
Abstract
Objective
This retrospective study compared two minimally invasive surgical methods for fifth metacarpal neck fractures in adolescents: percutaneous Kirschner wire (K-wire) fixation and elastic stable intramedullary nailing (ESIN).
Methods
This study involved 42 adolescents aged 11 to 16 years with fifth metacarpal neck fractures treated by either K-wire fixation (n = 20) or ESIN (n = 22). The palmar tilt angle and shortening were compared on radiographs preoperatively and 6 months postoperatively. Total active range of motion (TAM), the visual analogue scale score for pain, and the Disabilities of the Arm, Shoulder and Hand score for upper limb function were recorded at 5 weeks, 3 months, and 6 months postoperatively.
Results
The mean TAM was significantly greater in the ESIN than K-wire group at all postoperative time points. The mean external fixation time was 2 weeks longer in the K-wire than ESIN group. One patient in the K-wire group developed infection. There was no statistically significant difference between the two groups in other postoperative outcomes.
Conclusions
ESIN fixation has the advantages of greater stability, better activity, a shorter external fixation time, and a lower infection rate than K-wire fixation in the treatment of fifth metacarpal neck fractures in adolescents.
Keywords
Introduction
The hand is one of the most vulnerable body parts of adolescents. 1 Among adolescents aged 13 to 16 years, metacarpal fractures account for about 39% of all hand fractures. 2 A fifth metacarpal neck fracture (known as a boxer’s fracture) is the most common type of hand fracture. 3 Most nondisplaced metacarpal fractures can be treated conservatively without surgery because the epiphysis of adolescents is not completely closed and has the ability to remodel. For metacarpal fractures that are angled at >30° or rotated, particularly those with a poor blood supply to the injured epiphysis, reduction surgery is required to avoid deformity during fracture healing and damage to the flexion, extension, and grasping functions of the hand. 4
Kirschner wire (K-wire) fixation is one of the most commonly performed treatments for metacarpal fractures in adolescents. An advantage of K-wire fixation in adolescents is the ease of performing the operation. However, this technique has disadvantages of poor stability, intra-articular trauma, and the need for long-term external fixation after surgery. 5 Elastic stable intramedullary nailing (ESIN) is the first-choice treatment for long bone fractures in children 6 and is now being used increasingly more often in short bones. Compared with K-wire fixation, using ESIN has the advantages of rapid recovery and a better reduction effect by minimally invasive prying of angular, rotated metacarpal fractures.
In this study, we compared the clinical outcomes of percutaneous K-wire fixation and ESIN of fifth metacarpal neck fractures in adolescents. In this way, the existing minimally invasive surgical treatment can be optimized, allowing patients to attain a better curative effect and faster postoperative recovery.
Methods
Participants
This retrospective study involved adolescent patients with fifth metacarpal fractures admitted to Jiangnan Hospital of Zhejiang Traditional Chinese Medical University during the 5-year period from January 2017 to December 2022. The inclusion and exclusion criteria are shown in the form of a patient selection flow chart in Figure 1. The inclusion criteria were an age of 11 to 16 years, a closed fracture of the fifth metacarpal neck angled at >30° (as shown by palmar oblique X-ray) and/or with rotational deformity, treatment by either percutaneous K-wire fixation or ESIN, and a follow-up time of >6 months. The exclusion criteria were open fractures, loss to follow-up, and fractures combined with vascular, nerve, and/or tendon injuries.
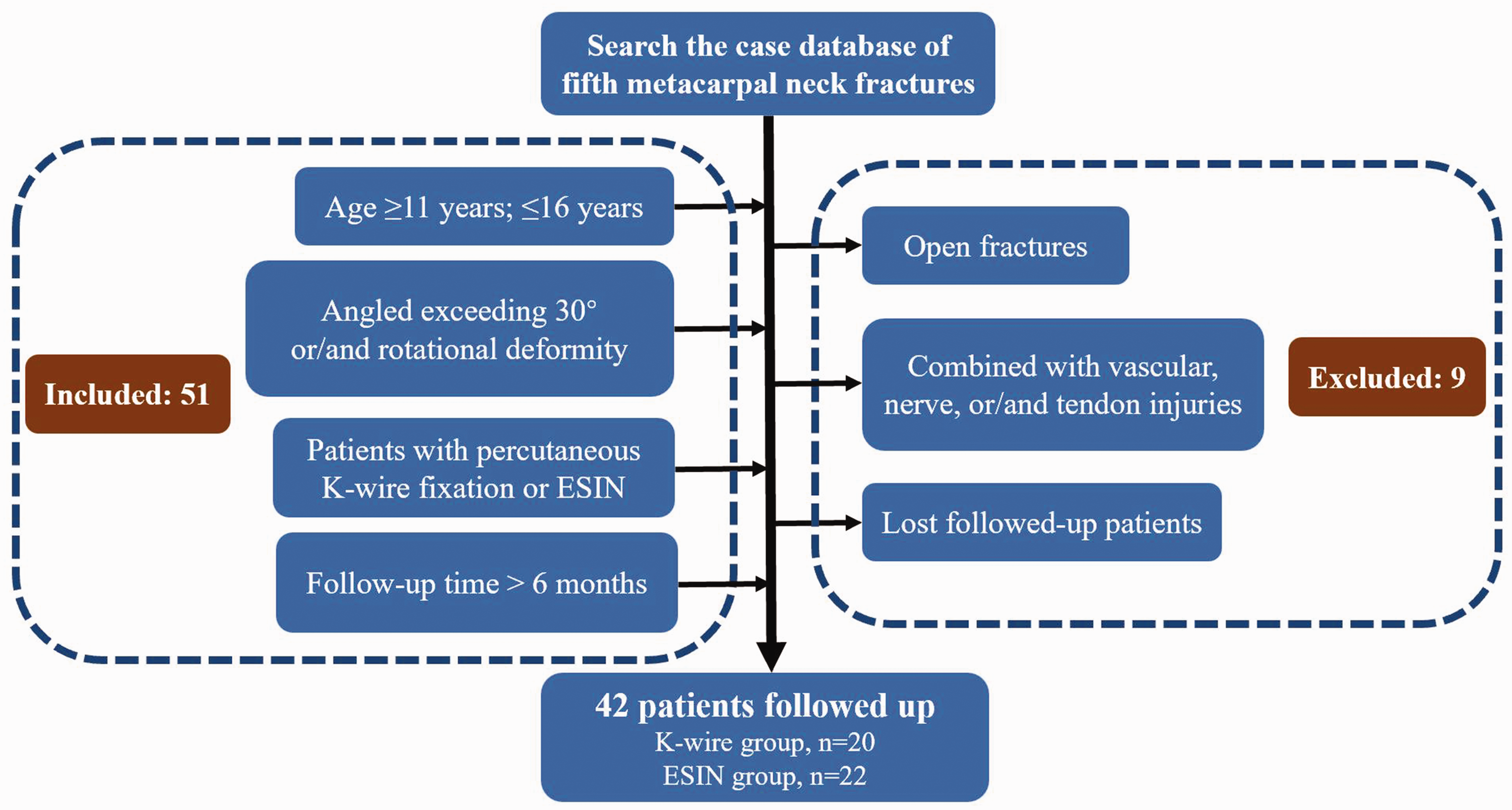
Inclusion and exclusion criteria.
Patients’ basic characteristics
After application of the above criteria, 42 patients were included in this study. Of the 42 patients, 20 underwent percutaneous K-wire fixation and 22 underwent ESIN. They comprised 28 male and 14 female patients, and 26 and 16 were right- and left-handed, respectively. Their average age was 14.13 years (range, 11–16 years; standard deviation, 1.57). All 42 patients’ fractures had been caused by sports-related accidental falls. The mean palmar tilt angle after injury was 45.82° ± 4.34°, and the mean shortening was 3.12 ± 0.33 mm. All 42 patients’ fractures were angled at >30°, and 21 patients’ fractures exhibited rotational displacement. The mean time from injury to surgery was 4.69 ± 0.64 days (Table 1).
Patients’ basic characteristics.
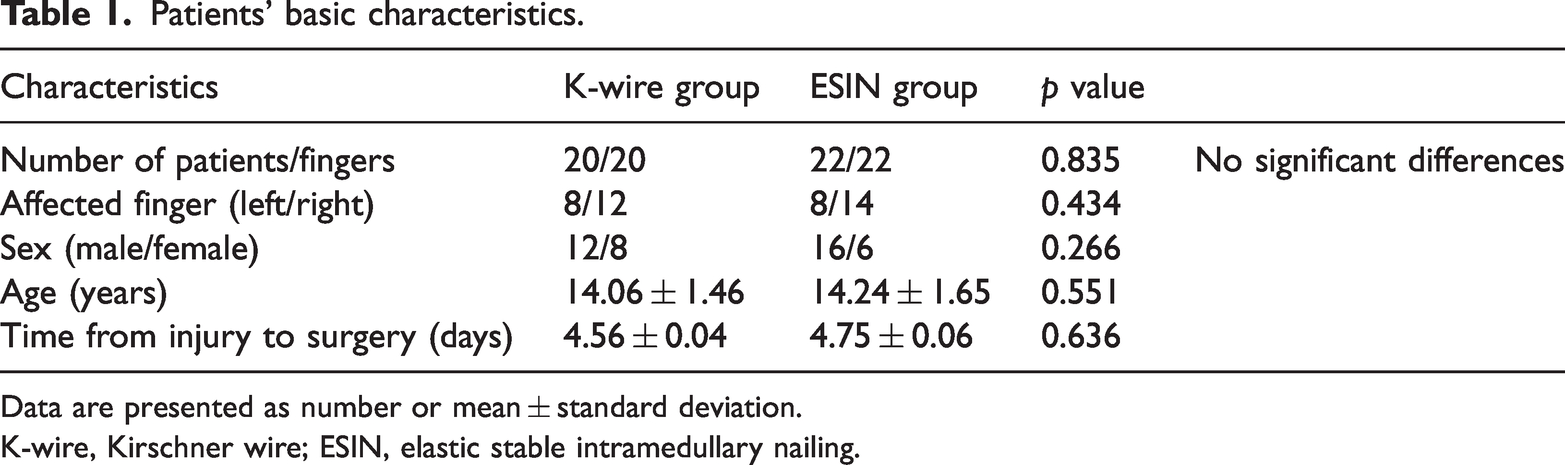
Data are presented as number or mean ± standard deviation.
K-wire, Kirschner wire; ESIN, elastic stable intramedullary nailing.
This retrospective study was approved for publication by the ethics committee of Jiangnan Hospital Affiliated to Zhejiang Chinese Medical University (Hangzhou Xiaoshan Hospital of Traditional Chinese Medicine) (XSZYY2081121), and the study was conducted in accordance with the tenets of the Declaration of Helsinki. All patients agreed to participate, provided written informed consent prior to treatment, and signed a consent form for publication of all data and accompanying images. All patients’ details have been de-identified. Copies of the written consent forms are available for review by the editors of this journal. The reporting of this study conforms to the STROBE guidelines. 7
Treatment methods
Preoperative treatment
After admission, each patient received symptomatic treatment such as analgesia and detumescence therapy. All patients underwent preoperative examinations to assess their surgical risk.
Percutaneous K-wire fixation
After assessment of the surgical indications (fracture angle of >30° and/or rotational deformity), brachial plexus anesthesia was administered and the Jahss maneuver 8 was applied for reduction. A K-wire of either 1.2- or 1.5-mm diameter was inserted from the distal aspect of the fifth metacarpal bone to the proximal end until it penetrated through the fracture line. Cross fixation was performed, and the metacarpophalangeal joint was passively moved after the reduction was deemed satisfactory by C-arm fluoroscopy. It was confirmed that the K-wire did not penetrate the tendon. Postoperative plaster immobilization was performed for 6 weeks, and digital radiography films were reviewed every 2 weeks. When the fracture had healed, usually by 6 weeks postoperatively, the K-wire could be removed.
ESIN
After assessment of the surgical indications (fracture angle of >30° and/or rotational deformity), brachial plexus anesthesia was administered and the Jahss maneuver was applied for reduction. The skin was sterilized, and an approximately 1-cm incision was made at the base of the metacarpal bone. A 2.0- or 2.5-mm elastic stable intramedullary nail was selected according to the thickness of the metacarpal bone. Under C-arm monitoring, the initial entry point was selected at the base of the metacarpal. A drill was advanced about 0.5 cm into the bone, and the blunt end of the intramedullary nail was inserted in an antegrade manner. The fracture was reduced when the wire passed across the fracture site but not through the growth plate. The intramedullary nail could be slightly rotated to fine-tune the fracture reduction. The C-arm was used to check the extent of fracture reduction, whether the nail was in the medullary cavity, and whether the fracture was well aligned (Figure 2). The fingers were flexed to observe whether two to four fingers were crossed or rotated. When the condition of the fingers was satisfactory, the intramedullary nail was cut, leaving a 2- to 3-mm length of nail outside the cortical bone to prevent irritation; the wound was then closed (Figure 3). The affected limb was fixed with a cast for 4 weeks, and digital radiography films were reviewed every 2 weeks.

Intraoperative radiological observation.

Elastic stable intramedullary nailing wound.
Postoperative rehabilitation activities were conducted under the guidance of a doctor. After 3 to 5 days, wound healing was assessed and X-ray examination was performed to review the fracture reduction.
Observations
The primary outcomes were total active range of motion (TAM), the visual analogue scale (VAS) score for pain, and the Disabilities of the Arm, Shoulder and Hand (DASH) score for upper limb function. We also evaluated the operating time and the number of complications. The secondary outcomes were the palmar tilt angle and shortening deformity. All patients were followed up for 6 months. We evaluated the VAS score 1 week postoperatively. We compared the radiological parameters, including the palmar tilt angle and shortening deformity, before surgery and after bone union between the two treatment groups. The TAM, VAS score for pain, and DASH score for upper limb function (Figure 4) were collected and compared at 5 weeks, 3 months, and 6 months postoperatively in both groups.

DASH score, Disabilities of the Arm, Shoulder and Hand.
Statistical analysis
The Mann–Whitney U test was performed to analyze age and the duration to bone union, and the chi-square test was performed to analyze sex; all differences were compared between the K-wire and ESIN groups. The unpaired Student’s t test was used to compare the differences in the radiological parameters, TAM, VAS score for pain, and DASH score for upper limb function between the two groups. A p value of <0.05 was considered statistically significant. The statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) version 11.0 (SPSS Inc., Chicago, IL, USA).
Results
All 42 patients were followed up for 6 to 12 months (mean, 8.68 ± 1.30 months). There were no significant differences between the K-wire and ESIN groups in the mean palmar tilt angle (42.43° ± 3.34° vs. 48.33° ± 2.64°, respectively) or shortening (3.18 ± 0.14 vs. 3.08 ± 0.19 mm, respectively) (Table 2).
Preoperative radiological data.

Data are presented as mean ± standard deviation.
K-wire, Kirschner wire; ESIN, elastic stable intramedullary nailing.
The mean operating time in the ESIN group (38.32 ± 4.23 min) was slightly longer than that in the K-wire group (31.45 ± 6.34 min). The mean VAS score for pain at 1 week postoperatively was 1.82 ± 0.04 in the ESIN group and 1.87 ± 0.04 in the K-wire group, with no significant difference. Postoperative radiographic examination showed that all patients in the study had achieved bone union at around 5 weeks, with no significant difference between the two groups (Figures 5, 6). Additionally, both methods were shown to effectively correct angulation and shortening, with the ESIN and K-wire groups showing postoperative angulation of 4.6° ± 0.03° and 5.2° ± 0.04°, respectively, and postoperative shortening of 0.82 ± 0.02 and 0.53 ± 0.04 mm, respectively. The American Society for Surgery of the Hand TAM (ASSH-TAM) joint flexion angle measurement score at 5 weeks postoperatively was significantly greater in the ESIN group (220.87° ± 8.94°) than in the K-wire group (130.66° ± 9.34°) (p < 0.001). The ASSH-TAM joint flexion angle measurement score was also significantly different between the ESIN and K-wire groups at 3 months postoperatively (248.67° ± 9.38° vs. 225.36° ± 8.76°, respectively; p < 0.001) and 6 months postoperatively (251.48° ± 4.11° vs. 230.23° ± 6.23°, respectively; p < 0.001). The DASH score for upper limb function at 5 weeks postoperatively was significantly better in the ESIN group (3.23 ± 0.03) than in the K-wire group (5.45 ± 0.05) (p < 0.001). However, the DASH score was not significantly different between the ESIN and K-wire groups at 3 months (1.31 ± 0.03 vs. 1.37 ± 0.02, respectively) or 6 months (0.87 ± 0.03 vs. 0.94 ± 0.03, respectively). The mean duration of external fixation was 2 weeks shorter in the ESIN than K-wire group (4 vs. 6 weeks, respectively). One patient in the K-wire group developed a wound infection, whereas no complications occurred in the ESIN group (Table 3).
Postoperative results.

Data are presented as mean ± standard deviation or number.
No significant differences were found between the two groups except in the ASSH-TAM scores at 5 weeks, 3 months, and 6 months postoperatively and the DASH scores at 5 weeks postoperatively. Only one complication occurred in the K-wire group.
K-wire, Kirschner wire; ESIN, elastic stable intramedullary nailing; VAS, visual analogue scale; ASSH-TAM, American Society for Surgery of the Hand total active range of motion; DASH, Disabilities of the Arm, Shoulder and Hand.

Five-week-postoperative radiographic image of a patient treated with K-wire fixation

Radiographic images of a 13-year-old boy treated with ESIN. (a) Preoperatively. (b) Five weeks postoperatively and (c) Six months postoperatively (after taking out the nail).
Discussion
In this retrospective study, we compared two minimally invasive surgeries for the treatment of fifth metacarpal neck fractures in adolescents. Because the bones of adolescents are still in the growth stage and have a unique physiological structure, and because fractures of the neck of the fifth metacarpal are morphologically unique, our observational indicators focused on whether adolescents are at risk of unique complications such as premature epiphyseal closure during the postoperative healing stage. The characteristics of fifth metacarpal neck fractures in adolescents and the curative effects of the two treatment methods as revealed in this study are discussed below.
Characteristics of metacarpal fractures
The metacarpal bones are the key bony factors in the three arcuate structures of the hands, which comprise the carpal bones, metacarpal bones, and phalanges from the fingertips to the wrist. These structures are mostly arcuate because of the traction produced by the tendons. Metacarpal neck fractures often occur in the second and fifth metacarpal bones, whereas metacarpal shaft fractures are more common in the third and fourth metacarpal bones. Studies have shown that when the metacarpal bone is shortened by 2 cm, the extension function of the palm will correspondingly decrease by about 7°. 9 The palmar aspect of the metacarpal neck is the weakest area of the metacarpal bone and therefore also a common site of comminuted fractures. An important factor for successful reduction of metacarpal fractures is the muscle proper. A strong muscle proper can cause metacarpal deformity in the sagittal plane, but when the metacarpophalangeal joint is flexed, the force of the muscle proper can be counteracted. At the same time, because of the thin skin on the back of the palm, metacarpal fractures can easily cause damage to tissues such as skin, nerves, and tendons; such damage may cause blood supply disorders and lead to avascular necrosis. Metacarpal fractures are likely to result in a local bulge, pain, and limited movement of the fingers because of the unbalanced tension in the flexor and extensor tendons.
Comparison between ESIN and K-wire fixation
Our study shows that ESIN is superior to percutaneous K-wire in terms of postoperative functional recovery. Although preoperative angulation and shortening improved and all fractures in both groups healed, patient satisfaction with comfort overwhelmingly supported ESIN. The mean operation time of percutaneous K-wire fixation was shorter than that of ESIN. The percutaneous K-wire operation is simpler than the ESIN operation; currently, the former technique is more frequently performed as surgeons are more proficient at it. However, in terms of the range of motion of the metacarpophalangeal joint at 5 weeks, 3 months, and 6 months postoperatively, ESIN is clearly superior to K-wire fixation. At all three postoperative time points after ESIN in this study, the range of motion was close to that of normal joints (Figure 7). The reason for this is that unlike ESIN, K-wire fixation damages the articular surface. Similarly, in terms of upper extremity functional recovery, ESIN was also superior to K-wire fixation at 5 weeks postoperatively. Although the DASH scores of the two groups at 3 and 6 months postoperatively tended to be the same, these findings still indicate that ESIN for treatment of metacarpal fractures has the advantage of rapid functional recovery. Additionally, patients in the ESIN group returned to school or the community 16 days earlier than patients in the K-wire group. Among all 42 patients, only 1 case of wound infection occurred in the K-wire group. This was related to the direct connection between the K-wire and the external body during percutaneous K-wire fixation, increasing the risk of infection.

(a, b) Joint flexion of ESIN group at 5 weeks. (c, d) Joint flexion of ESIN group at 3 months
Therefore, compared with percutaneous K-wire fixation for juvenile metacarpal fractures, ESIN has the following four advantages: (1) high stability of internal fixation, especially against transverse and longitudinal forces; (2) less intra-articular trauma, resulting in less impact on juvenile epiphyseal development and later functional recovery; (3) a short external fixation time and early recovery of function; and (4) no connection of internal fixation device to external fixation device, decreasing the risk of wound infection.
Notably, however, percutaneous K-wire fixation has the following advantages: (1) simple operation and short operation time, (2) strong resistance to rotation and displacement, (3) no need for a secondary operation to remove the internal fixation device, and (4) low surgical cost.
Literature review
As one of the most classic surgical methods for the treatment of fractures of the fifth metacarpal neck, percutaneous K-wire fixation has a certain degree of popularity worldwide. Although it has also been confirmed to have a certain degree of stability in some previous biomechanical studies, its ability to resist fracture displacement is not one of its advantages over other surgical methods such as plate-and-screw internal fixation and cortical nail internal fixation.10,11 Additionally, when K-wire fixation is used to treat metacarpal neck fractures, the K-wire must pass through both the articular surface and growth plate. When K-wires pass through the epiphysis, the epiphyseal growth may be affected. 12 Furthermore, the size, location, number of passes, and number of K-wires may lead to epiphyseal damage during surgery. The structure of epiphyseal rods may also lead to complications of epiphyseal growth. A drill injury of 7% to 9% of the epiphyseal cross-sectional area was found to be sufficient to cause growth retardation. 13 Although a small central disruption of the epiphysis is not thought to alter the growth of the epiphysis, 14 K-wires that pass through the center and periphery of the epiphysis appear to have the same risk as that associated with rods. 13 One study showed that K-wire fixation did not increase the risk of growth arrest and that epiphyseal injury at the end of the growth stage did not alter the limb axis. 15 No consensus has been reached regarding the effect of K-wires on epiphyseal injury. When ESIN is used to treat metacarpal fractures, there is no need to cross the growth plate and there is little damage to the epiphysis.
Increasingly more surgeons are using ESIN to treat metacarpal fractures, and many reports have described the advantages of this technique. Through a follow-up of 27 cases, She and Xu 16 found that the use of anterograde elastic single intramedullary nails in the treatment of fifth metacarpal neck fractures led to earlier functional exercises and better functional recovery. Mirza et al.17,18 treated 17 patients with prefabricated intramedullary nails and found that the use of elastic intramedullary nails for metacarpal fractures had the advantage of avoiding nerve and tendon injury. Additionally, through a summary of the postoperative imaging and joint range of motion of 55 cases, they found that ESIN treatment of metacarpal fractures could provide early restoration of joint range of motion and had a low incidence of complications. Shen et al. 19 summarized 69 cases of elastic intramedullary nails for the treatment of juvenile fifth metacarpal neck fractures and proposed that anterograde insertion of elastic intramedullary nails has strong stability, induces minimal trauma, and results in almost no damage to the juvenile epiphysis. In a study by Lieber et al., 20 one patient developed nerve and tendon injury due to excessive pursuit of ESIN stability, and the authors cautioned that attention should be paid to the distance between the ESIN head and the articular surface when the ESIN needle is inserted. Compared with microplate fixation, elastic intramedullary nail fixation allows for easier reduction of fractures and avoids excessive peeling of the periosteum; this allows the periosteum to fully form bone and facilitates scab formation to promote fracture healing. Moon et al. 21 reported that compared with K-wire fixation, elastic intramedullary nailing does not require additional fixation, allows for rapid progression to functional exercises, and shortens the average recovery time. Zeng et al. 22 found that using dual intramedullary nails can help patients return to activity earlier than when using a single intramedullary nail. Ghazala et al. 23 compared the lockable intramedullary nail with the ordinary intramedullary nail and found that the former further strengthened the stability of fixation and optimized the ESIN technique (Table 4).
Literature review.

ROM, range of motion; VAS, visual analogue scale; DASH, Disabilities of the Arm, Shoulder and Hand; TAM, total active range of motion; ESIN, elastic stable intramedullary nailing; MCP, metacarpophalangeal.
Limitations of the study
This study had two main limitations. First, because this was a retrospective study, the integrity and homogeneity of the clinical data cannot be guaranteed. We plan to conduct prospective studies on ESIN surgical methods to improve the quality of the data and conclusions. Second, the lack of self-comparison with the degree of shortening and joint mobility of the healthy side may have led to some errors in the results.
Conclusion
This retrospective study has shown that both ESIN and percutaneous K-wire fixation are effective in the treatment of fifth metacarpal neck fractures in adolescents. ESIN for metacarpal fractures has the advantages of minimal invasiveness, stability, minimal intra-articular trauma, a low risk of infection, and a good prognosis, although it has the disadvantage of relatively poor anti-rotation ability. However, comparison of the pros and cons leads to the conclusion that ESIN is a safe, efficient, and convenient treatment. Compared with other common surgical fixation methods, it has its unique advantages and may be promoted in clinical practice.
Footnotes
Author contributions
Kai Wang and Changzong Deng collected the data and wrote the manuscript. Kai Wang was a major contributor to writing the manuscript. Ningrui Hu, Weibin Du, and Wei Zhuang contributed to the conception and design of the study. All authors read and approved the final manuscript.
Declaration of competing interests
All the authors declare that they have no conflicts of interest.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This work was supported by the Zhejiang Medical and Health Science and Technology Project (No. 2019KY547), the Hangzhou Medical and Health Science and Technology Project (No. OO20191129), the Hangzhou Health Science and Technology Project (No. B20210628), and the Hangzhou Health Science and Technology Project (No. B20210140).