2 mmol Gd-DTPA2- (Magnevist, Berlex, NJ, USA) intravenously. Patients were positioned supine in the spica cast, and imaging was performed without sedation in most patients. The minimum requirement of the imaging protocol was maintained throughout the study period. This included acquiring at least one pre- and post-contrast axial and coronal T1-/PD-weighted spin-echo sequence with fat suppression, each with an acquisition time of 1 min. The repetition and echo times for the T1-/PD-weighted sequence were 800–1000 and 11, 2200–2600 and 25 ms, respectively. The slice thickness was 4 mm, which ensured that at least four to five consecutive slices of the femoral head epiphysis were obtained field of view was 22–24 cm with a minimum matrix of 256 × 256, yielding an in-plane resolution of a least 0.9 × 0.9 mm. We obtained at least two enhanced images of the epiphysis to ensure the position of the femoral head relative to the acetabulum was visible.
Image analysis
PRGE-MRI analysis
We assessed the femoral head enhancement according to the enhancement grading pattern described by Tiderius et al., 4 previously reported to have high inter-observer agreement. The PRGE-MRI grading was determined through a consensus reading by two pediatric orthopedic surgeons (ENN and Y-JK) and a pediatric radiologist (SDB), each with over 10 years of experience in their respective fields. These readings were blinded with respect to patient history and the latest radiographic follow-up. Hips were categorized into four groups based on the severity of enhancement abnormality on PRGE-MRI: Grade 0 indicated normal enhancement; Grade 1, asymmetrical enhancement; Grade 2, focal decreased enhancement; and Grade 3, globally decreased enhancement. Globally decreased enhancement was defined as the absence of enhancement throughout the entire epiphysis, including the ossification center, when present (Figure 2). We limited the analysis to hips with globally decreased enhancement (Grade 3) because it is the only type of enhancement currently associated with the development of AVN.3 –8
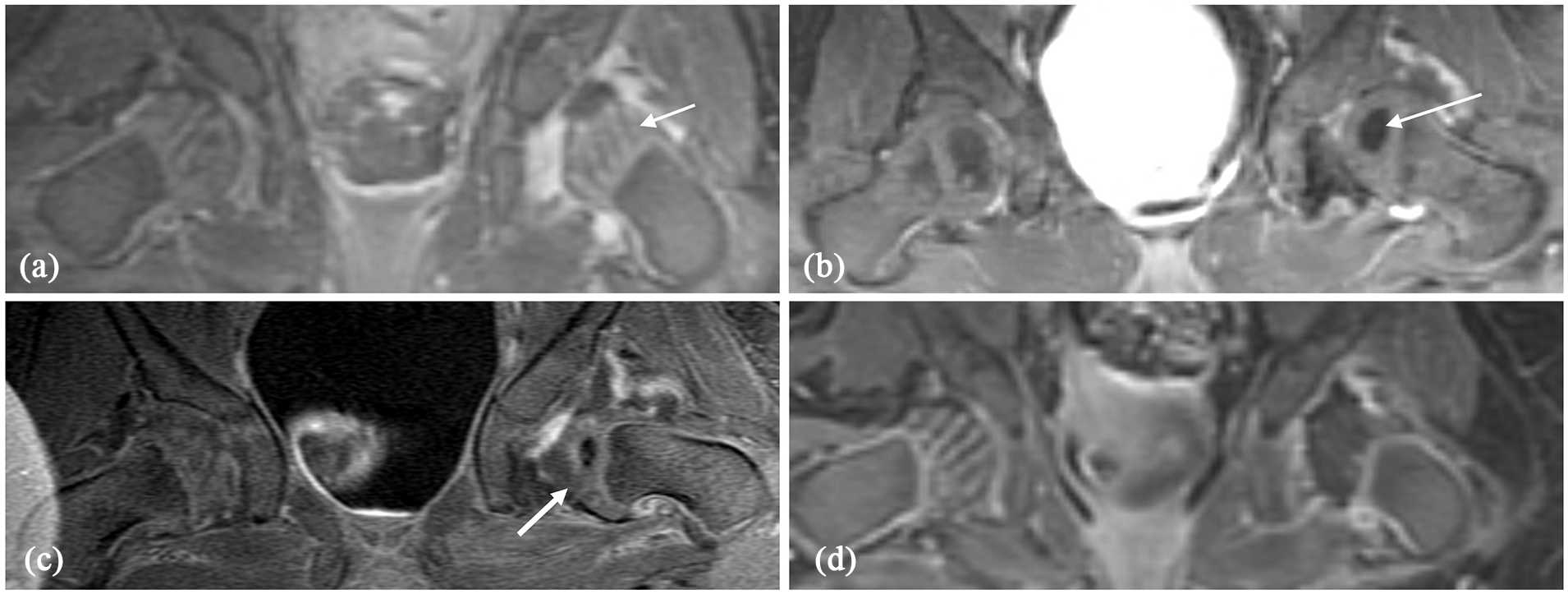
Classification of the enhancement pattern of the femoral head on PRGE-MRI for different patients treated with closed reduction of the left hip. (a) Grade 0: normal enhancement of the left hip after closed reduction, defined by visualization of the epiphyseal vascular canals and physis (white arrow). (b) Grade 1: asymmetric enhancement of the femoral head. The epiphyseal vascular canals were seen with less intensity than the contralateral hip, or the overall signal intensity of the ossific nucleus was lower than the contralateral right hip (white arrow). (c) Grade 2: focal decreased enhancement of the femoral head with an area of diminished signal intensity in the epiphysis or the center of ossification (white arrow). (d) Grade 3: globally decreased enhancement of the femoral head. The entire femoral head, including the center of ossification, when present, fails to enhance, and the femoral head appears dark without the vascular channels that are present on the contralateral right hip.
Radiographic analysis at final follow-up
We used the Kalamchi and McEwen 10 classification to assess AVN on the latest radiographs. Type 1 indicated minimal deformity, while types 2, 3, and 4 showed valgus deformity, coxa breva, and severe femoral head and neck deformity, respectively (Figure 3). Interobserver agreement was assessed using intraclass correlation coefficients by three blinded readers (ENN, Y-JK, and SDB), and discrepant cases were reviewed by consensus. Patients with AVN Grades 2–4 were placed in the “any AVN” group, while Grade 4 patients were classified as the “severe AVN” group, given their worse outcomes.1,2

The Kalamchi and McEwen classification was utilized to evaluate AVN in the most recent follow-up radiographs of individual patients included in this series. It should be noted that the study assessed all types of AVN (Grades 2–4), as well as severe AVN categorized explicitly as Grade 4. (a) Grade 1: minimum loss of residual height or coxa magna and no changes in the femoral neck with adequate acetabular development. (b) Grade 2: damage to the lateral part of the physis leads to decreased growth in the lateral segment of the femoral neck, leading to premature closure laterally, creating a tethering effect and causing a lateral tilt of the head into valgus (coxa valga). The femoral neck appears shorter and angled in valgus, with the acetabulum showing marked uncovering of the femoral head. (c) Grade 3: damage to the central aspect of the physis results in symmetrical growth retardation or cessation in the femoral neck, leading to a shortened neck (coxa brevis) with relative overgrowth of the greater trochanter. The head typically appears spherical, contained in the acetabulum. (d) Grade 4 (severe AVN deformity): damage to the head and neck leads to flattening of the femoral head and irregularity, widening, and shortening of the femoral neck with true varus angulation. The acetabulum is affected by persistent acetabular dysplasia.
Statistical analysis
Owing to their non-normal distribution, continuous variables were summarized using the medians and IQRs, and non-parametric tests were employed. 16 Categorical variables were presented using counts, percentages, and confidence intervals (CIs). Logistic regression was employed to examine the association between closed/open reduction, age, abduction angle, and globally decreased enhancement on PRGE-MRI as predictors for AVN. Inter-rater reliability calculated using Shrout–Fleiss’17,18 interclass correlation (2.1) was outstanding (0.792 (95% CI: 0.529–0.939) for the Kalamchi and McEwen 12 classification measured by K between the three observers. p Value below 0.05 was considered statistically significant, and all tests were two-sided. We used the SAS software (Version 9.4; SAS, Cary, NC, USA). Sensitivity, specificity, PPV, and NPV of globally decreased enhancement on PRGE-MRI were computed to differentiate between hips with any form of AVN and severe AVN from hips without AVN.
Results
Following the Tiderius et al. 4 grading scheme, 51 out of the 94 hips (54%) exhibited normal enhancement, 20 (21%) showed asymmetric enhancement, 11 (12%) displayed focal decreased enhancement, and 12 (13%) had globally decreased enhancement. At final follow-up, the median age was 11 years (IQR, 8–14 years). Of the 94 hips, 63 (67%) had no AVN, and 31 (33%) developed AVN at a median of 10 years (IQR, 7–14). Based on the Kalamchi and MacEwen 10 criteria, 13 hips (13/94;14%) exhibited Grade 2 AVN, 7 (7/94;7%) Grade 3, and 11 hips (11/94;12%) showed severe (Grade 4) AVN (Table 2).
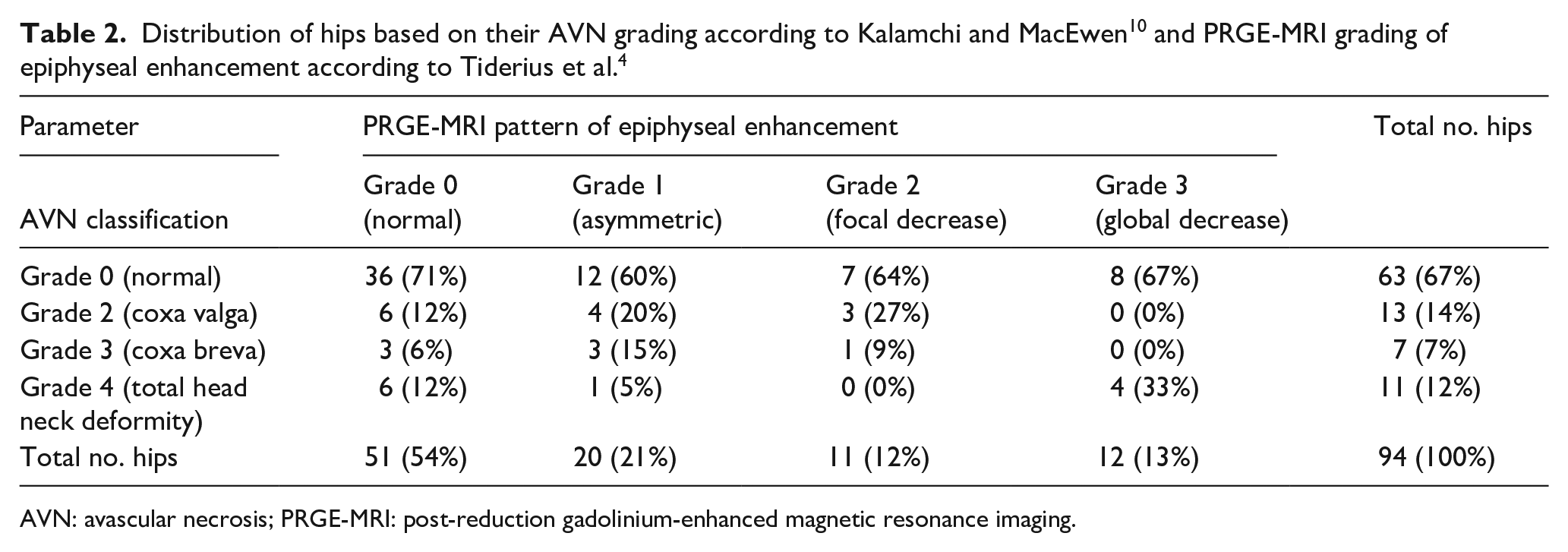
AVN: avascular necrosis; PRGE-MRI: post-reduction gadolinium-enhanced magnetic resonance imaging.
There were no significant differences between hips that developed any AVN or severe AVN and those without AVN regarding age, weight, type of surgery, and abduction (Table 3). Multivariate regression analysis showed that none of the parameters, including age at surgery, type of surgery (open versus closed reduction), abduction angle, and globally decreased enhancement on PRGE-MRI had a statistically significant association with the development of any AVN (Grades 2–4) or severe AVN (Grade 4; Table 4).
Demographic characteristics of patients without AVN (Grade 0), any type of AVN (Grades 2–4), and severe AVN (Grade 4).
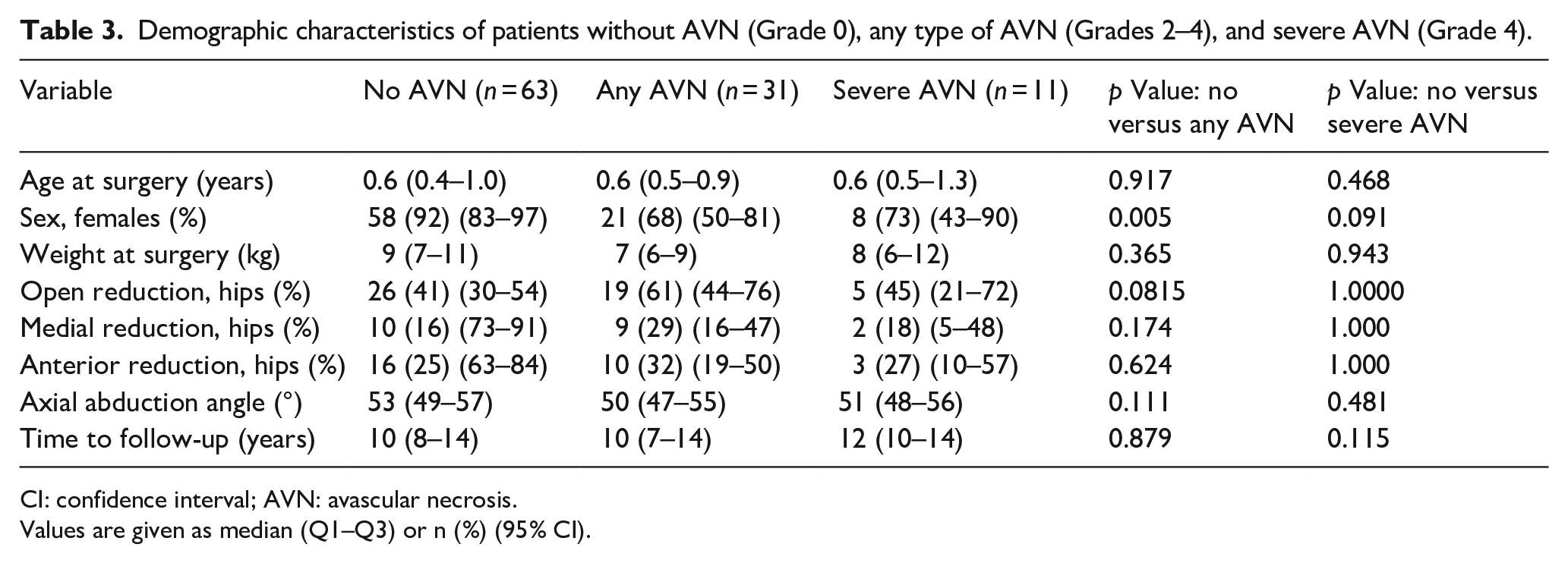
CI: confidence interval; AVN: avascular necrosis.
Values are given as median (Q1–Q3) or n (%) (95% CI).
Multivariate analysis.
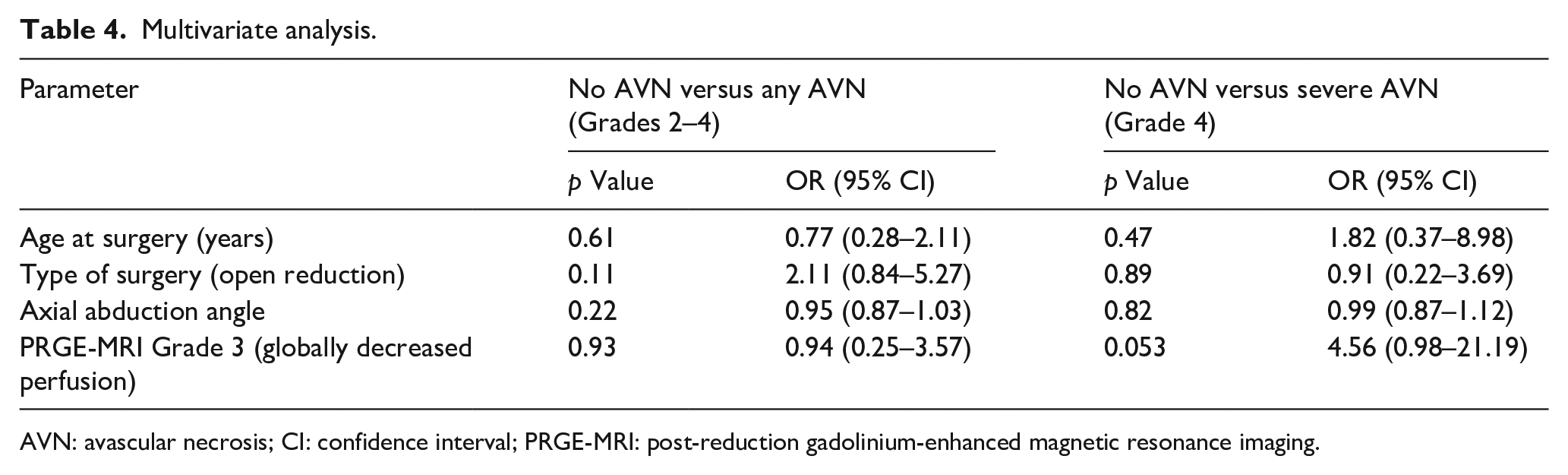
AVN: avascular necrosis; CI: confidence interval; PRGE-MRI: post-reduction gadolinium-enhanced magnetic resonance imaging.
The accuracy analysis to evaluate the performance of globally decreased enhancement on PRGE-MRI in discriminating hips without AVN from those with any form of AVN (Grades 2–4) or severe (Grade 4) AVN indicated that the PRGE-MRI could identify severe AVN with slightly better accuracy than any AVN (84% versus 63%). However, the results suggest limitations in the test’s ability to identify both AVN groups accurately. The sensitivity was poor among the hips with any AVN (13%) and severe AVN (36%). The specificity was 87% and 90%, respectively. In addition, the PPV was poor (33% for both), while the NPV was moderate for any AVN (67%) and high for severe AVN (91%; Table 5).
Diagnostic performance of globally decreased enhancement on MRI to distinguish any radiographic AVN (Grades 2–4) and severe radiographic AVN (Grade 4).
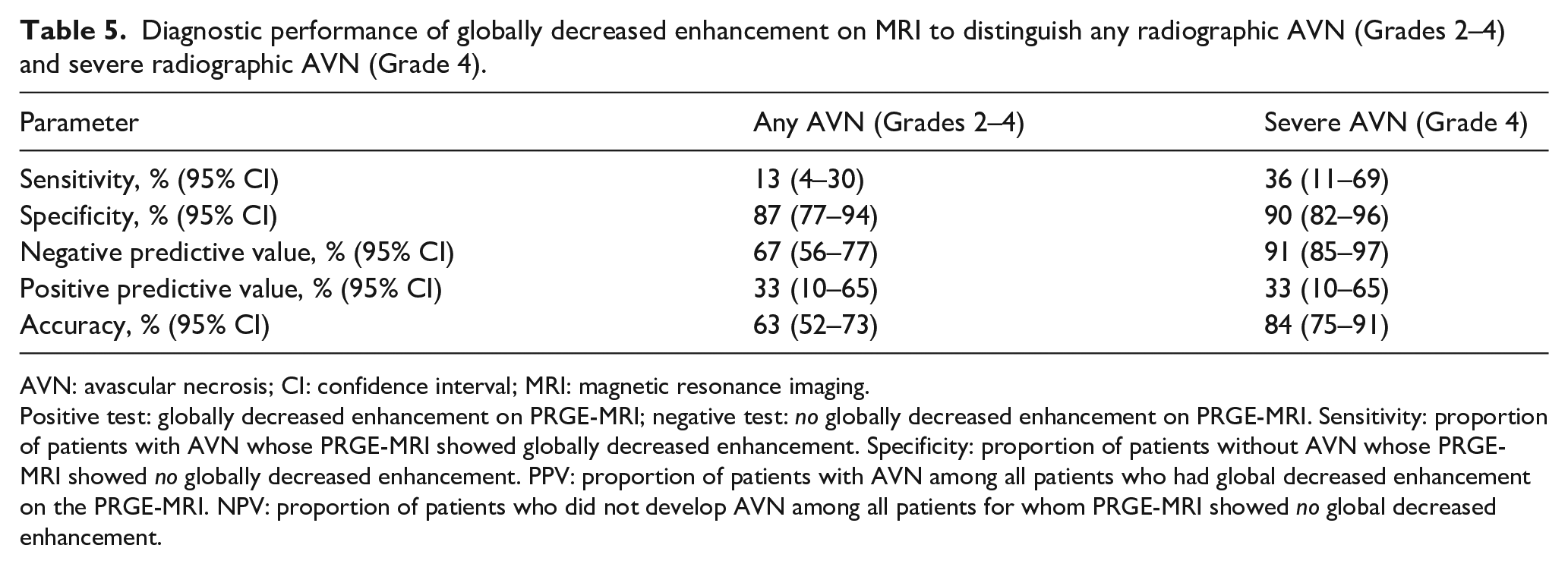
AVN: avascular necrosis; CI: confidence interval; MRI: magnetic resonance imaging.
Positive test: globally decreased enhancement on PRGE-MRI; negative test: no globally decreased enhancement on PRGE-MRI. Sensitivity: proportion of patients with AVN whose PRGE-MRI showed globally decreased enhancement. Specificity: proportion of patients without AVN whose PRGE-MRI showed no globally decreased enhancement. PPV: proportion of patients with AVN among all patients who had global decreased enhancement on the PRGE-MRI. NPV: proportion of patients who did not develop AVN among all patients for whom PRGE-MRI showed no global decreased enhancement.
Discussion
This study investigated the diagnostic accuracy of globally decreased enhancement on PRGE-MRI in diagnosing any form of AVN or severe AVN by assessing hip deformity at least 5 years after closed or open reduction. Globally decreased enhancement on PRGE-MRI was not associated with AVN development. The sensitivity of PRGE-MRI was poor, with a low proportion of hips that developed any AVN or severe AVN correctly identified by globally decreased enhancement. (Figure 4) Specificity was better with a high proportion of hips free of any or severe AVN, correctly identified by the absence of globally decreased enhancement. The NPV for severe AVN was high, indicating that the preserved enhancement on PRGE-MRI could accurately identify most hips that did not develop AVN, which aligns with previous studies suggesting no AVN development in hips with normal enhancement.6–9 However, the PPV was poor, indicating that only one-third of hips with globally decreased enhancement actually developed any AVN and severe AVN in the long term. Therefore, it is not absolutely reliable to use the presence of globally decreased enhancement on PRGE-MRI to predict the development of AVN-related deformities in the long term after closed or open reduction (Figure 5).
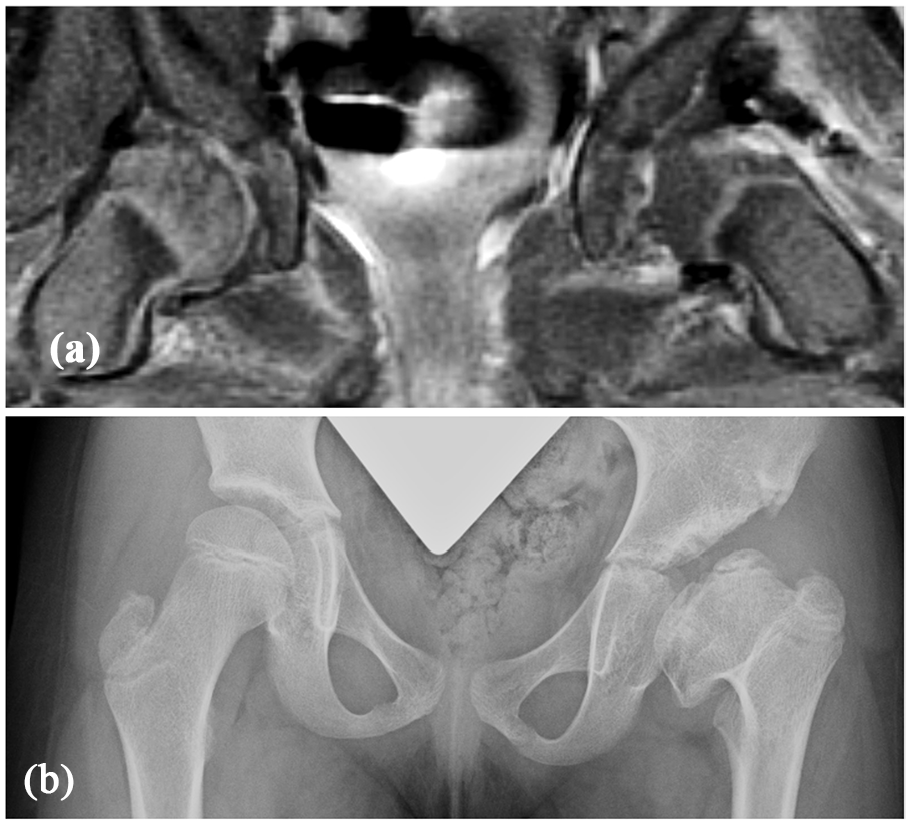
True-positive result for globally decreased enhancement leading to AVN in a 6-month-old female undergoing open reduction. (a) Coronal T1-weighted turbo spin echo PRGE-MRI performed within 6 h after open reduction of the left hip shows global decreased enhancement of the epiphysis without the vascular channels, which can be observed on the contralateral right femoral head. (b) Anteroposterior pelvic radiograph of the patient obtained 7 years after reduction, at age 7.5, shows a severe (Grade 4) AVN deformity according to the Kalamchi and McEwen classification.

False-negative result for globally decreased enhancement leading to AVN in a 5-month-old female. (a) Coronal T1-weighted turbo spin echo PRGE-MRI acquired within 6 h after closed reduction of the right hip shows no enhancement of the epiphysis with globally decreased enhancement and absence of the enhanced vascular channels, which are present on the contralateral left femoral head. (b) Anteroposterior pelvic radiograph of the patient obtained 10 years after reduction, at age 11, shows a spherical femoral head concentrically reduced into the acetabulum without any major associated deformity of the femoral neck and greater trochanter.
Our study contradicts previous studies that suggested an association between decreased enhancement and AVN development after closed reduction in smaller case series with shorter follow-up.4 –7 Tiderius et al. 4 were among the first to propose that PRGE-MRI may predict AVN after closed reduction. Haruno et al. 5 found decreased enhancement in patients with AVN after an average of 3 years following closed reduction. Cheon et al. 7 identified excessive abduction and globally decreased enhancement as factors for AVN in infants who were evaluated around 1 year after closed reduction. Including patients with a minimum of 5-year follow-up may have yielded different results from previous studies that assessed AVN based on radiographs obtained over a shorter term. Short-term assessment may lead to an underestimation of the prevalence of AVN since it can take several years for the proximal femoral deformity to develop. 10 Notably, Grade 2 AVN, the most common pattern of growth disturbance, has a latent onset typically observed between the ages of 5 and 12 years, with potential progression until skeletal maturity.1,2,9,10,20–23 Nevertheless, our findings align with Nguyen et al., 8 who found no significant difference in enhancement between AVN and non-AVN groups in 38 children treated with closed and nine with open reduction and followed for an average of 47 months.
The clinical implications of our findings do not align with previous studies, suggesting a change in management may be warranted for patients with globally decreased enhancement on PRGE-MRI following hip reduction for DDH.3 –5 First, globally decreased enhancement was not a predictor of AVN. Second, the PPV and sensitivity were poor. Therefore, changing the management of all hips with globally decreased enhancement would lead to unnecessary overtreatment. Moreover, no previous study showed change in management can impact the rate of AVN. In one study, 5 two patients had casts changed within 24 h because their PRGE-MRI showed decreased enhancement. However, after the cast was changed, both patients had similar enhancement levels. Another study 3 reported on 22 patients treated with closed reduction and PRGE-MRI and compared them to a historic cohort without PRGE-MRI. At the final follow-up, a higher proportion of AVN was observed in the historic cohort (28% compared to 4%). The authors proposed that using a PRGE-MRI after closed reduction could lower AVN risk by allowing surgeons to assess femoral head vascularity and adjust treatment before AVN changes become irreversible. However, the two hips with decreased enhancement on PRGE-MRI, leading to an open reduction, were excluded from the follow-up AVN analysis. To determine whether management changes can reduce the development of AVN in patients with globally decreased enhancement, future long-term, randomized studies prospectively evaluating clinical management are needed.
In this study, revascularization of the epiphysis with globally decreased enhancement may have accounted for the absence of long-term AVN. Haruno et al. 5 identified two patients in whom a repeat PRGE-MRI was performed within 28 h after the initial scan that showed decreased enhancement. In both patients, the repeat scan showed improved enhancement, and neither of these patients developed AVN. Nguyen et al. 8 obtained three post-contrast series and showed that the enhancement pattern could change over time, as evidenced by a case where a hip that initially showed near-absent enhancement on early images demonstrated improvement on the late images. Notably, the time course of ischemia and the extent of epiphyseal damage remain unclear. One experimental study 19 demonstrated that femoral head ischemia could be reversed if corrected within 6 h. Another study 20 showed that a prolonged lack of blood flow (96 h) is needed to increase water mobility and contrast enhancement, a finding which is possibly related to the irreversible process of cartilage matrix breakdown. Although further investigation using sequential PRGE-MRI could establish whether revascularization is a viable phenomenon and determine the specific time frame in which it occurs and whether AVN is irreversible after that, conducting such studies may be challenging due to concerns about gadolinium accumulation in the pediatric brain.
This study has limitations. First, similar to previous studies,3,4 we only investigated hips with globally decreased enhancement on the PRGE-MRI. The consequences of asymmetrical and focal reduction of enhancement remain unclear and require further investigation to be fully understood. Furthermore, globally decreased enhancement, defined according to the original description 4 as global decreased enhancement of the entire epiphysis, does not quantify the disruption of blood flow. This limitation of PRGE-MRI may be overcome by the advancement of the technique. Notably, advancements in MRI technology, such as the widespread use of 3T technology and dynamic contrast-enhanced MRI of bone marrow enhancement, may allow for further quantitative assessment of blood flow to the epiphysis, but these were unavailable during this study. Second, the study is limited by its retrospective design, which hindered the ability to standardize the protocol for image acquisition and timing of MRI after reduction over the extended study period. Although we examined the MRI performed within 24 h after the reduction, following reduction similar to the original study describing this technique, 4 there was minor variability of the time between casting and image acquisition. Notably, most patients (74%) underwent MRI within 6 h of reduction, and 87% of patients were imaged within 12 h, minimizing the likelihood that temporal differences affected the interpretation. However, variability in MRI acquisition timing remains a relevant consideration, and efforts to standardize early imaging may improve reproducibility in future studies. Third, the MRI protocol did not account for the dynamic, time-dependent nature of gadolinium transit through the immature femoral head. Repeated scans could capture both early and late enhancement phases and improve the sensitivity of detecting enhancement changes; however, it is not currently performed in our clinical practice. Fourth, we experienced a loss to follow-up of 35% of patients at the minimum 5-year follow-up threshold. However, the minimum 5-year follow-up criteria were implemented to mitigate the possibility of under-diagnosing the onset of AVN, an important limitation of previous studies. Moreover, our institution serves as a tertiary pediatric center, and we receive a considerable number of patients referred from various regions nationally and even globally, which poses challenges to ensuring patient compliance with radiographic follow-up.
In conclusion, our findings highlight the critical limitations of globally decreased enhancement on PRGE-MRI as a predictive tool for AVN following a closed or open reduction in DDH. Our findings suggest that there is a low likelihood of long-term AVN development if there is no globally decreased enhancement on PRGE-MRI. However, the clinical significance of globally decreased enhancement after reduction remains uncertain, as it did not reliably predict the occurrence or severity of AVN, raising concerns about its diagnostic accuracy. Consequently, we do not recommend modifying the treatment strategy solely based on findings of globally decreased enhancement. Future research should prioritize improving the diagnostic accuracy of PRGE-MRI. In addition, longitudinal, prospective studies are needed to evaluate whether adjustments in management for patients with globally decreased enhancement can effectively reduce the incidence of AVN.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: One of the authors (FS) received funding from the Swiss National Science Foundation (grant no. 181643) during the conduct of this study.
Ethical considerations
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research. This work was performed at Boston Children’s Hospital, Boston, MA, USA.