
Abstract
Purpose:
The elastic stable intramedullary nail has been recognized as an accepted technique for treating pediatric long bone fractures. The principle of the technique is “3-point support and fixation,” and it should be followed to achieve the optimum outcome without implant failure and complications. However, tools have yet to be reported for pre-bending of the elastic stable intramedullary nail. This study aims to present a novel tool for pre-bending the elastic stable intramedullary nails and the results of using this tool by surgeons.
Methods:
A designed case of femoral shaft fracture was provided to the participants. All participants were divided into three groups according to their experience with the elastic stable intramedullary nail technique: resident, fellow, and attending groups. The time of completing the pre-bending and coronal plane deviation of the nails after pre-bending was recorded. Statistical analysis compared the data in a conventional way and with the new tools in each group.
Results:
A total of 30 physicians were recruited in this study. The pre-bending duration with the new tool was significantly shorter than that of the conventional method for all physicians (p
Conclusion:
This novel tool for elastic stable intramedullary nail pre-bending was convenient and easy to use in achieving the principal role of the elastic stable intramedullary nail technique. Physicians could reduce the coronal plane deviation when pre-bending elastic stable intramedullary nails, especially for physicians with less experience with the elastic stable intramedullary nail technique.
Level of evidence:
IV.
Introduction
With the development of various surgical techniques in the past 20 years, the elastic stable intramedullary nail (ESIN) has been recognized as an accepted technique for treating pediatric long bone fractures and is adopted by many pediatric orthopaedic surgeons.1,2 This technique is considered to be minimally invasive, with the advantages of shorter hospital stay and early ambulation, resulting in rapid recovery.3 –5 The principle of the technique is “3-point support and fixation” of the bone.6,7 In order to achieve adequate fixation, nails should be accurately pre-bent as an essential prerequisite. Generally, the nail should be bent in a C-shaped manner and approximately three times the diameter of the long bone at its isthmus at which the nail is to be inserted. The apex of the curvature should be a 40° radius to position, with a maximal curve at the level of the fracture site.6,8 –11 This principle must be followed to achieve the optimum outcome without implant failure and complications, such as angulation.7,11
However, a tool has yet to be designed for optimum nail bending. Surgeons must bend the nails by hand or use other tools not designed for this purpose. No method has been introduced to evaluate whether the nails are pre-bended accurately and follow the “3-point support and fixation” principle.7,11 This study aims to present a newly designed tool for pre-bending the ESINs and compare the results achieved using this tool by different groups of surgeons with varying levels of experience with the ESIN technique.
Patients and methods
A designed case of femoral shaft fracture was provided to the surgeons who participated in this study. The length of the femoral shaft was 20 cm, with a diameter of 1 cm. The distance from the fracture site to the intertrochanteric area was 7 cm. The participants were asked to use two nails of 4 mm diameter, bend the nails in a C-shape, approximately 3 cm from the tip of the nail to the apex of the curve, and keep the apex at the fracture site according to the requirements of the ESIN technique.6 –11 The shape of the fractured femur and all related information, including detailed instructions about how and where to pre-bend the nails, were printed on the paper provided to the participants to check whether they achieved accurate pre-bending to follow the principle (Figure 1). This study was performed in line with the principles of the Declaration of Helsinki, approved by the authors’ Institutional Review Board (IRB) institution. Each participant signed the informed consent.
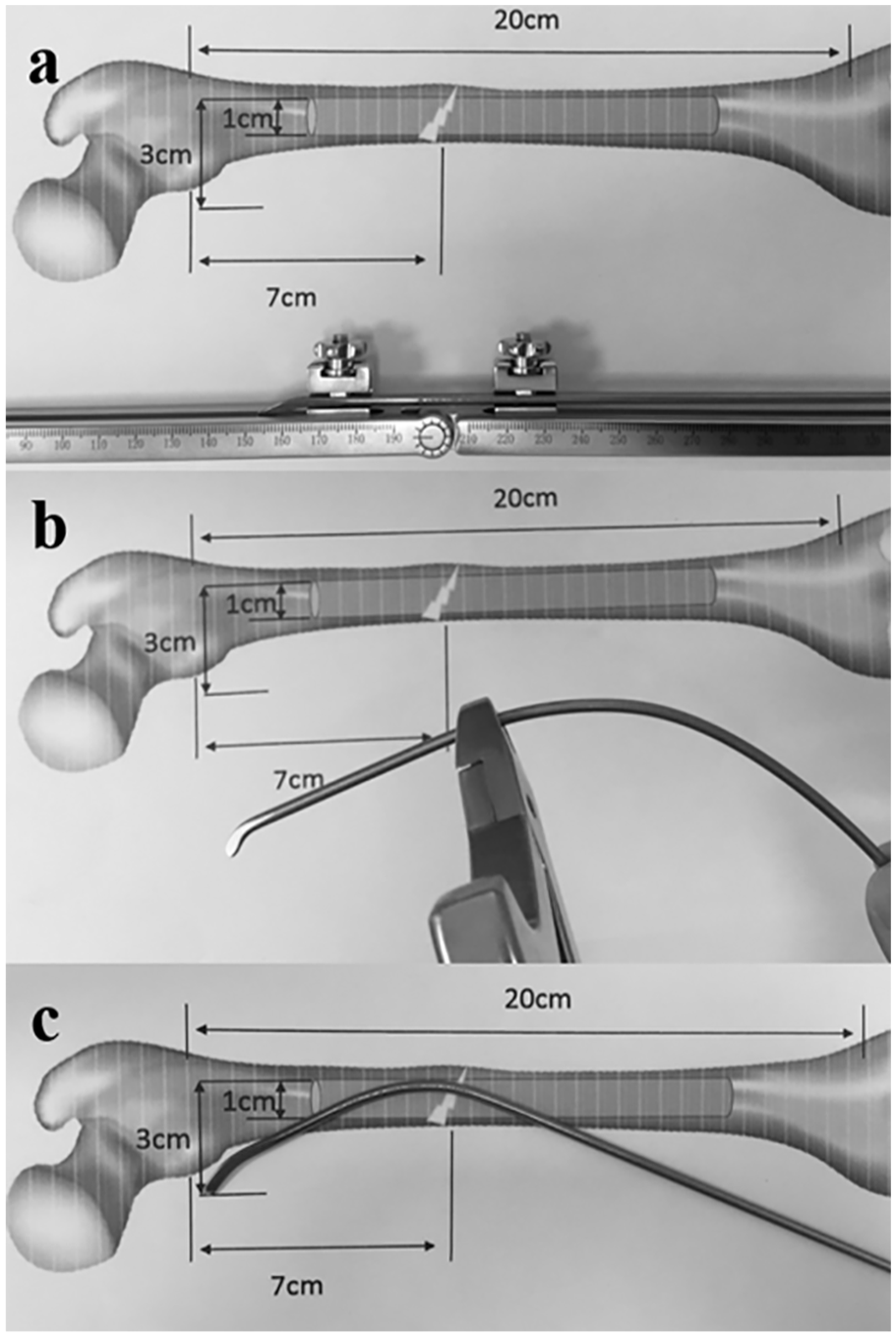
A designed case with femoral shaft fracture; the length of the femoral shaft was 20 cm with a diameter of 1 cm. The distance from the fracture site to the intertrochanteric area was 7 cm. The nails should be 4 mm in diameter. All participants pre-bent the 4- mm ESIN with (a) the new tool or (b) with a pair of pliers in the ESIN tools box in the conventional way. The nail should be formed in a (c) C-shape, about 3 cm from the tip of the nail to the apex of the curve according to the requirements of the ESIN technique.
The participants were divided into three different groups according to their experience with the ESIN technique: (1) Resident group: Surgeons who have never performed surgery using ESIN or have been performing surgery using ESIN but fewer than 10 cases; (2) Fellow group: Surgeons who have been performing surgery using ESIN but performed only 10–50 cases; and (3) Attending group: Surgeons who have been performing surgery using ESIN and performed over 50 cases. Each participant was asked to bend the 4-mm titanium nails (Double Medical, Xiamen, China) to achieve the required shape according to the “3-point support and fixation” principle four times. At first, they were asked to bend the ESIN using the newly designed tool for pre-bending twice (Figure 1). Finally, they were asked to bend the ESIN using a pair of pliers in the ESIN toolbox in a conventional way twice. The completion time of pre-bending the nails after pre-bending was recorded in seconds by two observers on average. The coronal plane deviation was defined as 0–4 levels according to the deviation number of centimeters after pre-bending (Figure 2). The deviation levers were checked by two observers and recorded to see whether their results were consistent. Otherwise, a third observer would check again and make the final decision. The observers were not involved with the authors of this research.
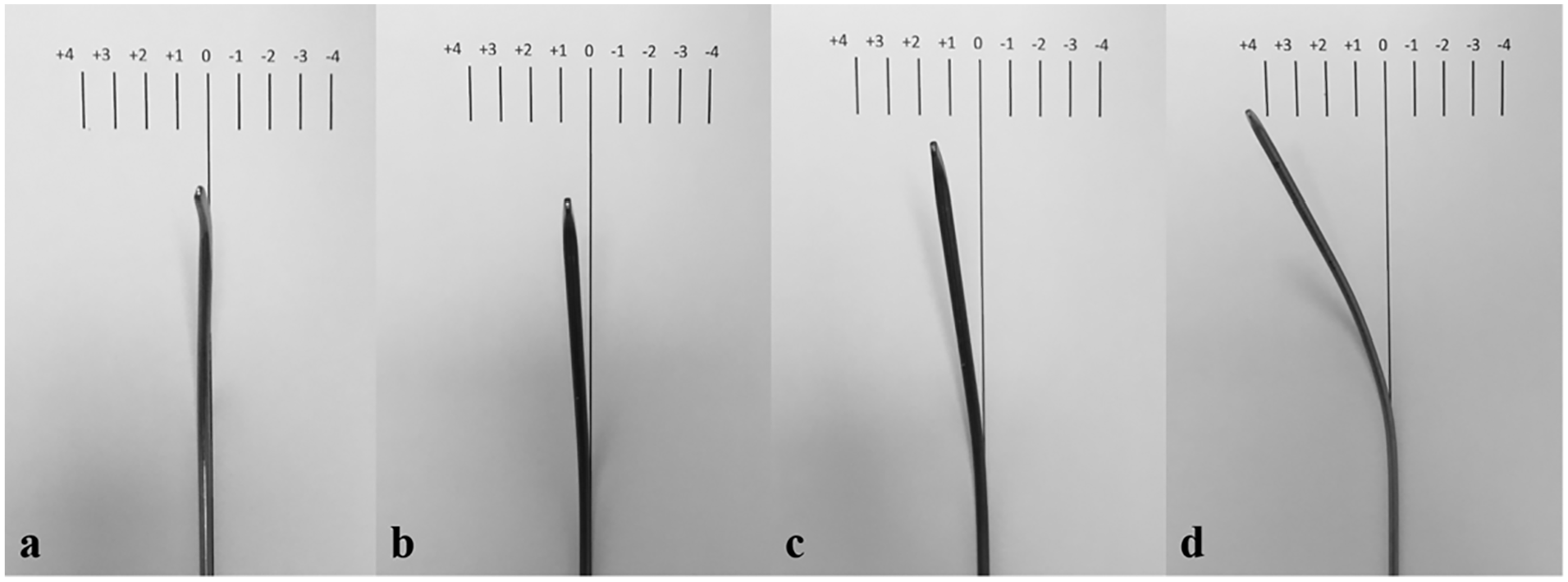
ESINs coronal plane deviation was defined as level 0: (a) no coronal plane deviation, (b) less than 1 cm, (c) less than 2 cm, and (d) over 2 cm according to the deviation number of centimeters after pre-bending.
Technique
The new pre-bending tool is composed of two stainless steel levers with scale and connected by a shaft with a rotating angle from 80 to 280° (Figure 3). The nail is fixed on each lever by a clip attached to the lever, which can be slid into the lever slot. The 3-point support and fixation principle and the methods of the new pre-bending tool were demonstrated to each participant before their pre-bending task, and each participant claimed that they had understood the process thoroughly. When pre-bending a nail, the surgeon should fix the nail with the clip so that the nail bends at the desired length with the appropriate curvature. After fixation, the nail was slowly bent by pulling the lever in order to achieve an appropriate curvature in a C-shaped manner so that it followed the principle of the ESIN technique (Figure 3). The pulling distance of the tip of the nail was almost equal to the distance calculated by the formula (Figure 4). Pre-bending is complete when the pulling distance of the tip of the nail becomes almost equal to the distance calculated using the formula. Both clips are then loosened, and the nail is removed and made ready for insertion.
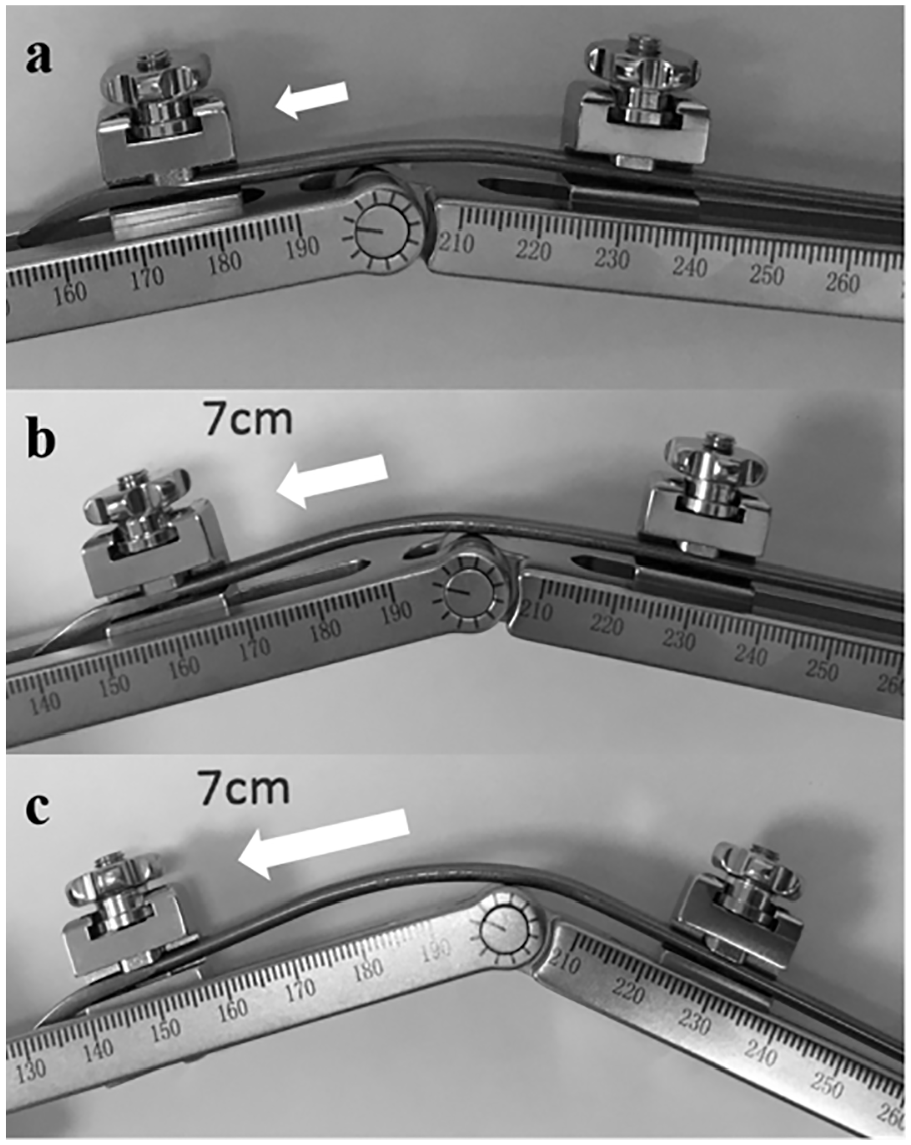
The procedure of pre-bending a nail: (a) the tip of a nail was fixed in the left clip and ensured that the nail across the right clip stands on the sagittal position, (b) then pull the left clip with the tip of the nail away from the shaft and bend the nail by two levers slowly. (c) If the pulling distance of the tip of the left nail was almost equal to the distance calculated by the formula, the pre-bending was completed.
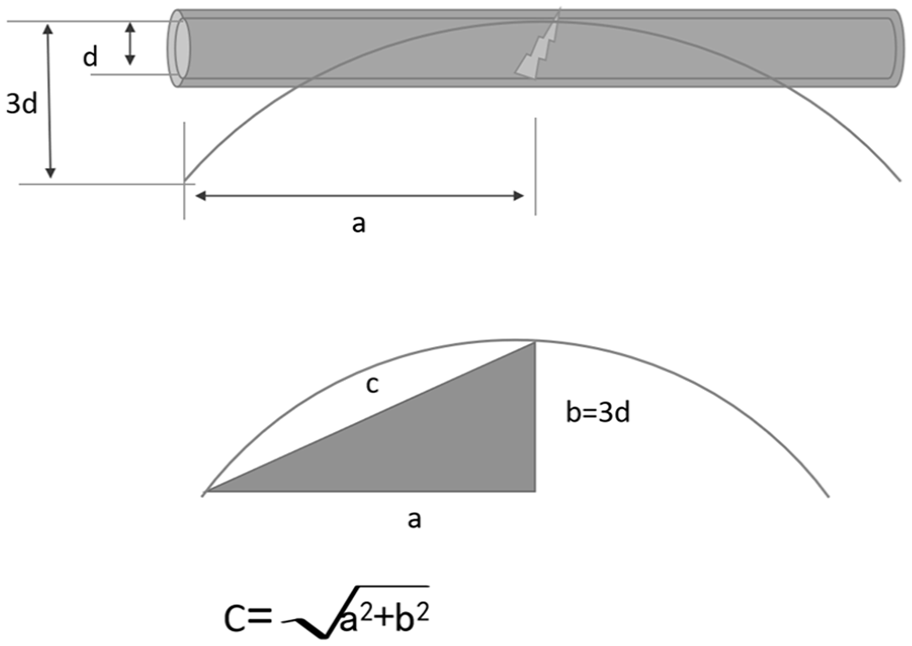
The nail should be formed in a C-shaped manner, about 3-times (b) the diameter of the long bone (d), which the nails insert from the tip of the nail to the apex of the curve (a) according to the requirements of ESIN technique. The pulling distance of the tip of the nail was almost equal to the distance calculated by the formula (c).
Statistical analysis
The time to complete pre-bending and coronal plane deviation data was compared between the conventional and new tool in each group. Statistical analysis was performed using the paired-sample T test and analysis of variance (ANOVA) with SPSS (version 22.0; SPSS, Chicago, IL, USA). The level of significance was set at p
Results
A total of 30 surgeons, including 10 surgeons in each group, were recruited in this study and completed four times pre-bending as required. The time taken to complete pre-bending in the three groups is shown in Table 1. The pre-bending duration with the new tool was significantly shorter than that of the conventional method for all surgeons in each group (p
The time of completing pre-bending in three groups (s).
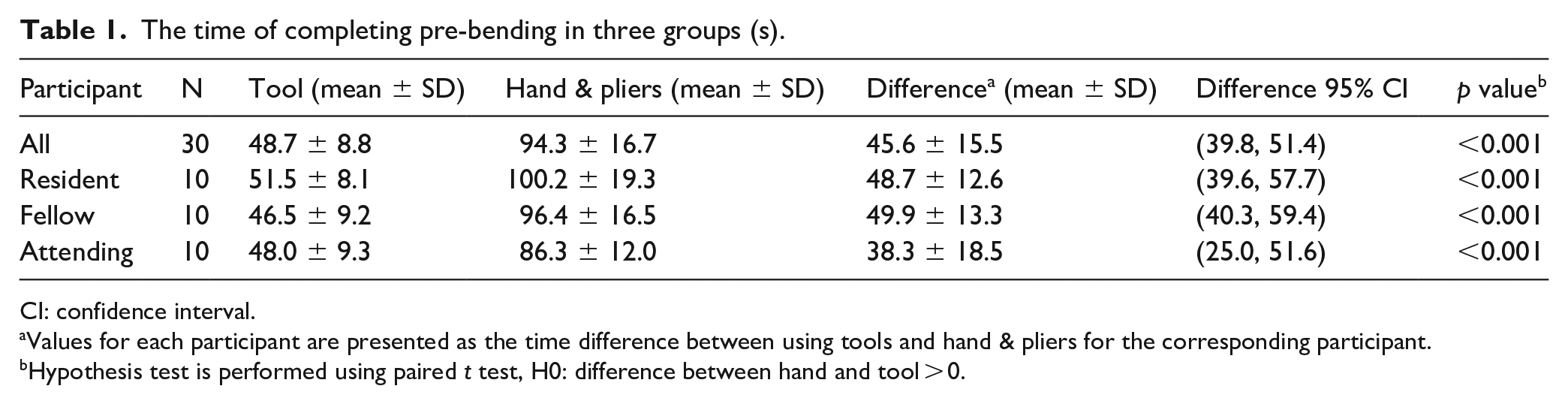
CI: confidence interval.
Values for each participant are presented as the time difference between using tools and hand & pliers for the corresponding participant.
Hypothesis test is performed using paired t test, H0: difference between hand and tool > 0.
The coronal plane deviation of nails after pre-bending in three groups (cm).
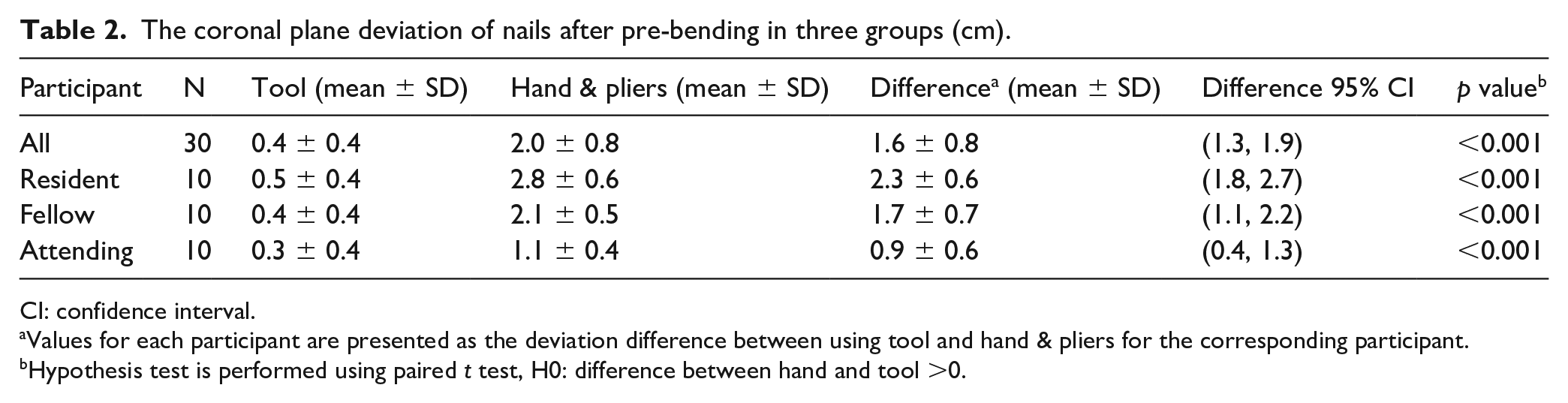
CI: confidence interval.
Values for each participant are presented as the deviation difference between using tool and hand & pliers for the corresponding participant.
Hypothesis test is performed using paired t test, H0: difference between hand and tool >0.
No statistically significant difference in completion time was observed among the three group of surgeons, whether using the new tool (p = 0.16) or by hand (p = 0.45) in Table 3. The coronal plane deviation of nails after pre-bending by hand in each group show statistically significant differences (p
The comparison of completing time and coronal plane deviation among three groups.
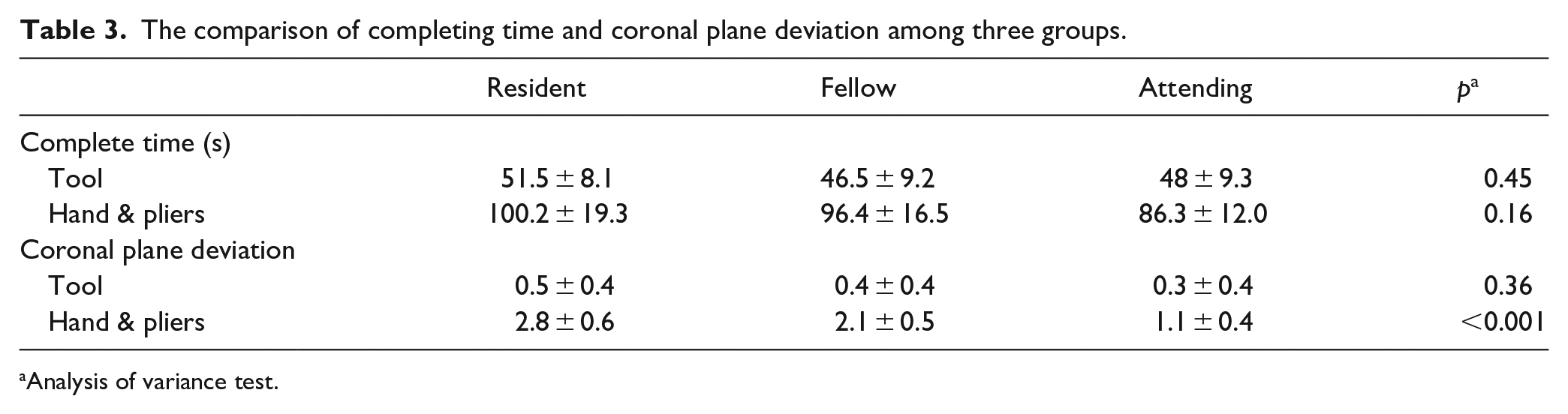
Analysis of variance test.
Discussion
To our knowledge, this is the first study to evaluate the feasibility and effectiveness of a newly designed tool for achieving the ESIN pre-bending principal role. Surgeons could quickly evaluate whether they had achieved the ESIN pre-bending principal role with the tool. With the help of the new tool, the time of ESIN pre-bending was significantly shorter and the coronal plane deviation of nails after pre-bending was significantly smaller than that of the conventional method in each surgeon groups of this research. The results showed that the new tool has the advantage of helping surgeons achieve the principal role with less coronal plane deviation of ESINs, especially for inexperienced residents who have yet to perform enough surgeries using ESINs to reach the performance equivalent to fellows and attending doctors.
The history of an intramedullary device dates back to the mid-19th century when ivory nails were used as intramedullary devices; 12 later, it was improved as Küntscher nail 13 and Rush nail. 14 However, such devices were used only for adults and were not suitable for children, as the physical injury was inevitable when using such devices. To avoid physes in growing children, ESIN was designed by surgeons from Nancy, France 15 in the 1980s and has been recommended as an acceptable implant for pediatric femur fractures by the American Academy of Orthopaedic Surgeons (AAOS). 16 Although ESIN was the preferred technique for femoral shaft fractures in a survey of members of the Pediatric Orthopaedic Society of North America (POSNA), 17 3-point fixation by two pre-bending ESINs is still the fundamental principle that must be strictly adhered to avoid complications and failures in the lower extremities.3 –11 However, no technique or tool was proposed to help surgeons achieve the “3-point support and fixation” principle. Most of the time, surgeons had to pre-bend the ESIN only with their hand, which might result in difficulty in achieving the principal role and significant coronal plane deviation in pre-bending ESIN, especially when the diameter of the ESINs is >3.0 mm. Significantly higher failure and complication rates are seen if the surgeon has little experience with the ESIN technique. 7
The literature has not discussed the coronal plane deviation during the ESIN pre-bending. Whether the coronal plane deviation will affect the biomechanical properties when a fracture is stabilized with ESINs is still being determined, because it is never mentioned in the literature.3 –5,7,8,10,11,18,19 The “3-point support and fixation” principle includes stability during the rotation of the biomechanics of the nail–bone unit.6,9 The coronal plane deviation may increase the difficulty of obtaining 3-point fixation when inserting the nails. If the coronal plane deviation is apparent, it could cause failure more frequently because of the instability of ESINs.3 –11,18,19 For all surgeons in each group, the coronal plane deviation of nails after pre-bending by the new tool was significantly smaller than that of the conventional method in this study.
Although it is a newly designed tool to achieve the principal role of ESINs, several areas for improvement, such as the limited number of participants and the lack of calculation of inter- and intra-observer variability. The separate introduction of the tool, detailed pre-bending information to participants, and the participants used the new tool in the first pre-bending round might lead to potential bias. There might be subjective bias for being a non-randomized study when the participants were grouped by their experience with the ESIN technique. The possibility that coronal plane deviation affects the stability of the nail–bone unit requires further research. A bending instrument with more hinging points might pre-bend the entire ESIN and obtain a long arch like a spring, but the part inserted into the bone was limited. However, the curve’s apex depends on the distance from the tip of the ESIN to the fracture area, and the distance between more hinging points cannot be adjusted in practice. Whether the advantages of the tool presented in the study might lead to better clinical results still need further clinical observation.
Conclusion
The newly designed tool for ESIN pre-bending was convenient and quick in achieving the principal role of the ESIN technique. Surgeons could reduce the coronal plane deviation when pre-bending ESINs, especially for surgeons with less experience with the ESIN technique.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231193713 – Supplemental material for A novel pre-bending tool for elastic stable intramedullary nailing: An efficient and accurate study
Supplemental material, sj-pdf-1-cho-10.1177_18632521231193713 for A novel pre-bending tool for elastic stable intramedullary nailing: An efficient and accurate study by Wen Shu, LongJun Yu, Theddy Slongo, Saroj Rai, Haobo Zhong and Xin Tang in Journal of Children’s Orthopaedics
Footnotes
Author contributions
LJ.Y. and W.S. were involved in data collection and follow-up assessments; X.T., S.R., and T.S. were responsible for the literature search and study design; W. S. and LJ.Y. drafted the manuscript. X.T. and HB.Z. finalized the manuscript.
Availability of data and materials
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
All guardians of patients signed written informed consent for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (IORG No: IORG0003571) gave a final APPROVAL on 20/11/2019 for the study. Although the data were collected anonymized and centrally, all guardians of patients signed written informed consent for participate.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.