
Abstract
Purpose:
The aim of the study was to compare the different internal fixations between elastic stable intramedullary nailing and Kirschner wires in treatment of angulated radial neck fractures.
Methods:
We retrospectively reviewed the patients with radial neck fracture without associated injuries who underwent surgery approach in our department during April 2011–March 2020. There were 62 patients meeting all the criteria with complete clinical data, with median age of 7.5 (IQR 5.8–9.5) years, 34 males and 28 females. The preoperative fracture pattern was assessed according to the Judet classification system. Depending on the materials implanted and fixation strategy, the patients could be divided into a Kirschner wire group and an elastic stable intramedullary nailing group. Final functional outcomes of patients were assessed by the Mayo Elbow Performance Score and Tibone–Stoltz functional evaluation classification.
Results:
The Kirschner wire group included 37 patients, with 4.8 years median follow-up. The elastic stable intramedullary nailing group included 25 patients with 5.9 years median follow-up. There were no significant differences in gender, age, Judet classification, average operative time, Mayo Elbow Performance Score, Tibone–Stoltz classification, or length of hospital stay between groups. However, the time to union in the Kirschner wire group was significantly shorter than that in the elastic stable intramedullary nailing group (p < 0.05). Both groups achieved satisfactory functional and cosmetic results.
Conclusion:
In the management of pediatric radial neck fractures, both elastic stable intramedullary nailing and Kirschner wire internal fixation have shown equivalent therapeutic results, leading to satisfactory functional outcomes. The selection of the internal fixation approach can be influenced by the patient’s fracture characteristics and the surgeon’s preferences.
Level of evidence:
Level III; Retrospective Comparison; Treatment Study.
Introduction
Radial neck fractures in children are rare and constitute approximately 10% of elbow fractures. 1 The treatment approaches relied on the degree of angulation and displacement of the radial neck, and the age of the children. Conservative treatment is normally the initial choice for those with angulation of less than 30° and translation of less than 2 mm, while higher degree of displacement is considered an indication for surgical intervention. In clinical practice, different surgery strategies exist for reduction and fixation, such as elastic stable intramedullary nailing (ESIN) or Kirschner wires (K-W). However, the literature evidence is inconclusive as to which is the preferred option. In this study, we conducted a retrospective analysis of patients with radial neck fractures who were treated at our department. We aimed to compare the clinical outcomes of two different fixation strategies.
Patients and methods
We retrospectively analyzed the patients with radial neck fractures who had undergone surgical intervention at our department between April 2011 and March 2020. Patients with associated injuries, such as nerve damage or concomitant fractures, were excluded from the study. These cases were completed by three senior physicians in the pediatric orthopedic department, each with a minimum of 20 years of specialized experience. All patients were followed up regularly post-surgery. A total of 62 patients with complete clinical data were included in the study, with a median age of 7.5 (interquartile range (IQR): 5.8–9.5) years, 34 males and 28 females. The preoperative fracture pattern was assessed according to the Judet classification system, 2 and the patients were divided into a K-W treatment group and an ESIN treatment group depending on the implanted materials and fixation strategy. Specifically, the K-W treatment group had 37 patients, with 13 closed reduction and 24 open reduction, while the ESIN treatment group had 25 patients, with 21 closed reduction and 4 open reduction. The median follow-up time was 5 (2.2–8.8) years. The patients in K-W and ESIN groups underwent surgery during the same time periods. Final functional outcomes of patients were assessed by the Mayo Elbow Performance Score (MEPS), Tibone–Stoltz functional evaluation classification, 3 and measurements of pronation/supination.
Surgical technique
K-W treatment group
Once the patient was successfully anesthetized, they were placed in a supine position and the forearm was further pronated to move the posterior interosseous nerve (PIN) away from the surgical area. First, a percutaneous levering reduction was conducted to assess the reduction of the radial head fracture. If an anatomical reduction can be achieved, two 1.0-mm antegrade K-Ws can be placed to securely transfix the fracture. The forearm’s flexed and pronated position facilitates easier K-W fixation. This approach, coupled with fluoroscopic guidance, can significantly enhance the success rate of the fixation process, avoiding repetitive, rough levering reduction and minimizing iatrogenic injury. If the fracture cannot be anatomically reduced or the stability of K-W fixation is insufficient, then an open reduction is required.
A 3.5-cm skin incision was made on the posterolateral elbow. Under the protection of the PIN and superficial branch of the radial nerve, the caput radii and radial neck were exposed through the brachioradialis muscle and extensor carpi radialis longus muscle. The fracture was exposed after the removal of the periosteum and soft tissue, and the fracture was then cleaned to ensure an open reduction. The radial head was gently repositioned, and any interposed capsular or ligamentous structures blocking the reduction were removed. With the guidance of fluoroscopy, two antegrade K-Ws were placed percutaneously to transfix the fracture. The annular ligament was then sutured, the pin was bent and cut, and the pintail was retained in the outer skin (Figure 1).
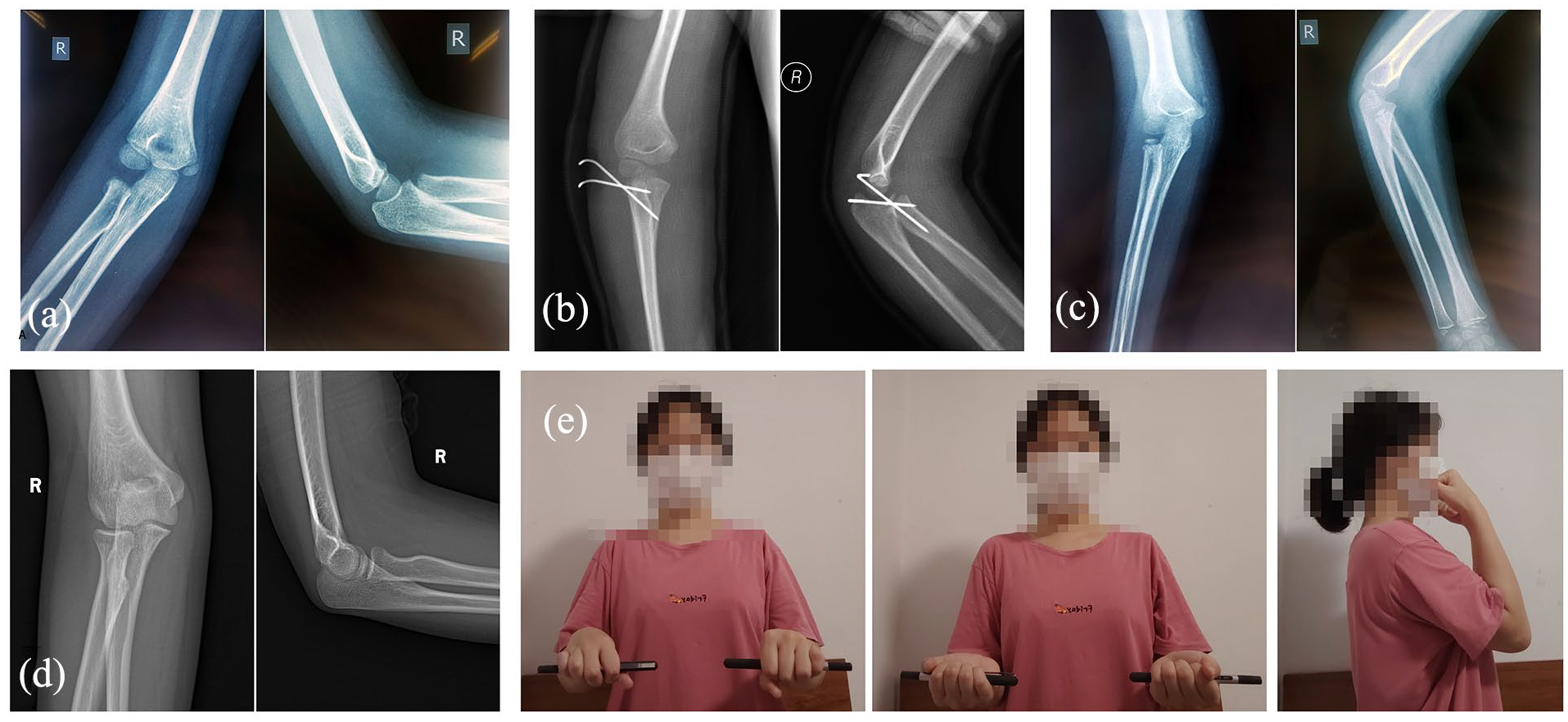
A 6-year-old girl, at the time of her injury, underwent open reduction and internal fixation with K-W for the fracture. Following a period of 9 years of careful monitoring, she experienced a successful recovery. (a) X-ray film during injury. (b) X-ray film after open reduction and internal fixation with K-W for the fracture. (c) X-ray film after removal of internal fixation, 5 weeks after surgery. (d and e) Follow-up of 9 years after the fracture, including the patient’s imaging data and activity status.
ESIN treatment group
ESIN fixation for radial neck fracture was first described by Metaizeau and colleagues,4,5 with the following surgical procedure. Once the patient was anesthetized, a 0.5–1 cm incision was taken from the dorsal side of distal radius, careful scissor dissection to the lateral radial cortex was performed with the protection of epiphysis, taking care not to damage the superficial radial nerve. An appropriately sized ESIN (1/3–1/2 width of internal diameter) was advanced through the radius to the fracture site. Extensor tendons, especially extensor pollicis longus, were encountered and should be carefully shielded during the opening of the radial cortex.
For patients who have not responded to closed reduction, a widely adopted approach involves a combination of percutaneous leverage reduction using K-Ws to align the fracture, followed by fixation with ESIN. 6 In this combined technique, the radial head is first reduced using K-Ws, then permitting successful passage of the distal tip of ESIN into the proximal fragment. Severe displacement of the radial head often poses a common challenge. The technique of percutaneous leverage reduction with two K-Ws, as described by Du et al., 7 has proven effective in increasing the rate of minimally invasive reduction. The ESIN should be impacted into the epiphysis for maximal fixation. With appropriate reduction of fracture, the nail should be rotated 90°–180° as needed to hook the proximal fragment. If the percutaneous leverage reduction fails, open reduction at the proximal of radius is needed, and the surgical procedure is similar with open reduction procedure in the K-W group (as described above). ESIN was passed across the fracture line to ensure the stability through the elastic hook structure at the front. At last, the ESIN should be cut distally, and avoid soft tissue irritation and extensor pollicis longus fraying from implant prominence (Figure 2).
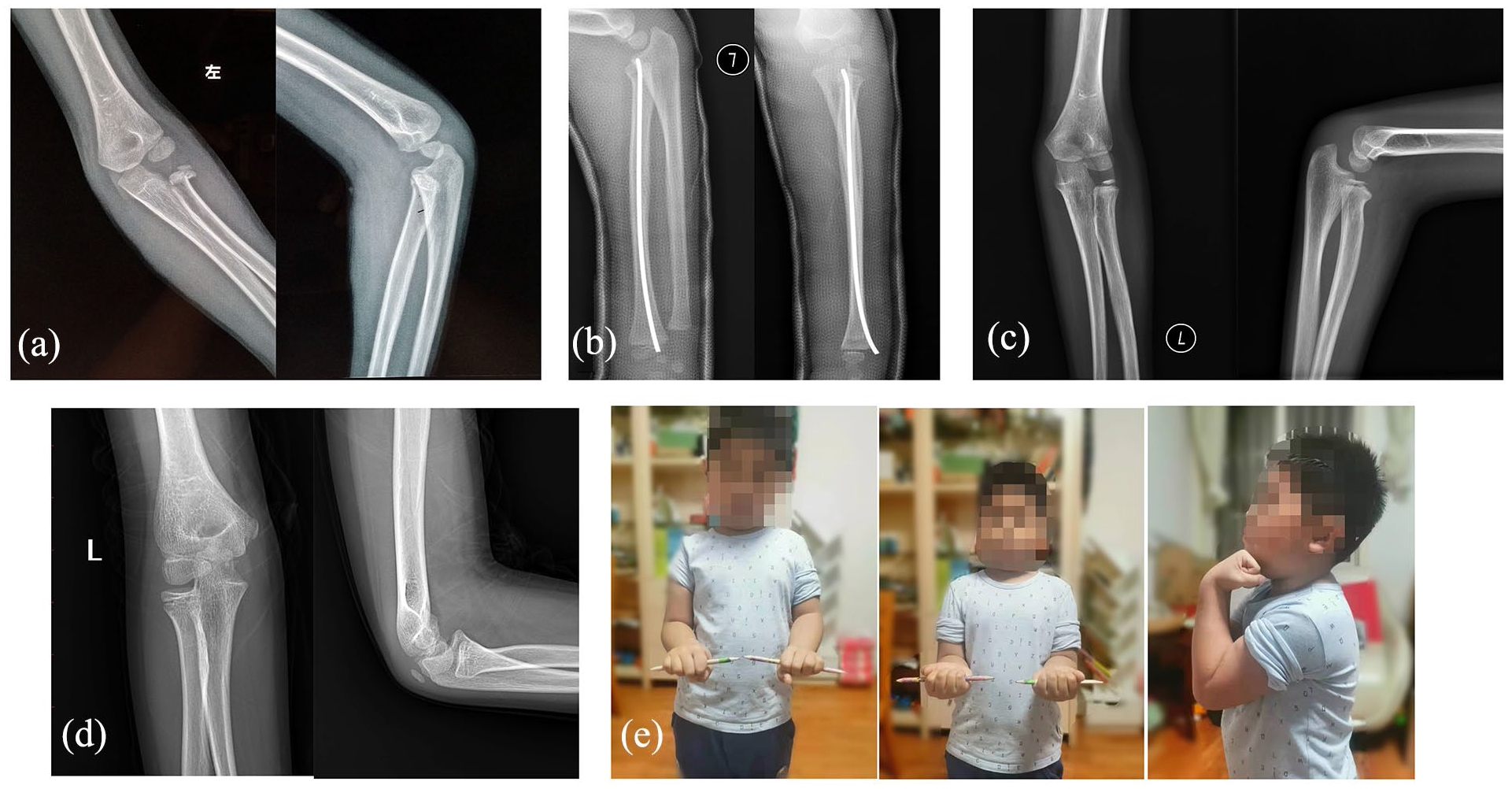
A 5-year-old boy, at the time of injury, underwent closed reduction and internal fixation with ESIN. After 4 years follow-up, he achieved a favorable outcome. (a) X-ray film after injury. (b) X-ray film after closed reduction and internal fixation with ESIN. (c) X-ray film after the removal of internal fixation, 9 months after surgery. (d and e) After 4 years of follow-up, the patient’s imaging data and functional activities were recorded.
Postoperative care and follow-up
Following surgery, all patients required immobilization with an above-elbow cast in a neutral position and flexion of 90° for 3–4 weeks. Radiographic examinations were conducted every week to assess the union of the radial neck fracture. Union time was estimated. The criteria for fracture union involve the nearly complete disappearance of the fracture line, accompanied by the presence of bridging fracture callus that can be discernible at three cortices on at least two orthogonal radiographs. 8 K-Ws were removed once the fracture had united, at 4–6 weeks postoperatively. ESINs were removed under general anesthesia at 4–6 months postoperatively. Rehabilitation exercise was instructed to perform with guidance to prevent elbow stiffness. Clinical evaluations were conducted at each follow-up, including range of elbow movement, elbow carrying angle, and vascular and neurologic examinations. All the complications were identified and recorded after surgery. Postoperative elbow function was assessed using the MEPS score and Tibone–Stoltz classification during follow-up.
Statistical analysis
Statistical analysis was conducted using SPSS 25.0. Pearson’s chi-square test or Fisher’s exact test were used to measure the differences when appropriate. A p-value of less than 0.05 was considered statistically significant. Post hoc power analysis was performed with G*Power (3.1.9.7, Dusseldorf, Germany).
Results
In the K-W treatment group, there were 37 patients with 18 males and 19 females, with a median age of 7.5 (IQR 5.7–9.6) years. In addition, 13 patients underwent percutaneous levering with closed reduction, and the other 24 patients were with open reduction (Table 1). The median follow-up was 4.8 (2.2–8.8) years and the average hospital stay was 4.30 days. The average operative time was 1.27 h. The distribution of fracture severity via Judet class was as follows: 12 IIs (<30°), 16 IIIs (30°–60°), 6 IVa (60°–80°), and 3 IVb (>80°). In the K-W group, there was one patient with superficial infection caused by the tail of the K-W and recovered quickly after taking out the K-W. In addition, no avascular necrosis or other complications were found (Table 2). The time of union ranged from 4 to 6 weeks, with an average of 5 weeks, and one patient with open reduction had union at 7 weeks. The average MEPS score was 98.2, with a range of 85–100. According to the Tibone–Stoltz classification, three patients were rated as good and the others as excellent. Most patients had a successful recovery, with the exception of one child who had mild supination restriction
Patients’ characters in K-W treatment group.
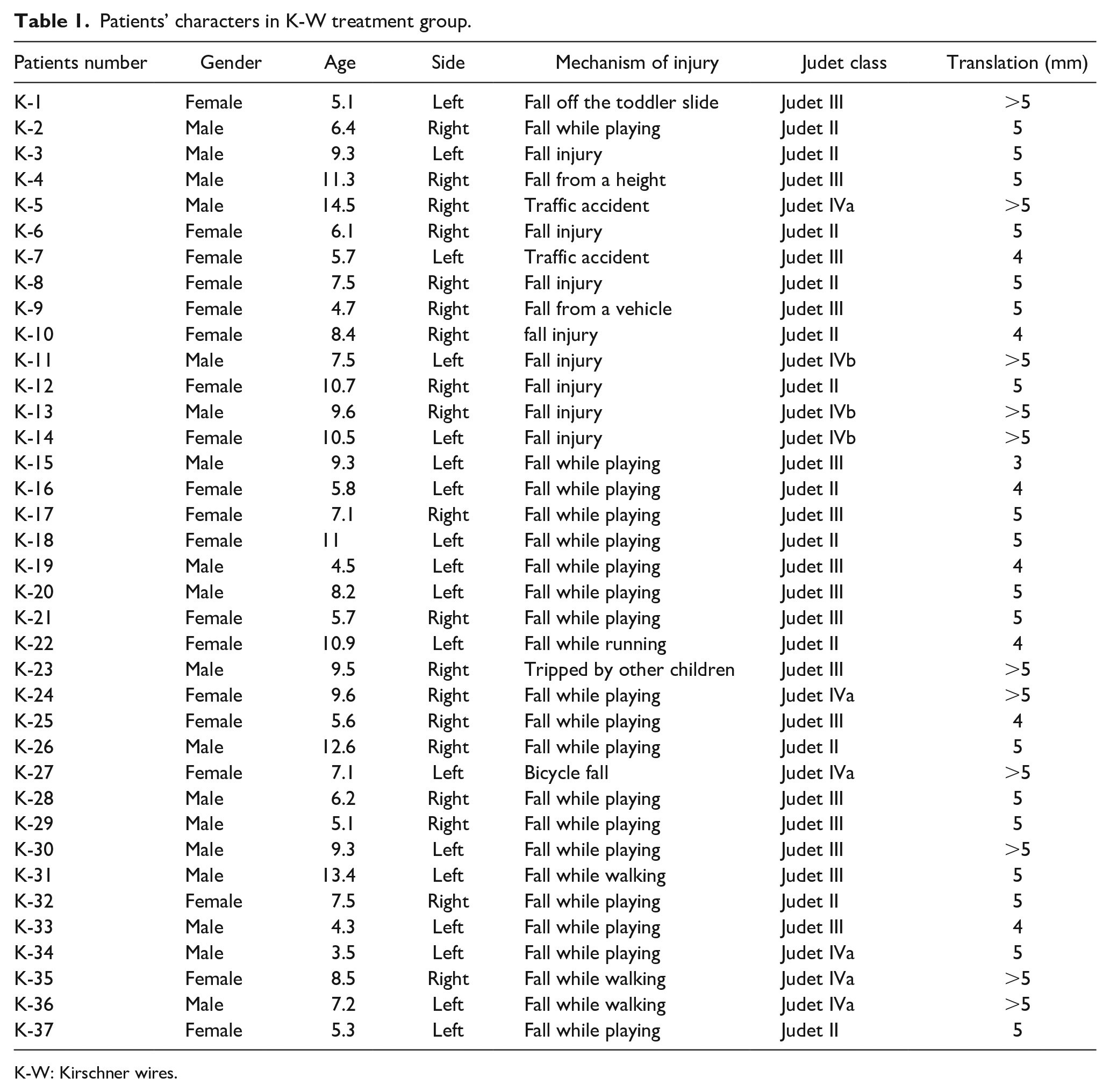
K-W: Kirschner wires.
Treatment and outcome in K-W group.
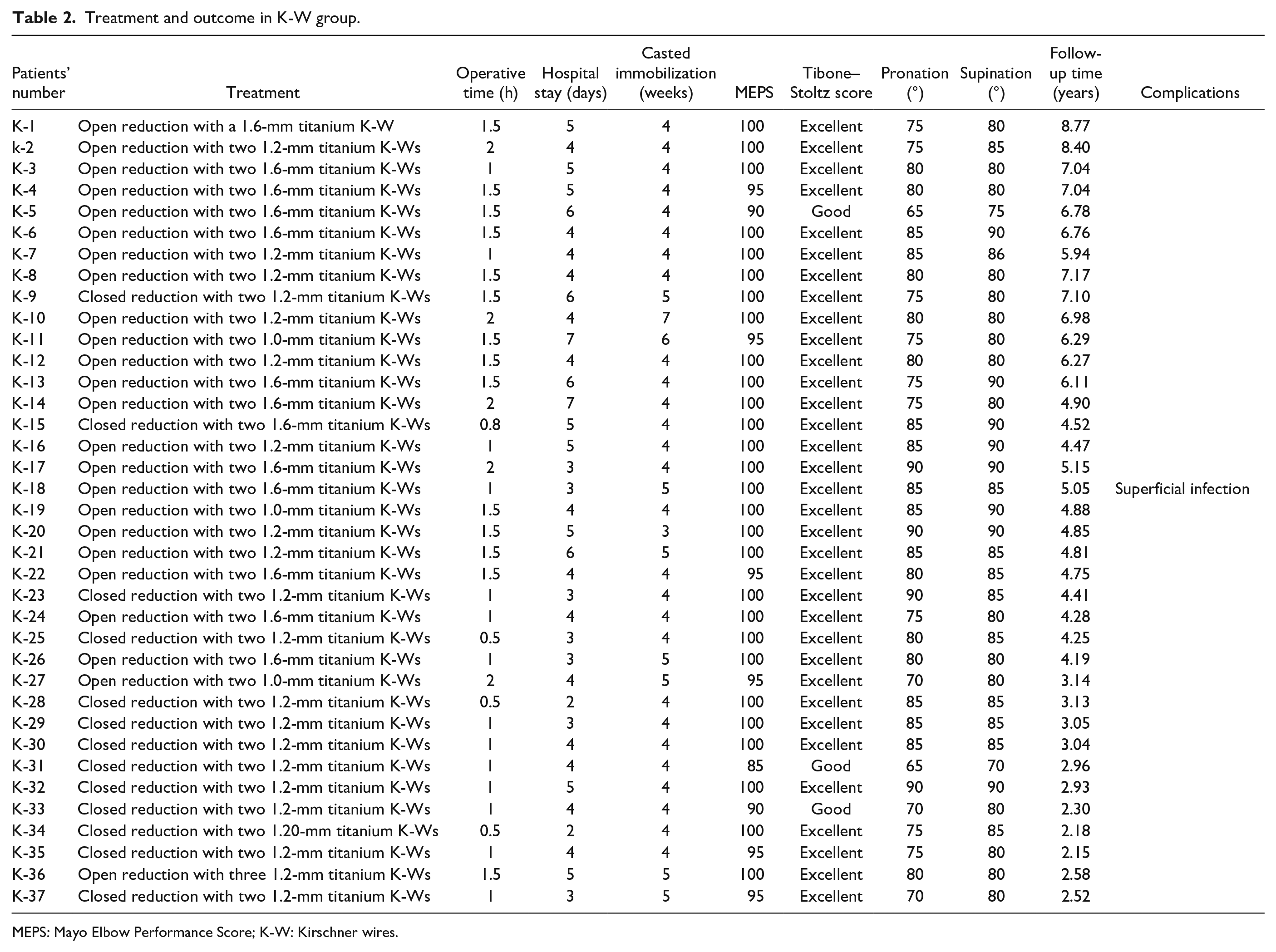
MEPS: Mayo Elbow Performance Score; K-W: Kirschner wires.
In the ESIN treatment group, there were 25 patients with 16 males and 9 females, and 21 closed reduction and 4 open reduction with a median age of 7.5 (IQR 6.0–9.3) years (Table 3). The median follow-up was 5.9 (2.7–8.5) years and the average hospital stay was 4.32 days. The average operative time was 1.30 h. The distribution of fracture severity via Judet class was as follows: 7 IIs, 15 IIIs, 2 IVa, and 1 IVb. In the group, two patients experienced skin irritation, and there were no cases of extensor pollicis longus tendon injury. The time of union ranged from 5 to 6 weeks, with an average of 5.7 weeks, and one patient with open reduction had union at 12 weeks. The average MEPS score was 97.4, with a range of 80–100 (Table 4). According to the Tibone–Stoltz classification, one patient was rated as fair, two patients as good, and the others as excellent. In one patient, there was postoperative displacement leading to malunion, and another patient had myositis ossificans around the elbow.
Patients’ characters in ESIN treatment group.
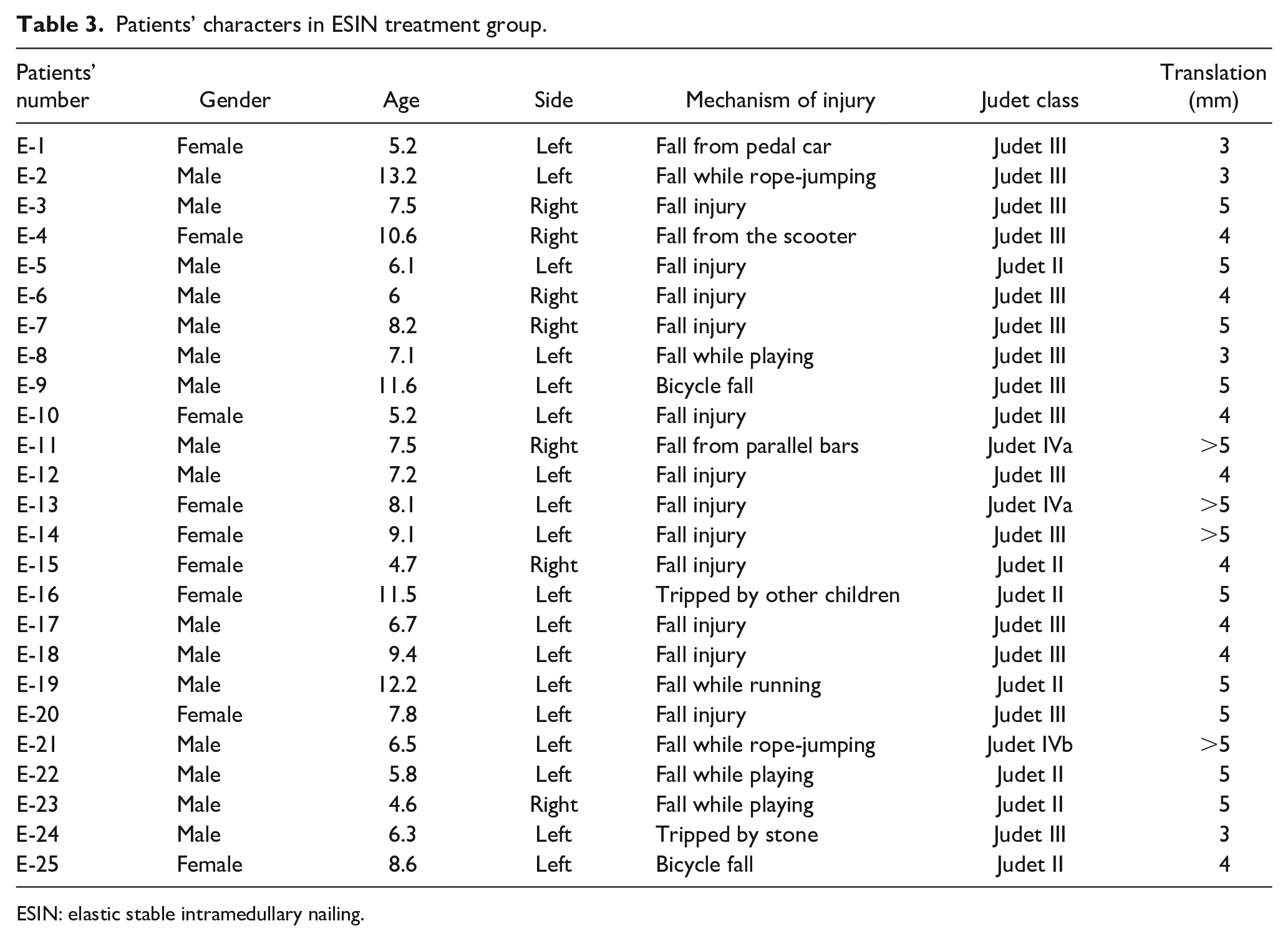
ESIN: elastic stable intramedullary nailing.
Treatment and outcome in ESIN group.
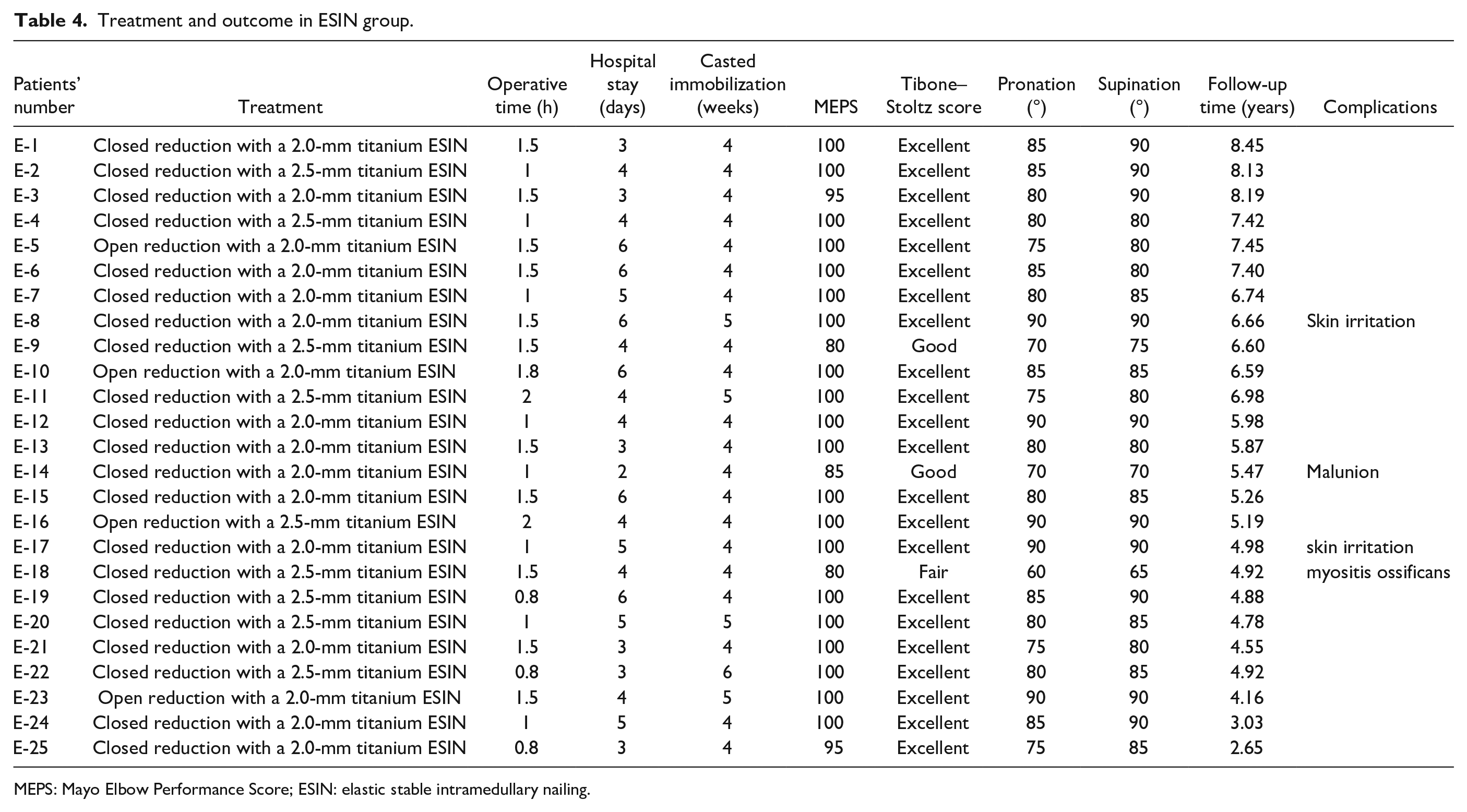
MEPS: Mayo Elbow Performance Score; ESIN: elastic stable intramedullary nailing.
Comparison between the two groups revealed no statistic differences in gender, age, Judet classification, average operative time, MEPS score, Tibone–Stoltz classification, or length of hospital stay. The pronation and supination degrees showed no significant difference between the two groups. Both ESIN and K-W internal fixation methods are reliable and satisfactory functional outcomes. However, the time of union was shorter in the K-W group than in the ESIN group (p < 0.05) (Tables 5–7). When comparing open reduction in the K-W group to closed reduction in the ESIN group, there were no statistic differences in gender, age, Judet classification, average operative time, MEPS score, Tibone–Stoltz classification, or length of hospital stay. However, in the open reduction K-W group, there was a longer average operative time and a shorter time of union. Post hoc power analysis was performed using G*Power (3.1.9.7, Dusseldorf, Germany), the outcomes in the two groups were assessed using chi-squared tests for contingency tables, and t-tests within the test family revealed the powers in this study were more than 0.8.
Comparations between the two groups.
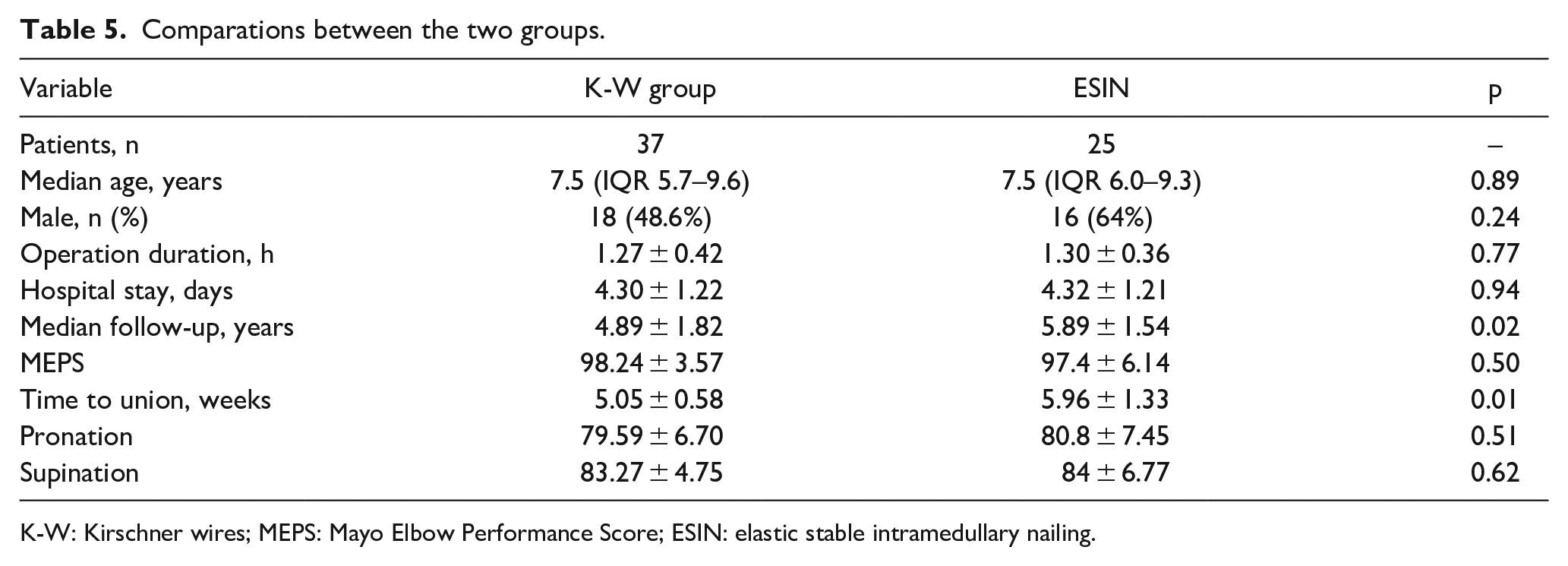
K-W: Kirschner wires; MEPS: Mayo Elbow Performance Score; ESIN: elastic stable intramedullary nailing.
Judet classification distribution of two groups.
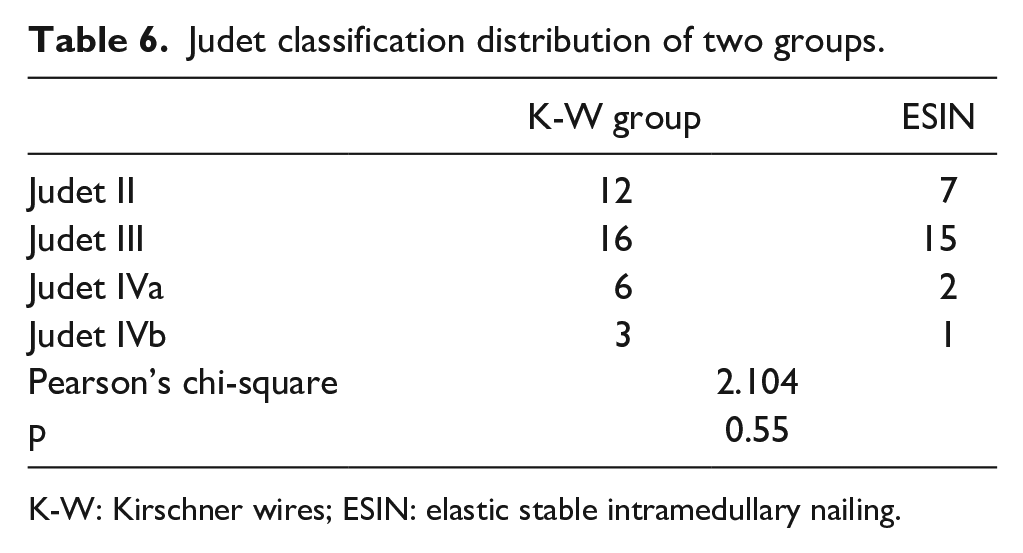
K-W: Kirschner wires; ESIN: elastic stable intramedullary nailing.
Tibone–Stoltz classification in K-W group and ESIN group.
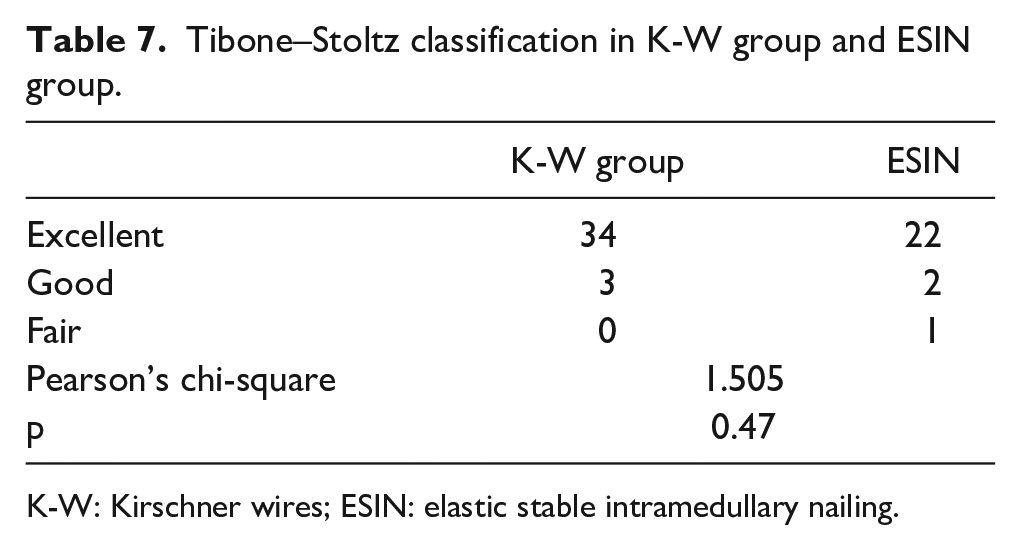
K-W: Kirschner wires; ESIN: elastic stable intramedullary nailing.
Discussion
Radial neck fracture was the third place in elbow fracture of children ranked after supracondylar and lateral condyle fractures, make up 1%–3% of all children’s fractures. 9 The mean age of injury is between 9 and 10 years in general population of children, 10 which is consistent with our research. The treatments range from non-surgical treatment to closed reduction or open reduction with internal fixation according to the angulation extent. 11 There was no study that showed which kind of displacement causes dysfunction, so most researchers suggested no more than 2 mm displacement was allowed in radial neck fracture. The radial head may lead to avascular necrosis and nonunion with significant displacement due to the anatomy structure. Operative treatment is considered when displacement remains over 2 mm, angulation is greater than 45° (age < 10 years) or greater than 30° (age > 10 years)—most importantly joint incongruity, and for open injuries. From our research data, it becomes apparent that 32% of the patients within the K-W group held a Judet II classification, while an equivalent of 28% within the ESIN group shared the same Judet II classification. The average age recorded was 8.2 years. On meticulous examination of this patient cohort’s data, it emerges that the angulation remained confined within the 30°. However, an evident displacement surpassing 50% (> 2 mm) manifested distinctly in the horizontal or lateral X-ray images. Cognizant of the potential risk inherent in deformity healing, the decision to proceed with surgical treatment has been judiciously made. Children with radial neck–limited displacement and non-surgical treatment generally result in superior outcomes compared to severely displaced fractures requiring surgical intervention. 12
K-W fixation was a traditional technique in the surgery of radial neck fracture of children, where literature had reported the clinical effect. Kalem et al. 13 reported that in 11 patients with radial neck fracture who received closed reduction with K-W fixation, 82% were excellent and 18% were good according to the Métaizeau classification. Tarallo reported that 12 cases used percutaneous reduction with K-W fixation, there were 8 excellent results and 1 fair case based on the MEPS. 14 Also, in Cha’ research, 13 pediatric patients with radial neck fractures who had received percutaneous reduction and fixation using K-W, excellent clinical results were achieved in 11 (84.6%) patients, good results in 1 (7.6%), and fair results in 1 (7.6%). 15 In our study, in the K-W group patients, the average score of MEPS was 98.2, 34 (91.9%) patients were excellent and others were good. The results were consistent with these previous studies. ESIN technique was first described by Metaizeau in 1980 and has been popularized in pediatric orthopedic surgery.4,16 In a retrospective review of 101 Judet III and IV radial neck fractures in children who underwent reduction with ESIN, there were 65.3% excellent (66 cases), 18.8% good (19 cases), 11.9% fair (12 cases), and 4.0% bad (4 cases) results in these patients. 17 In a study with 24 patients with radial neck fractures and with closed reduction and ESIN fixation, there were 23 excellent results and 1 good result based on the MEPS. 18 In another retrospective study, a total of 24 patients showed good QuickDASH score treated by ESIN. 19 In our ESIN group patients, the average score of MEPS was 97.4, 22 (88%) patients were excellent, 2 patients were good, and 1 patient was fair. The patients treated with ESIN technique had a favorable prognosis.
Between the two groups stratified by internal fixation material, there were no significant difference in the therapeutic efficacy, including MEPS scores and Tibone–Stoltz classification. This means the two kinds of surgery method are suitable for radial neck fracture in children. The healing time in K-W group was shorter than ESIN group (5 vs 5.7 weeks); but according to the previous study, healing usually occurs within 4–6 weeks, and the healing time in two groups was in the normal range. There was no difference between the Judet classification between the groups, but the rate of open reduction in the K-W group was significantly higher than that in the ESIN group. This may be due to the difficulty of K-W fixation technique with closed reduction, as it is difficult to obliquely fix the fracture line by K-W, as the proximal part of the fracture is mainly of cartilage which is small and unapparent under fluoroscopy. The forearm’s flexed and pronated position facilitates easier K-W fixation. This approach, coupled with fluoroscopic guidance, can significantly enhance the success rate of the fixation process. It is crucial to highlight that the transfixation of the radial neck with a K-W poses potential risks of severe neurological and mechanical complications, particularly the risk of PIN damage, and the formation of a bone bridge at the proximal radioulnar joint. To mitigate the possibility of PIN injury during closed reduction, it is recommended to position the forearm in a flexed and pronated state, effectively keeping the PIN away from the surgical area. In addition, caution should be exercised to prevent the penetration of the K-W tip into the adjacent ulna, minimizing the risk of further complications. This precautionary approach is essential to ensure the safety and success of the procedure while minimizing potential adverse outcomes. In open reduction patients, one case of K-W patient’s fracture healed after 7 weeks post-surgery and one ESIN patient’s fracture healed after 12 weeks. Given the limited size of the study sample, drawing a definitive conclusion about whether open reduction leads to delayed healing is challenging. Nevertheless, it remains crucial to be cautious and take measures to reduce any potential interference with the blood supply during surgical procedures. This will help ensure optimal healing conditions.
The consensus in the literature that open reduction is one of the most contributing factors for postoperative poor prognosis in patients with radial neck fracture. 20 Some scholars argued that the outcomes are most closely correlated with the injury severity, not the open reduction.21,22 In our K-W group, there were 24 patients with open reduction and 13 patients with percutaneous leverage closed reduction, the average operative time and length of hospital stay in 24 patients with open reduction were longer than patients with closed reduction, but there was no difference in MEPS and Tibone–Stoltz classification compared with two groups. The reason may be that there was no difference in Judet classification between the two groups. Our results support this conclusion that prognosis is mainly dependent on initial injury severity.
Falciglia holds the view that premature physeal closure and necrosis of the radial head are significant factors that affect the function of the elbow joint, which are closely associated with greater Judet classification, higher fracture angulation, and increased invasive interventions and iatrogenic injury. 23 Since ESIN passes through the epiphyseal line, it may lead to premature physeal closure, which is also the reason why some scholars are skeptical of this technique. However, in our ESIN group, no premature physeal closure was found, and the function of most patients was good. ESINs can not only fix fracture line but also can rotationally reduce the fracture through the elastic hook structure at the front to ensure the stability. However, there was one case of postoperative displacement, resulting in malunion, which heightened our alertness to its fixation strength. Patients with K-W fixation could have the internal fixation removed in the outpatient department after the fracture healing without a second surgical procedure of hospitalization. ESINs need to be removed under general anesthesia for a second time and with longer indwelling time, which increased the length of hospital stay and expenses, the costs are a considerable expense in developing countries. Therefore, some surgeons tend to opt for K-W fixation.
According to the mid-term follow-up of this study, the therapeutic effect of the ESIN group was not superior to that of the K-W group. Therefore, K-W fixation can also be regarded as an option for surgical treatment. Thus, it is essential to select the suitable internal fixation for pediatric orthopedic surgeons to minimize open reduction and reduce the occurrence of complications. This study is a single-center retrospective study and the research level is relatively low, a large-scale, multi-center prospective studies are required to explore the treatment effects of different methods on pediatric radius neck fractures.
Conclusion
In the management of pediatric radial neck fractures, both ESIN and K-W internal fixation have shown equivalent therapeutic results, leading to satisfactory functional outcomes. The selection of the internal fixation approach can be influenced by the patient’s fracture characteristics and the surgeon’s preferences. By minimizing repetitive reduction maneuvers and reducing the risk of vascular compromise, the combination of cast fixation contributes to positive treatment outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241233444 – Supplemental material for Comparison of elastic stable intramedullary nailing versus Kirschner wires in treatment of pediatric radial neck fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521241233444 for Comparison of elastic stable intramedullary nailing versus Kirschner wires in treatment of pediatric radial neck fractures by Kaixuan Tian, Jinchao Cao, Xinjian Pei, Yuchang Liu, Tianyou Li and Yazhou Li in Journal of Children’s Orthopaedics
Footnotes
Author contributions
K.T. involved in acquisition, analysis and interpretation of data, and originally drafted the article. J.C. performed data curation, and analysis and interpretation of the data. X.P. reviewed and edited the article. Yu.L. participated in analysis and interpretation of data, conflict of interest statement statistical expertise, and supervision. T.L. contributed to conception and design of the study, and acquisition. Ya.L. conceived and designed the work, and contributed to surgical technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of the Shandong Provincial Hospital affiliated to Shandong First Medical University, with the approval no. 2022-003. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institution and with the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Hebei Province Medical and Health Science and Technology Development Plan (grant no. 20230730).
Informed consent
Informed consent was not required as this study includes completely anonymized radiographs and no individual identifying information.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.