
Abstract
Purpose:
A common question faced by clinicians is when a child may return to sport after treatment for a pediatric forearm fracture. There are few published recommendations and fewer supported by evidence. The aims of this study were to summarize existing published recommendation for return to sport after pediatric forearm fractures and to conduct a survey to determine usual clinical recommendations.
Methods:
A scoping review was performed on Ovid MEDLINE, Cochrane Central Register of Controlled Trials, Embase, Scopus, and Google Scholar in accordance with the Joanna Briggs Institute guidelines. In addition, 64 orthopedic surgeons were anonymously surveyed asking for recommendations regarding return to sport after pediatric forearm fractures. Participants were to assume children were 9 years old and played a sport with an average risk of forearm injury.
Results:
Twenty-two publications for return to sport were retrieved. Children with distal radius buckle fractures safely commonly returned to sport by 4 weeks after initial injury, while survey respondents recommended over 6 weeks. Survey respondents valued fracture stability the highest when making return to sport recommendations. Children with simple, metaphyseal, single-bone fractures were usually allowed to return to sport at 8–10 weeks post-injury. Diaphyseal and complete fractures were prescribed longer return to sport intervals. Australian respondents also prescribed longer return to sport intervals.
Conclusion:
Children with distal radius buckle fractures may return to sport by 4 weeks after initial injury, sooner than recommended. Published recommendations remain limited for other fractures. However, our survey suggests children with simple, metaphyseal, single-bone fractures may return to sport at 8–10 weeks. Children with diaphyseal and complete fractures should abstain from sport for longer than metaphyseal and greenstick fractures, respectively.
Level of evidence:
level V
Introduction
Forearm fractures are the most common injury in children, 1 accounting for 23%–40% of all injuries in children,2–4 and most commonly occur during sporting activities. 5 Over one-third of all preadolescent fractures are a result of sport. 6 In Australia, sport is encouraged, with 55.5% of school-aged children being involved in some form of regular, organized sport. 7 Return to sport (RTS) is the most common question posed by children, parents, and athletes. 8
Allowing RTS requires caution as the injury confers a fourfold risk of further injury 9 and refracture already complicates 1.4%–7% of all forearm fractures.10–12 In particular, a “premature” RTS has been reported (without strong evidence) to increase risk of malunion, non-union, and growth arrest. 13 Clinicians face perceived pressure from affected children, parents, or even coaches to minimize time away from sport. Recommendations for RTS after pediatric forearm fractures are scarce,6,14 with no standardized guidelines to aid the treating doctor to make a decision.6,14,15 This is evident in a study of distal radius buckle fractures, which demonstrated that only 46.9% of parents were given any recommendations for RTS and only 38.3% recommended an appropriate time interval. 16
Therefore, the aims of this study are to (1) summarize existing published recommendation for RTS after pediatric forearm fractures and to (2) to conduct a survey to report what recommendations are routinely given in practice.
Methods
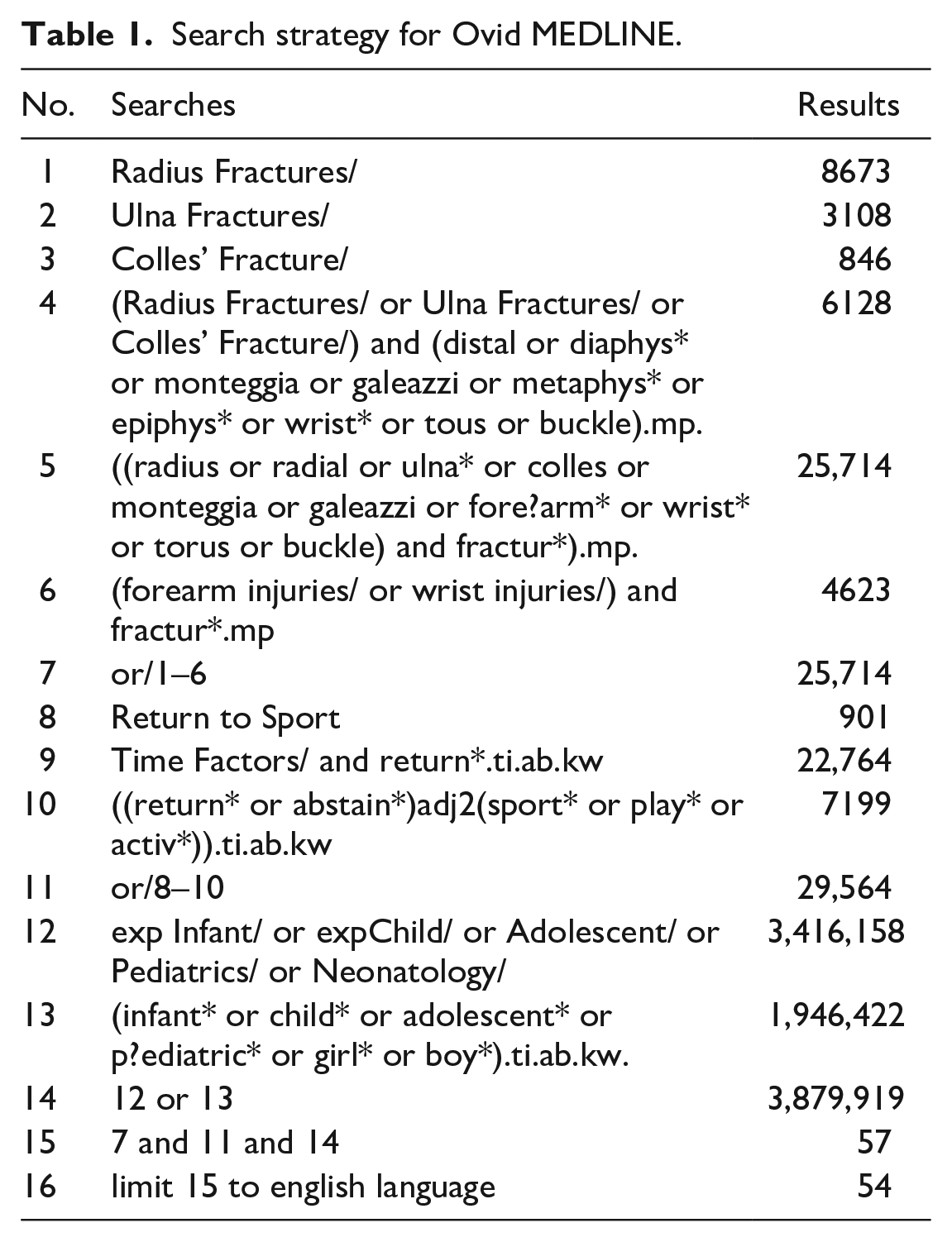
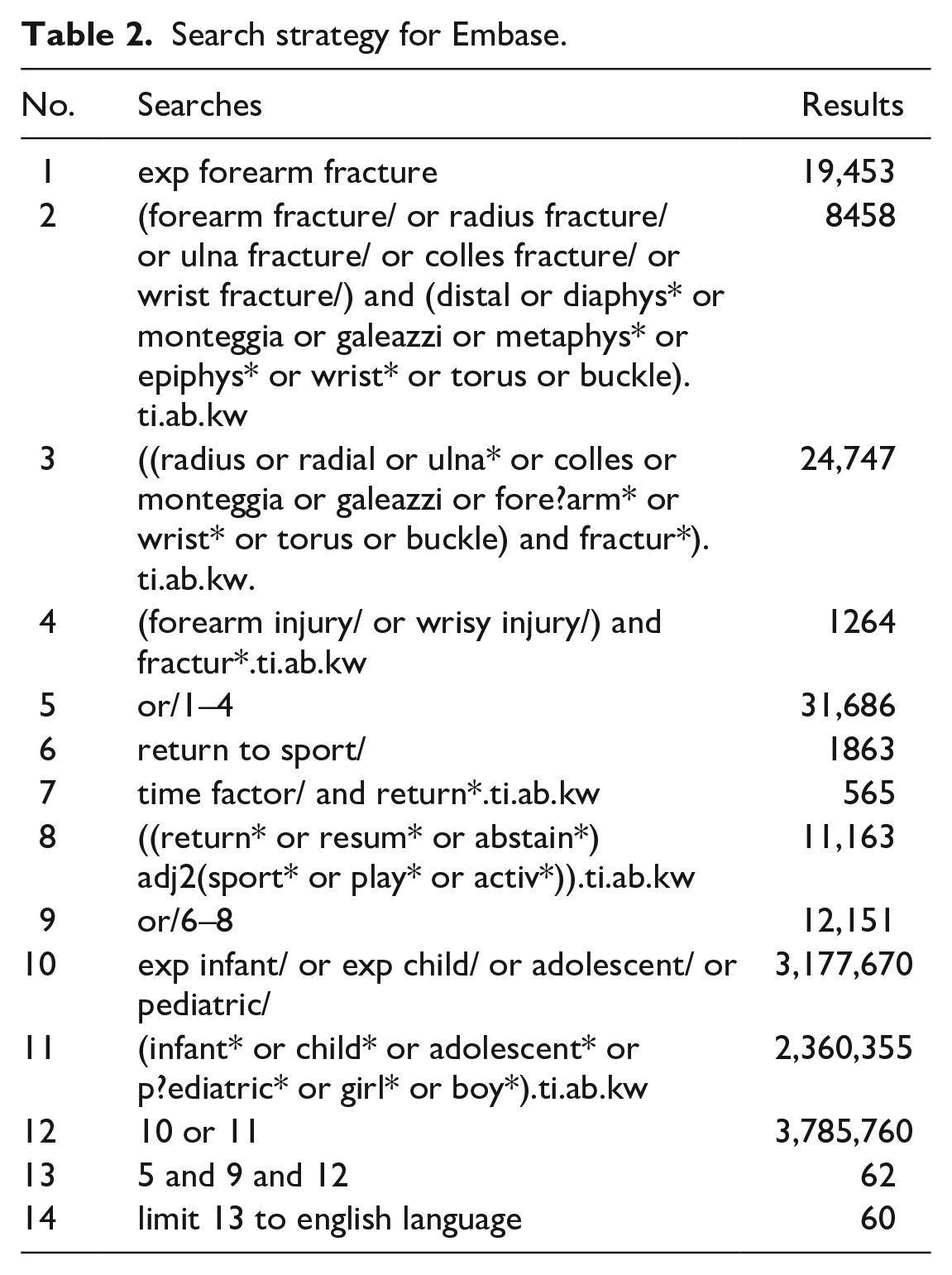
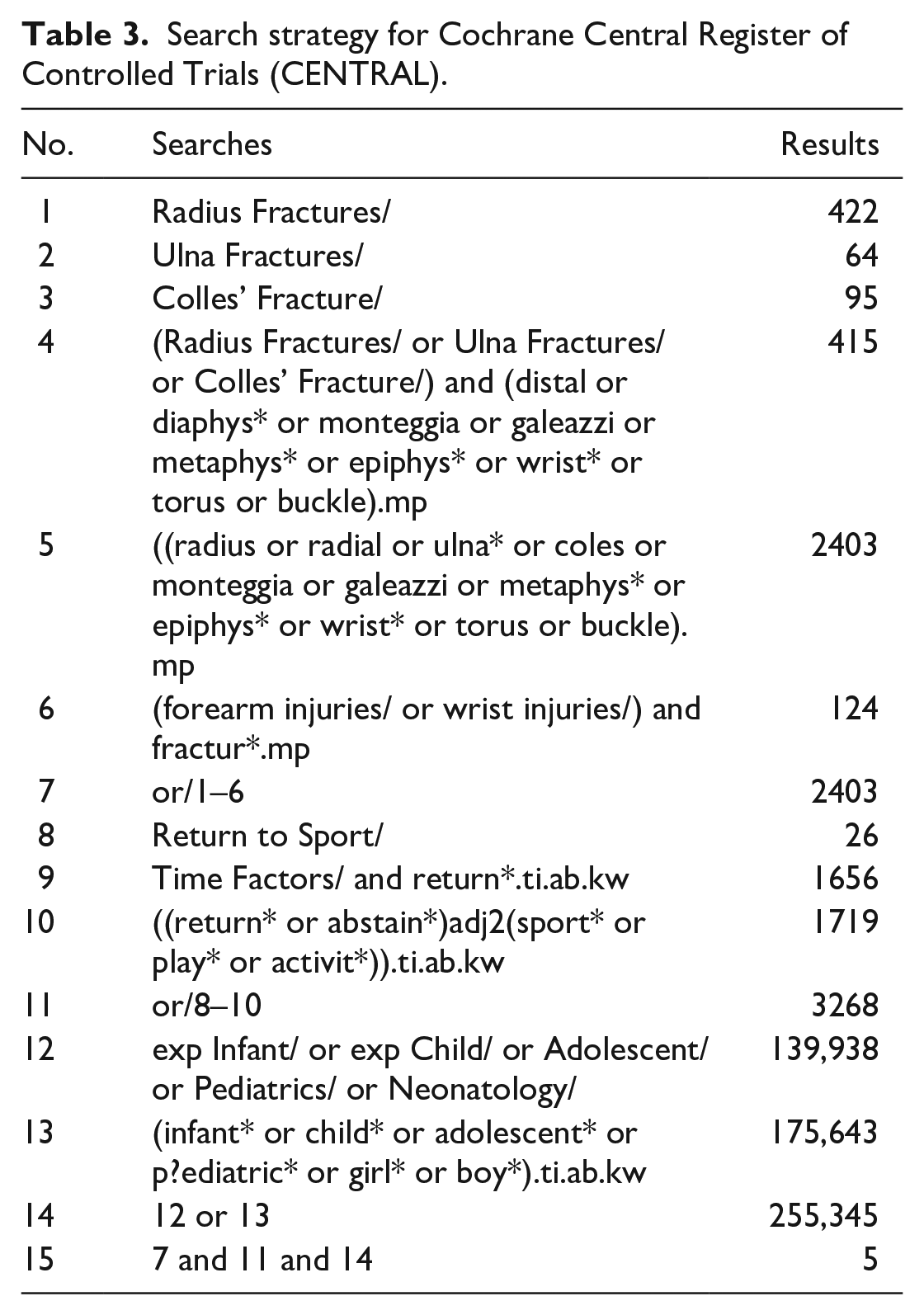
A thorough three-staged search was conducted as per the Joanna Briggs Institute (JBI) reviewer’s manual section on scoping reviews. 17 The search was designed to answer the question, “What are the recommendations for return to sport after forearm fractures in children?” A preliminary search was performed on Ovid MEDLINE and Cochrane Central Register of Controlled Trials to identify keywords and index terms. A secondary search was subsequently undertaken on Ovid MEDLINE, Cochrane Central Register of Controlled Trials (Cochrane), Embase, Scopus, and Google Scholar. Keywords and search strategies used are detailed in Online Appendix 1 and Tables 1–3. Finally, the references of all included publications were examined for relevant articles.
Search strategy for Ovid MEDLINE.
Search strategy for Embase.
Search strategy for Cochrane Central Register of Controlled Trials (CENTRAL).
Inclusion criteria were set to include publications of patients aged 2–18 years with traumatic fractures of either the radius or the ulna. Both undisplaced and displaced fractures, as well as those treated surgically and non-surgically, were included. Publications were included if they made RTS recommendations or if RTS intervals were recorded. Studies recording return to regular, full, or near-full activity in the target patient demographic were also included. Only studies of humans and those in English language were included. Gray literature, review articles, expert opinion, and all study types were included. Exclusion criteria were set to exclude stress fractures, avulsion fractures, overuse injuries, and pathological fractures.
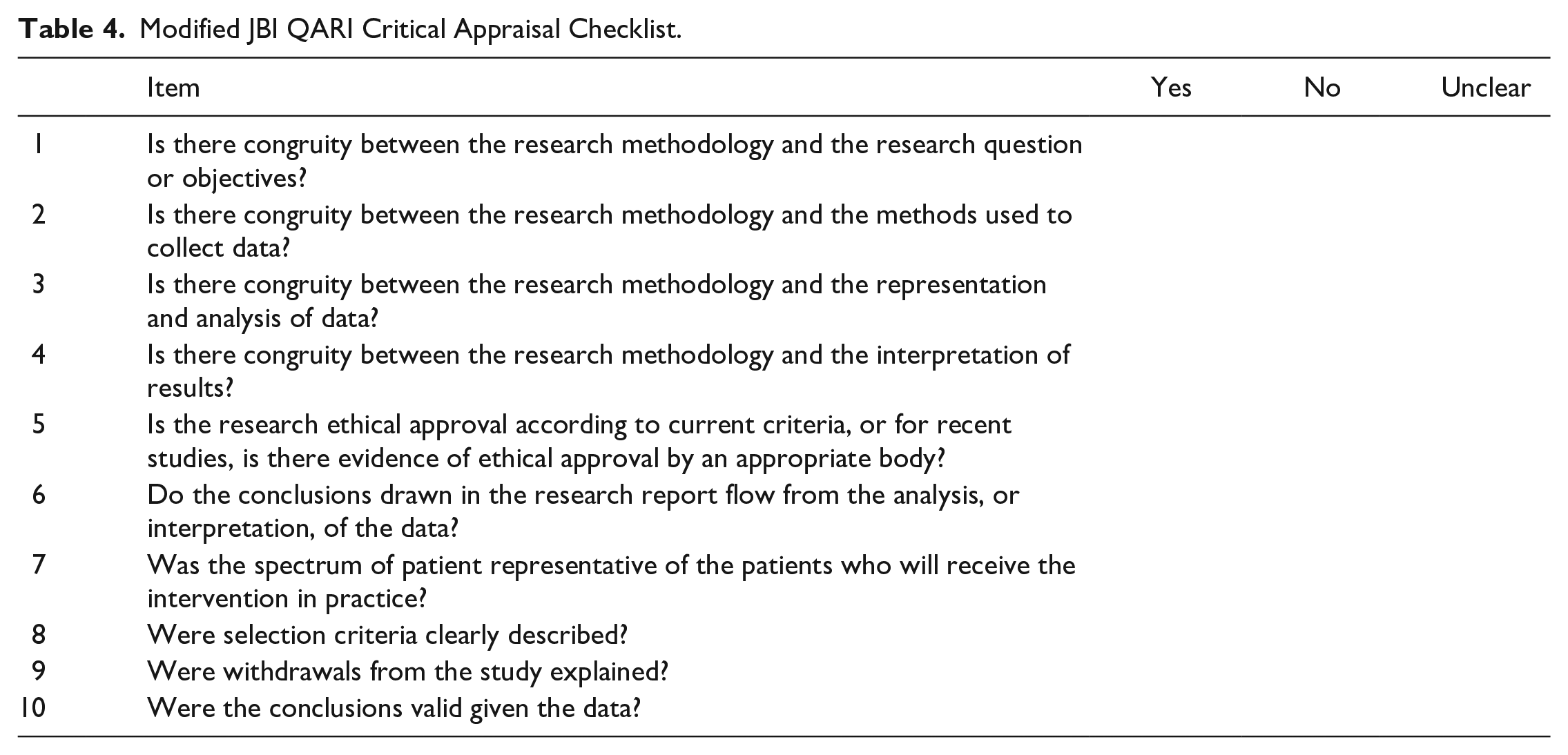
Articles retrieved from this search were reviewed for inclusion by two independent investigators (A.B. and R.B.). Articles were first reviewed by title and abstract, and then by full text. Articles included after this were then assessed for acceptable methodological quality using the Modified JBI QARI Critical Appraisal Checklist (Table 4). The same two investigators then extracted the data from the qualifying articles, and the data were recorded on a spreadsheet using the software Microsoft Excel (version Excel for 365; Microsoft Corporation, Redmond, WA, USA). The data were then synthesized in accordance with the JBI Reviewer’s Manual recommendations for scoping reviews. 17
Modified JBI QARI Critical Appraisal Checklist.
An anonymous 23-item survey was then distributed among experienced pediatric orthopedic surgeons (Online Appendix 2). Participants were recruited from the International Paediatric Orthopaedic Think Tank (IPOTT) and the Australian Paediatric Orthopaedic Society (APOS). Participants were recruited by direct e-mail, the Australian Orthopaedic Association (AOA) website, and the AOA newsletter. Participants were asked about their level of experience and broad location of practice. Participants were then asked to rate the extent that patient age, gender, fracture stability, treatment method, and level of sporting competition would affect their recommendations for RTS, on a scale from 0 to 10. Fracture stability was defined as the perceived susceptibility of a fracture to displace based on the fracture configuration. Finally, participants were shown preoperative radiographs of a variety of common forearm fractures and asked to make recommendations for time after initial injury, in weeks or months, before RTS could be allowed. All fractures were simple fractures as none were comminuted. Participants were to assume that the fracture would be treated by the method of their choice and that the child was involved in sport requiring a moderate level of upper body force and risk of falling. Participants were also told to assume the patients were all 9 years old to nullify the influence of age on their recommendations. This age was chosen to grossly represent the midpoint of ages considered pediatric. Ethical approval was obtained for the use of de-identified radiographs. All responses were recorded on the online platform SurveyHero.
Statistical analysis was performed using IBM SPSS Statistics (Windows version 26.0, IBM Corp., Armonk, NY, USA). Recommendations by different demographics of participants were compared using the Mann–Whitney U test. The Mann–Whitney U test was also performed to determine differences between recommendations by fracture type, fracture location, and initial degree of displacement.
Results
Scoping review
Twenty-two publications were included for data extraction (Figure 1). Sixteen studies6,8,16,18–30 related to specific fractures (Table 5), while six studies14,31–35 made general recommendations (Table 6).
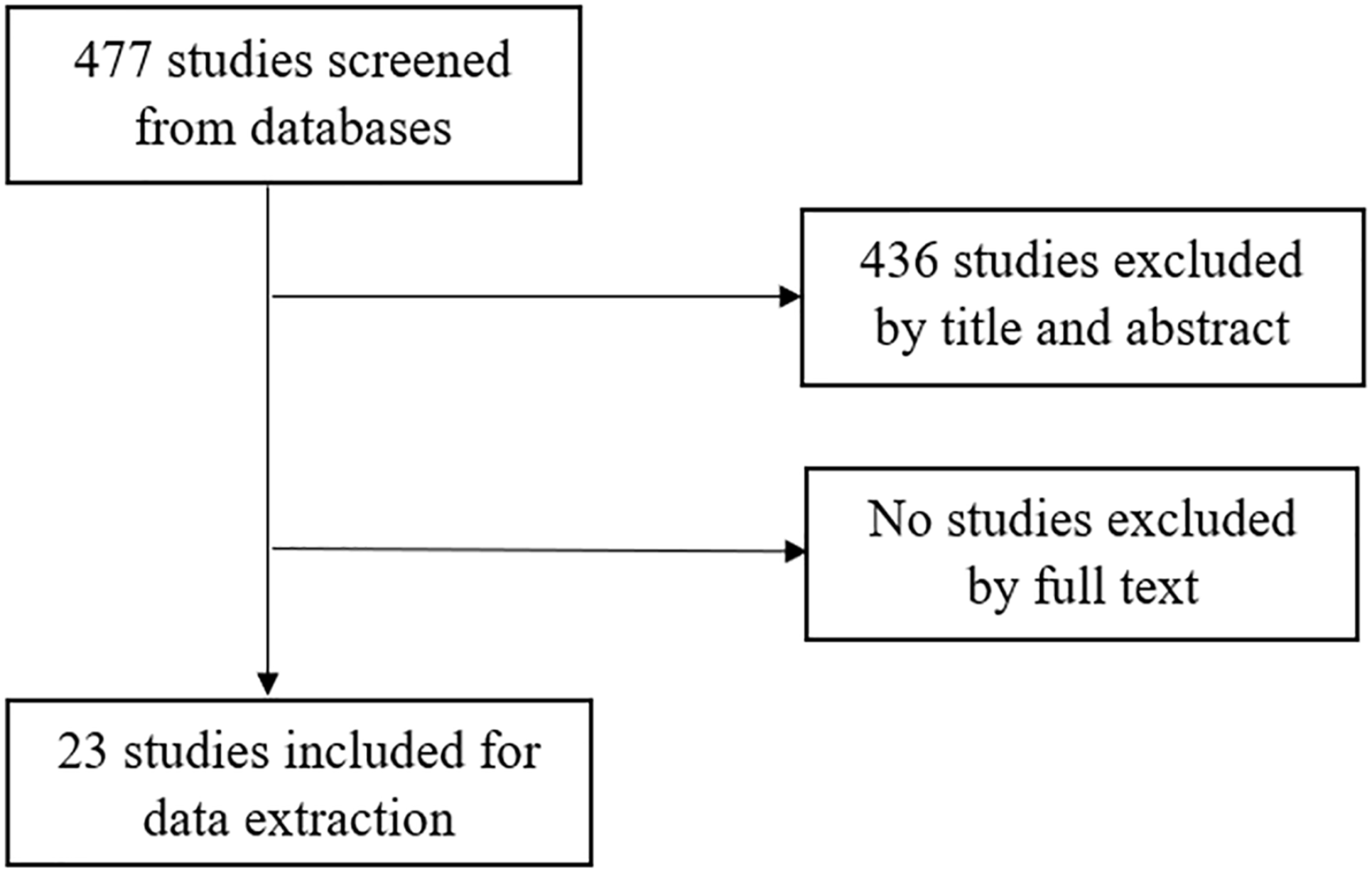
PRISMA-style flow diagram detailing inclusion and exclusion of studies in study screening.
List of published fracture-specific recommendations and recorded return to sport (RTS) intervals.
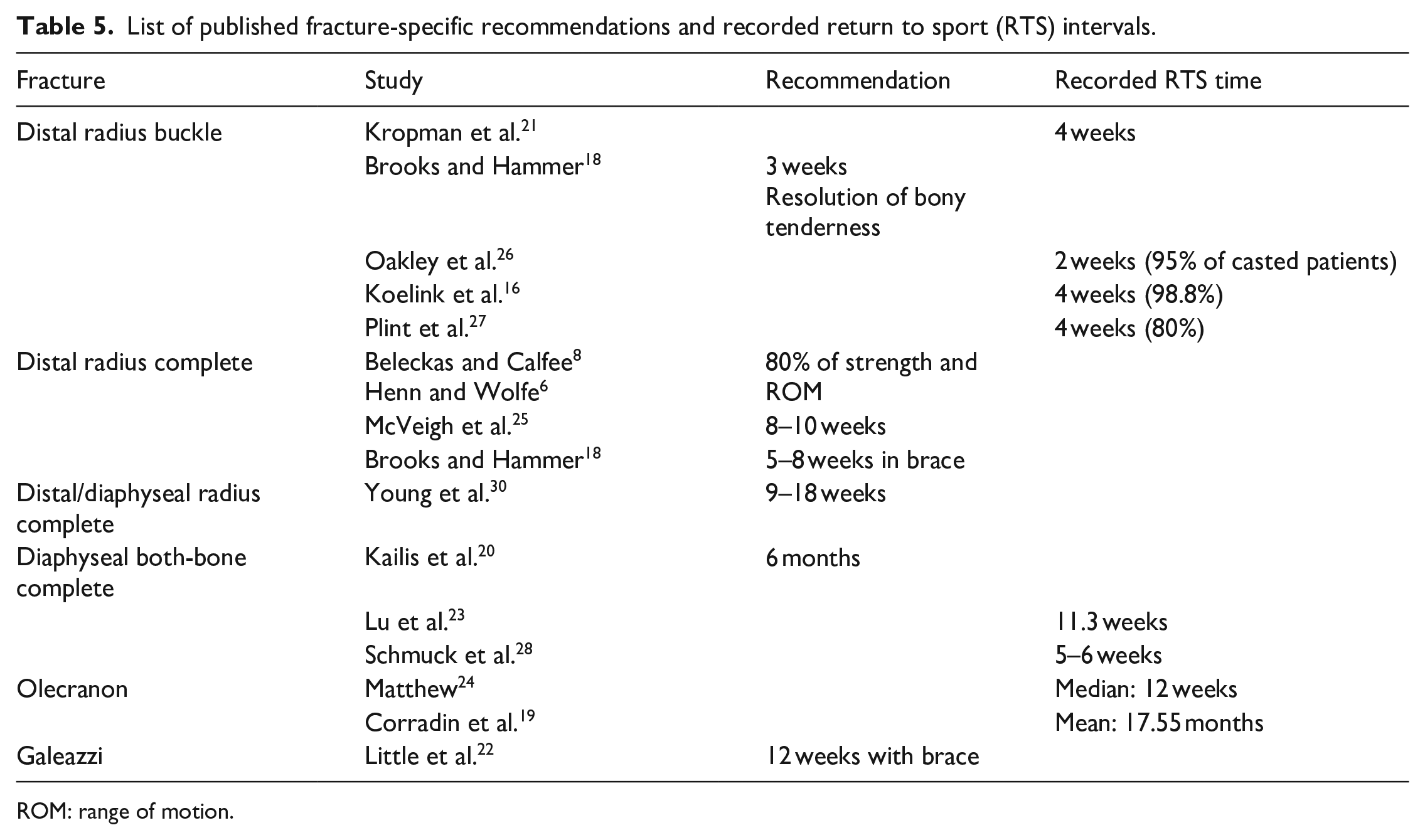
ROM: range of motion.
List of published general recommendations for return to sport (RTS).
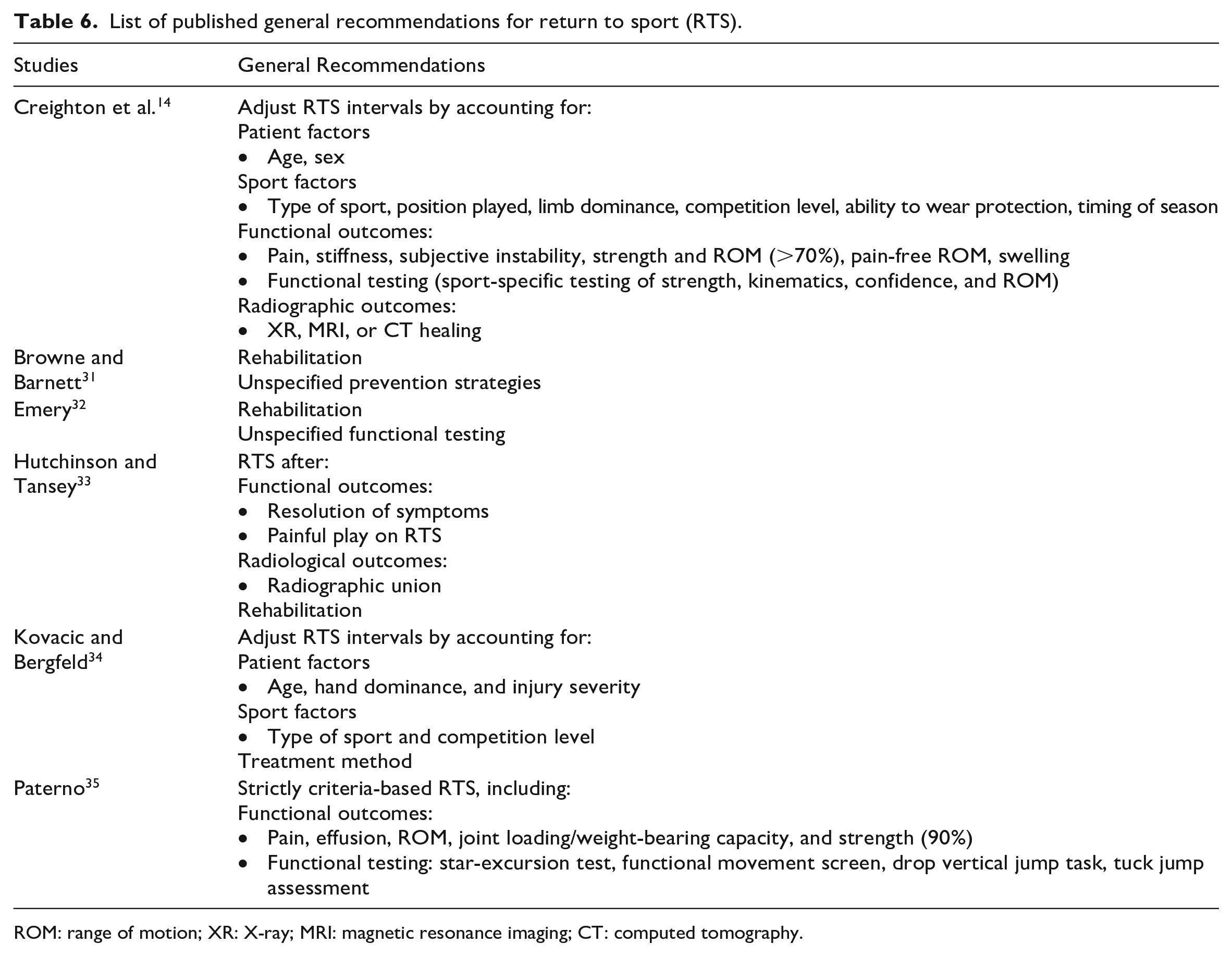
ROM: range of motion; XR: X-ray; MRI: magnetic resonance imaging; CT: computed tomography.
Distal radius buckle fractures
One article made recommendations for RTS after distal radius buckle fractures 18 and five recorded intervals at which their patients returned to normal activities or sport.16,21,26,27,29 Patients returned to sport by 4 weeks after their initial injury in most studies, and in one study 95% of patients returned to normal activities at 2 weeks after their initial injury. 26 Interestingly, there were no refractures recorded in any of these studies. One article recommended RTS at 3 weeks if there was no bony tenderness. 18 One study only recorded RTS as time after cast removal; however, the casting time was variable among patients, so RTS time from initial injury could not be calculated. 29
Distal radius complete metaphyseal fractures
Two articles made general recommendations for RTS after complete distal radius fractures,6,8 while two review articles recommended RTS at 5–8 weeks 18 and 8–10 weeks, respectively. 25 Another article recommended RTS 6–12 weeks after cast removal but did not discriminate between distal and diaphyseal fractures. 30 General recommendations included accounting for age, sex, fracture stability, fracture characteristics, and need for wrist in sport. Recommendations also included RTS after 80% of strength and range of motion (ROM) were achieved, gradual RTS, and RTS in a cast for athletes.
Diaphyseal both-bone fractures
Three studies recorded RTS intervals after diaphyseal both-bone fractures with no consensus.20,23,28 Recommendations ranged between 5 weeks and 6 months after initial injury. Interestingly, one study allowing RTS at 5–6 weeks after initial injury reported a refracture rate of 6.7%, 28 while studies allowing RTS at 11 weeks after initial injury or later presented refracture rate in 0.6% of cases.20,23
Olecranon fractures
Two studies19,24 reported different RTS intervals. Intervals ranged between 12 weeks and 17.6 months after initial injury.
Fracture-dislocations
One article recommended gradual RTS after Galeazzi and Monteggia fracture-dislocations at 12 weeks in a brace and full return at 6 months after initial injury. 22
General recommendations
Studies that made recommendations for RTS in general recommended prescription of RTS based on patient factors,14,34 sport-specific factors,14,34 functional outcomes,14,32,33,35 and radiological outcomes (Table 6). Rehabilitation prior to RTS was also recommended in three studies.31–33 Patient factors included age, sex, hand dominance, and injury severity. Sport-specific factors most commonly included type of sport and level of competition, although other factors were also suggested. Evaluation of functional outcomes prior to allowing RTS most frequently referred to resolution of symptoms; however, two articles recommended specific functional assessment.14,35 One recommended testing of sport-specific strength, kinematics, confidence, and ROM. 14 Numerous specific tests were listed in the other; 35 however, these were all lower limb injury assessment tools.36–39 Two articles recommended ensuring radiological healing prior to RTS.14,33
Survey
Sixty-four respondents completed the survey. The median age group of respondents was 50–60 years, and the median level of experience as a qualified surgeon was 10–20 years. Interestingly, the median level of pediatric orthopedic experience was longer than the median level of experience as a qualified surgeon at 21–29 years. This may be due to the inclusion of pediatric orthopedic experience during surgical training. Respondents consisted of 46 dedicated pediatric orthopedic surgeons. There were 44 Australian surgeons who were all members of the AOA recruited via direct e-mail and the AOA newsletter, and 20 members of the IPOTT recruited by direct e-mail. Fifty respondents predominantly practiced in metropolitan regions.
Fracture stability was deemed to be more relevant to RTS recommendation than any other factor (mean, 7.5 ± 2.4). All factors except gender were also scored highly as factors relevant to RTS recommendations (Table 7).
Summary of survey responses.
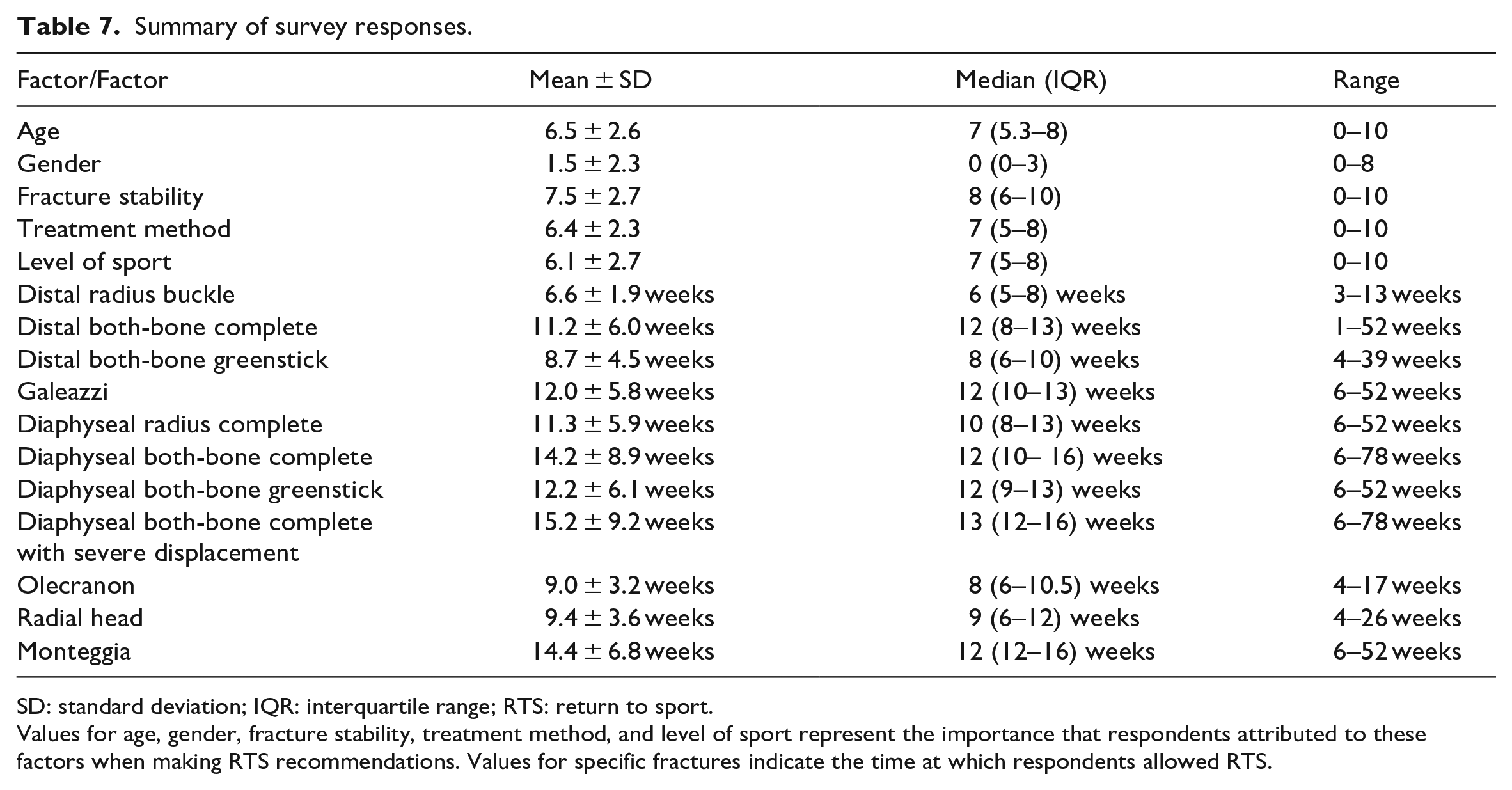
SD: standard deviation; IQR: interquartile range; RTS: return to sport.
Values for age, gender, fracture stability, treatment method, and level of sport represent the importance that respondents attributed to these factors when making RTS recommendations. Values for specific fractures indicate the time at which respondents allowed RTS.
Respondents prescribed the shortest intervals for RTS post-injury for distal radius buckle fractures (mean, 6.6 ± 1.9 weeks; range, 3–13 weeks), distal both-bone greenstick fractures (mean, 8.7 ± 4.5 weeks; range, 4–39 weeks), olecranon fractures (mean, 9.0 ± 3.2 weeks; range, 4–17 weeks), and radial head fractures (mean, 9.4 ± 3.6 weeks; range, 4–26 weeks). The longest RTS intervals were prescribed for complete diaphyseal both-bone fracture, with and without severe displacement (mean, 15.2 ± 9.2 weeks; range, 6–78 weeks and mean, 14.2 ± 8.9 weeks; range, 6–78 weeks) and Monteggia fracture-dislocations (mean, 14.4 ± 6.8 weeks; range, 6–52 weeks). Recommendations for the remaining fractures are listed in Table 7.
The only significant difference in recommendations between pediatric orthopedic surgeons and general orthopedic surgeons was in recommendations for complete diaphyseal both-bone (p = 0.017; mean, 14.0 ± 10.5 vs 14.6 ± 2.9 weeks) and radial head fractures (p = 0.005; mean, 9.0 ± 3.3 vs 9.3 ± 3.8 weeks). There were also no significant differences in recommendations made by pediatric trauma surgeons and the remaining cohort.
Australian respondents prescribed longer RTS intervals than International respondents for distal radius buckle fracture (p = 0.02; mean, 6.8 ± 1.8 vs mean 5.9 ± 2.2 weeks), distal both-bone greenstick fracture (p = 0.007; mean, 9.4 ± 5.1 vs 7.2 ± 2.5 weeks), complete diaphyseal radius fracture (p = 0.026; mean, 11.9 ± 6.5 vs 10.0 ± 4.0 weeks), and olecranon fracture (p = 0.0012; mean, 9.6 ± 3.2 vs 7.7 ± 3.2 weeks). There were no significant differences between recommendations made by metropolitan and rural respondents.
Diaphyseal fractures were prescribed significantly longer RTS intervals when analyzing distal versus diaphyseal complete both-bone fractures (p < 0.001; mean, 11.2 ± 6.0 vs 14.2 ± 8.9 weeks) and both-bone greenstick fractures (p < 0.001; mean, 8.7 ± 4.5 vs 12.2 ± 6.1 weeks). Similarly, complete fractures were prescribed significantly longer RTS intervals when analyzing complete versus greenstick distal (p < 0.001; mean, 11.2 ± 6.0 vs 8.7 ± 4.5 weeks) and diaphyseal fractures (p = 0.01; mean, 14.2 ± 8.9 vs 12.2 ± 6.1 weeks). There were no significant differences between recommendations for fractures with varying degrees of initial displacement.
Discussion
Making recommendations for RTS after forearm fractures in children remains challenging as there has not yet been a summary of published recommendations. There is a lack of clinical guidelines that may otherwise direct a clinician. This study has allowed for a summary of published recommendations and contemporary recommendations from experienced pediatric orthopedic surgeons.
This study has demonstrated no refractures in distal radius buckle fractures who have been allowed to RTS at 4 weeks after initial injury, with two randomized controlled trials and one randomized prospective study demonstrating no refractures after allowing RTS between 2 and 4 weeks from initial injury.21,26,27 In contrast, survey respondents only allowed RTS at an average of 6.6 weeks for these fractures. In the published literature, recorded RTS intervals and fracture-specific recommendations for other fracture types lacked consistency and had minimal supporting evidence, precluding to deduction of meaningful conclusions. For this reason, the results of our survey are important and provide the greatest set of recommendations currently available.
Published recommendations did advocate for assessment of functional outcomes and rehabilitation rather than purely radiological healing before RTS. Although there is much contention regarding the best measurement of healing,40–42 assessment of functional outcomes has become popular in the last decade.
Several studies have recommended the use of both functional and radiographic outcomes in the definition of union.40,42,43 These authors seem to favor functional recovery as the goal of treatment and track this as an end-point. Furthermore, radiographic outcomes have been shown to correlate poorly with strength and stiffness of the healing bone and lag behind changes in mechanical properties of the bone.42,44 There are several definitions of radiographic union, 43 including the Radial Union Scoring System (RUSS); 45 however, the determination of union may not accurately predict uncomplicated healing. Combining the use of functional and clinical outcomes before allowing RTS may be preferable. The use of validated outcome measures such as the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH),19,46 Visual Analog Score for pain, 21 Activities Scale for Kids score,25,27 and RUSS is also encouraged. Suggestions for sport-specific functional testing and gradual RTS may be beneficial, as these will account for sport-related factors including type of sport, position played, and the need for upper limb in the sport. Assessment of patient factors including age, fracture stability, and hand dominance may also help to inform RTS recommendations; however, gender appears unlikely to help. Our recent systematic review demonstrated no correlation between refracture risk after pediatric forearm fractures and gender, 47 and this is likely to be true regarding other complications. Survey responses are also consistent with these suggestions regarding age, fracture stability, and gender.
Given the paucity of evidence-based recommendations for fractures other than distal radius buckle fractures, the results of our survey provide the greatest body of recommendations. Although there was considerable variation in survey responses for many fractures, the mean and median values represent the most popular recommendations, providing insight into an otherwise uncertain field. It should be noted that these recommendations were for 9-year-old children, and adjustment for age should be made when consistent evidence emerges about the effect of age on RTS-related complication risk. These recommendations were from surgeons with a median of 21–29 years of orthopedic experience, meaning that they can be considered expert opinion. From these results, we can see that single-bone metaphyseal fractures and metaphyseal greenstick fractures are usually allowed to RTS between 8 and 10 weeks. Meanwhile, children with diaphyseal both-bone fractures and fracture-dislocations were allowed to RTS between 12 and 14 weeks post-injury. In this study, surgeons prescribed significantly longer RTS intervals to diaphyseal fractures, and this partially explains these findings. There is good evidence to suggest diaphyseal fractures are at greater risk of refracture,10,47,48 and so these recommendations are likely to be beneficial. Complete fractures were also prescribed significantly longer RTS intervals when compared to greenstick fractures. Complete fractures require more bone formation and are perhaps prescribed longer RTS time due to this.
Differences in recommendations from pediatric and general orthopedic surgeons were few and negligible, as were those from metropolitan and rural locations and those from pediatric trauma surgeons and the remaining cohort. The similarities between these groups are likely to be due to the common orthopedic training program that these surgeons undergo. Meanwhile, Australian surgeons commonly prescribed longer RTS intervals than International surgeons. The lack of a shared training program may also account for disparities in recommendations between Australian and International surgeons. Australian surgeons may prescribe longer RTS intervals due to a greater prevalence of higher physical contact sports in the Australian environment and wheeled-vehicle-related sports (such as motorcycles). In fact, 33% of Australian children who play sport are involved in high physical contact or wheeled sports. 49
This study was limited by the paucity of published recommendations for RTS after pediatric forearm fractures. Furthermore, aside from distal radius buckle fractures, there was a lack of consistency in recorded RTS intervals, making definitive conclusions regarding RTS in these fractures difficult. The lack of evidence-based recommendations is likely to account for these issues. Furthermore, pediatric, Australian, and metropolitan respondents were overrepresented in our survey; however, they do reflect a high level of experience in the field.
Conclusion
Children with distal radius buckle fractures may RTS at 4 weeks after initial injury, which is sooner than commonly allowed in practice. RTS requires a holistic assessment of patient factors, and functional and radiological recovery. Simple, single-bone, metaphyseal fractures are usually allowed to RTS between 8–10 weeks post-injury. Diaphyseal and complete fractures should be prescribed longer RTS. Australian surgeons recommend RTS later than surgeons overseas.
Supplemental Material
sj-docx-1-cho-10.1177_18632521231156434 – Supplemental material for Return to sport after forearm fractures in children: A scoping review and survey
Supplemental material, sj-docx-1-cho-10.1177_18632521231156434 for Return to sport after forearm fractures in children: A scoping review and survey by Ameya Bhanushali, Rebecca Bright, Louis Xu, Peter Cundy and Nicole Williams in Journal of Children's Orthopaedics
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was completed in accordance with the principles of the Helsinki Declaration. Ethical approval was obtained from the Women’s and Children’s Hospital Network Ethical Committee on 2 October 2020 for the use of de-identified radiographs utilized in the survey (HREC/19/WCHN/109). Informed consent was not required for this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.