
Abstract
Background
Balanced forces around the hip joint are critical for normal development of the hip joint, so it should be considered in every hip reconstructive procedure.
Methods
In seven children with complete destruction of the femoral head and neck due to septic arthritis, a reconstructive hip surgery was done to reconstruct the femoral head without sacrificing the greater trochanter and its muscles completely. The technique consists of a modified greater trochanter arthroplasty with only a medial portion of the greater trochanter and a varus femoral osteotomy.
Results
The average age of the children at surgery was 17 months (range 8–36 months) and the patients were followed for an average of 16.6 years (range 10.9–20.1 years). The average number of second operative procedures for each patient was 2 (range 1–4). The follow-up evaluation for each patient included documentation of pain, hip range of motion, and assessment of gait. In addition, the current leg-length discrepancy, final coverage and stability of the hip joint were documented. At final evaluation, all patients had a pain-free stable hip and two patients had near-normal hip range of motion. All patients have had satisfactory surgery results.
Conclusions
By this kind of hip reconstruction, we could provide a stable painless hip joint with special attention to the greater trochanter's role on hip biomechanics.
Introduction
Infantile hip sepsis occurs infrequently; however, without early diagnosis and treatment, it can cause serious musculoskeletal sequelae [1–3]. The potential complications seen following infantile septic arthritis of the hip are diverse, including: premature closure of the triradiate cartilage and/or proximal femoral physis, limb length inequality, subluxation, dislocation, and complete destruction of the femoral head and neck with resultant marked functional impairment [4].
Treatments to recommend for sequelae of infantile septic arthritis of the hip depend on the presenting complications and deformities. They can range from nonoperative treatments [5, 6] to extensive femoral and pelvic surgeries [7–10], both with the goal of having a stable, mobile, and painless joint as a desirable result.
To better define and understand the resultant deformities and surgical planning strategies, there are some classification systems to assist in this, such as Hunka et al. [4], Choi et al. [7], and, recently, that of Forlin and Milani [11]. The base of these classifications are on dislocation of the hip joint and the presence of head and neck remnants. A more severe form of the disease (Hunka type V or Choi type IVB) is very rare, therefore, its recommended treatment has a limited use.
The purpose of this study was to review our new method of “greater trochanteric preserving hip arthroplasty” for the treatment of hips with Choi type IVB residual deformities.
Materials and methods
Patients selected for the “greater trochanteric preserving hip arthroplasty” method met the following criterion:
Younger than 3 months of age when the septic arthritis developed Had complete destruction of the femoral head and neck by the septic process (Choi IVB hips or Hunka type V) Had been followed for more than 10 years
All patients were offered this type of treatment; however, all other available options, such as surgical or nonsurgical treatments, had been explained to the parents and they were informed about the overall poor prognosis of the problem. Other parents who did not accept this reconstructive surgery were referred to other centers.
Nine patients met the criteria for the arthroplasty. Only seven patients came back for the final follow-up evaluation. There were four boys and three girls, with an average age of 17 months (range 8–36 months) at the time of the surgery (Fig. 1a). The right side was involved in three patients and the left side in four. Five patients had late drainage and two did not undergo hip drainage.

All patients in this series had been operated by one senior orthopedic surgeon at an average of 20 months (range 6–30 months) after the known original infection.
A “greater trochanteric preserving hip arthroplasty”, which was a combination of a Colonna trochanteric arthroplasty [12]—with preserving lateral portion of the greater trochanter—and a proximal femoral varus osteotomy [13], was performed in all patients.
Technique
The patient is placed in the supine position and the involved hip is elevated by placing a sandbag underneath the ipsilateral side of the pelvis. The entire extremity is draped free so that intraoperative manipulation of the hip is possible. Through an anterior iliofemoral approach, the interval between the sartorius and the tensor fasciae latae is developed. The straight head of the rectus femoris is tagged with a suture and released from its origin at the anterior inferior iliac spine. The anterior hip capsule is then excised, in order to remove all interposing tissues in the acetabulum.
The gluteus medius and minimums with an outer one-third of the greater trochanter were separated. Any remnant of the femoral neck is resected flush with the inner surface of the femoral shaft. The iliopsoas tendon is released from the lesser trochanter, and the vastus lateralis and intermedius are reflected distally, exposing the proximal end of the femur. The short external rotators muscles are sectioned at their insertions and the adductors are released, if they restrict hip abduction to less than 30°. A subtrochanteric osteotomy is then performed through a straight lateral incision and fixed with a plate, effectively placing the greater trochanter into the acetabulum. Then, the osteotomized lateral portion of the greater trochanter is fixed to the lateral proximal femoral shaft by a screw or pullout suture (Fig. 1b). The straight head of the rectus is reattached at its origin. The patient is then immobilized in a spica cast for 3 months.
In our series, documentation was made if any additional surgical procedures were done. The decision to perform the second procedure depended on the serial follow-up examinations and X-rays, not on a regular time frame; for example, an acetabular osteotomy was done based mainly on the age of the patient and uncoverage zone of the new head. To date, the average number of second operative procedures per patient was 2 (range 1–4): greater trochanter advancement osteotomy on five hips (Fig. 1c), greater trochanter epiphysiodesis in two patients, additional varus intertrochanteric osteotomy on one hip, Salter osteotomy on four hips, Chiari osteotomy in two, and Staheli shelf procedure in one patient. Implant removal was performed in five patients completely and in one patient partially (not considered as an additional surgery). Two patients had a femoral lengthening, in addition to one tibial lengthening for one of them. One of the patients had an epiphysiodesis of the contralateral distal femoral physis (Table 1). Total hip replacement as a final point of the longevity of the procedure was not performed on any patient.
Demographic information, surgical procedures, and the clinical results of the patients with severe sequelae of septic hips
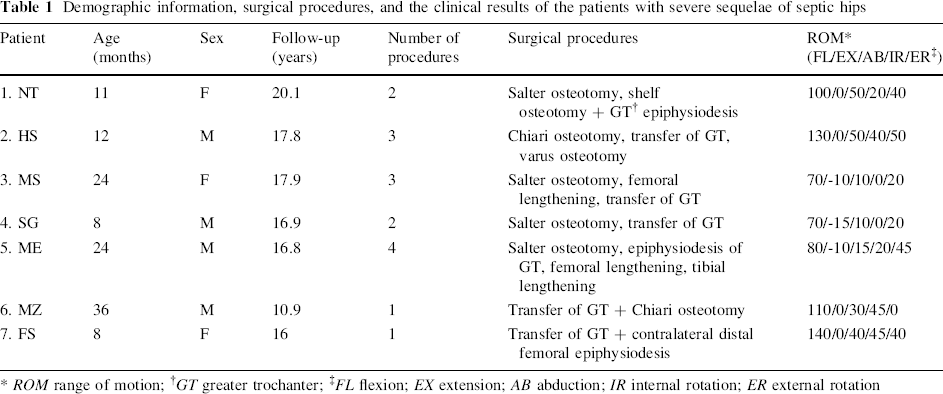
ROM range of motion;
GT greater trochanter;
FL flexion; EX extension; AB abduction; IR internal rotation; ER external rotation
The average length of follow-up was 16.6 years (range 10.9–20.1 years). The follow-up evaluation for each patient included: documentation of pain, hip range of motion, and assessment of gait, all performed by one senior surgeon. Nevertheless, current leg-length discrepancy (LLD), final coverage and stability of the hip joint were also documented.
Results
Noteworthy, at final evaluation, all patients had a pain-free hip. Hip stability and LLD were our major concern during the follow-up period. In all but one patient, acetabular osteotomies were done to achieve a stable hip. In two patients, Salter innominate osteotomy was performed at the index operation and the other osteotomies or shelf procedure were performed on stage surgery after the index operation (Table 1). Abductor lurches were not seen in our patient, but two patients limped, which was due to a significant LLD. All hips were located at the last follow-up (Fig. 1 d, e). Avascular necrosis was seen in one patient (Fig. 2).

Two patients had near-normal hip range of motion. There were three patients with mild flexion contracture (10°–15°) and flexion of the hip joint was greater than 90° in four patients. The others had flexion between 70° and 90°. Internal rotation and abduction of the hip were restricted to less than 20° in two patients. External rotation was severely limited in one patient (Table 1). Femoral lengthening was performed on two patients. One of them (MS, Table 1) had lengthening at age 8 years, but because of previous femoral head necrosis and gradual subluxation, we could not achieve more than 25 mm lengthening; her final LLD was about 50 mm (Fig. 2d). Another patient (ME, Table 1) had 45 mm femoral lengthening at age 9 years and then 35 mm tibial lengthening at age 11 years, with the final LLD about 10 mm. The actual mean LLD for all patients was recorded as 1.9 cm (range 1–5 cm).
All patients achieved a near-normal level of daily activities. The results could be simply classified as satisfactory or unsatisfactory, based on criteria proposed by Hunka et al. [4]. The results were considered to be satisfactory when three criteria were met: (1) the joint was stable; (2) the arc of flexion was 70° or more, with a flexion contracture no greater than 20°; and (3) the patient was free of pain and was able to perform activities of daily living. Based on Hunka et al.'s criteria [4], in our series, all hips were satisfactory. Two patients might need extra lengthening procedures at final evaluation.
Discussion
Biomechanically, a stable congruent hip will work well for many years. The importance of the greater trochanter as a lever to balance forces around the hip joint should not be ignored. These balanced forces make a spherical congruent hip during hip development until 4 years of age.
Various forms of reconstructive procedures have been described that attempt to salvage the hip joint with the goal of making a stable painless articulation [13]. Trochanteric arthroplasty is one such procedure that redirects and substitutes the cartilage of the trochanteric apophysis to overcome the problem of the absent femoral head into the acetabulum [14]. Variable results have been obtained with all forms of trochanteric osteotomy [12, 15]. When successful, it provides stability of the joint, less abductor lurch, less limb-length discrepancy, and better anatomic conditions for later prosthetic replacement [13]. The most favorable results have been reported when this procedure is combined with a proximal femoral varus osteotomy in cases with a variable severity of hip destruction [7, 13, 16]. In addition to varus osteotomy, the greater trochanter was divided in this study to preserve potential effects of the greater trochanter on the hip joint biomechanics for cases with the most severe type of hip destruction.
Freeland et al. [13] studied greater trochanteric hip arthroplasty among 17 children with catastrophic loss of femoral head. They showed that all of the children in their series were limping and they concluded that this limp may be due to abductor weakness, LLD, pain, or a stiff hip joint. The other aspect of their study was progressive subluxation of the greater trochanter, which, in one patient, eventually resulted in a late dislocation. They mentioned that the most important cause of such subluxation was the lack of an adequate abductor lever arm. Another problem related to a weak abductor was gradual straightening of the proximal end of the new femoral head. This may lead to progressive subluxation of the greater trochanter from the hip joint, which may necessitate a repeat varus osteotomy [13]. We tried to preserve the lateral portion of the greater trochanter with its muscular attachment to avoid such problems. Actually, the potential complication of this procedure is greater trochanter overgrowth, which forced us to transfer it in five patients and carry out epiphysiodesis in two patients, but we think that this complication would be worth it in order to obtain such good results.
The major concern with trochanteric arthroplasty of any kind is the potential risk of the avascularity of the proximal osteotomized portion. Dobbs et al. [14] reported one case of avascular necrosis of the greater trochanter among five patients who underwent trochanteric osteotomy plus proximal femoral varus osteotomy. They noted that total hip motion was surprisingly good, even in this patient with avascular necrosis of the trochanter. In our study, one case developed avascular necrosis of the trochanter, but the overall motion of the hip joint was satisfactory, in spite of developing avascular necrosis of the head fragment (Fig. 2d).
Overgrowth of the greater trochanter might be due to avascularity of the osteotomized medial portion which had been constructed as the femoral head. But the standard technique with trochanteric arthroplasty is a combination of the removal of all soft tissue from the greater trochanter and then varus osteotomy of that portion. Therefore, the risk of avascularity of the reconstructed femoral head should be much higher than our technique [14]. The advantage of our new technique is the preservation of soft tissue attachment to the lateral portion of the greater trochanter and, as previously mentioned, the biomechanical benefits of this preservation. In spite of the good results reported by Cheng and Lam after femoral lengthening on four patients with Choi IVB hip involvement [17], we have had one hip subluxation and loss of hip mobility after femoral lengthening (Fig. 2). They attributed their good results to the hip joint stabilization by acetabular or femoral head reconstructive procedures, but in our case, the reconstructive procedure and salter osteotomy were performed before lengthening to stabilize the hip joint. On the next case, we performed tibial lengthening to prevent this problem, which was successful.
The latest study was published by Dobbs et al. [14] in which five patients with Hunka type V hip were followed after a hip reconstructive procedure (trochanteric osteotomy plus proximal femoral varus osteotomy). At their final evaluation, four patients had pain-free hips and one had mild hip pain with prolonged ambulation; no patient had an antalgic gait. All hips were located at the latest follow-up and were stable; one hip had autofused. Surprisingly, on their radiographs, only two patients had Hunka type V and the others were type IV A or B. But based on Hunka et al.'s criteria [4], four hips were satisfactory and the result in one patient was unsatisfactory. When comparing these results with ours, with “greater trochanter preserving hip arthroplasty”, we were able to obtain satisfactory results in all Hunka type V patients.
We believe that the satisfactory results with a congruent hip after “greater trochanteric preserving hip arthroplasty” are because of the balanced muscle action on the proximal femur. Balanced muscular tension on the hip joint can produce a congruent hip joint. The support of our hypothesis of the muscular tension is overgrowth of the greater trochanter in nearly all patients, which, in turn, could be treated by a simple procedure, such as greater trochanter distal transfer or epiphysiodesis.
Conclusion
When considering the positive biomechanical effects of the greater trochanter on hip development and its stability, a stable, painless, and functional hip can be obtained in children with complete destruction of the hip joint with the “greater trochanter preserving hip arthroplasty” performed at an early age.