
Abstract
Abstract
Purpose
The purpose of this study was to determine the risk factors for loss of reduction in patients with an isolated distal radius fracture and intact ulna.
Methods
Outpatient records and initial, post-reduction, and follow-up radiographs of children with displaced distal radial metaphyseal fractures and intact ulnas that required closed reduction and casting at our institution were reviewed for demographic factors, body mass index (BMI), initial fracture displacement, residual displacement after reduction, and 3-point cast index. Loss of reduction was defined as angulation ≥15° in the coronal plane for all ages and/or angulation ≥20° in the sagittal plane for patients ≥11 years of age and ≥30° for children <11 years of age. Additionally, all patients who were remanipulated and/or pinned were considered to have lost reduction.
Results
Thirty-five of the 76 patients in our series met the criteria for loss of reduction (46%). Multivariate logistic regression revealed that initial angulation in the coronal plane and post-reduction translation in the coronal plane were independent predictors for loss of reduction. Patients with >11° of initial angulation in the coronal plane were 6.3 times as likely to lose reduction (confidence interval [CI]: 1.43–28.3, P = 0.015) and those with any amount of residual translation in the coronal plane after closed reduction were 7.8 times as likely to lose reduction (CI: 2.5–24.0, P < 0.001).
Conclusion
Our study, the largest dedicated series of distal radial metaphyseal fractures with intact ulnas, indicates that loss of reduction is common, and that risk factors include initial angulation in the coronal plane and post-reduction translation in the coronal plane.
Introduction
Distal radial metaphyseal fractures are among the most common fractures seen in children [1, 2]. It has been reported that between 35 and 45% of all pediatric fractures involve the radius, with over three-quarters of these involving the distal radius [3–6]. Closed reduction and cast immobilization continues to be the mainstay of treatment for most displaced distal radius fractures, in part, because of the remodeling potential of the pediatric wrist [1, 7, 8]. However, several authors have advocated percutaneous pin fixation for those fractures that are at high risk for loss of reduction [7, 9, 10].
One particular injury pattern that has been associated with difficulty in maintaining reduction is a distal radial metaphyseal fracture in the setting of an intact ulna [10, 11]. Similar to Gibbons et al. and Roy, we have found this fracture pattern to be particularly problematic in our practice, with a high incidence of lost reduction and remanipulation. While the risk factors for loss of reduction have been examined across all distal radial fractures [8, 12, 13], the risk factors for loss of alignment within this particular fracture pattern have yet to be described. The purpose of this study was to determine the risk factors for loss of reduction in patients with an isolated distal radial metaphyseal fracture and intact ulna.
Methods
After obtaining IRB approval, we queried the outpatient database at our pediatric trauma center to identify those patients with an ICD-9 code consistent with a distal radius fracture. For each of these patients, initial radiographs were screened in order to identify those patients with a distal radial metaphyseal fracture and an intact ulna. For the purposes of this study, ulnar styloid fractures and buckle fractures were considered to be intact. We further included only those patients who had a closed reduction performed at our emergency department. As this was a retrospective study, there were no strict criteria used to determine which fractures required reduction; however, all fractures were displaced. All reductions were performed under conscious sedation by orthopaedic housestaff. Conscious sedation consisted of either ketamine or fentanyl and midazolam, and was administered by the emergency department. Reductions were performed using a mini “C arm” to verify the fracture position and the quality of the reduction. All patients were immobilized in a long-arm fiberglass cast after reduction.
For those patients who met the initial inclusion criteria, emergency department and outpatient records were retrospectively reviewed to determine demographic information and body mass index (BMI). All radiographic measures were performed by three of the five authors (N.A.B., J.A.B., J.A.P.) using PACS software and digital images. Injury radiographs were measured for initial shortening, and angulation and translation in both the coronal and sagittal plane. Translation was expressed as a percentage by dividing the distance of translation by the width of the bone at the level of the fracture. Similarly, shortening was calculated by dividing the length shortened by the diameter of the radius at the level of the fracture site. Angulation in both the coronal and sagittal planes were measured by first finding the bisecting line of each fragment (i.e., a line drawn along the midshaft of the diaphysis, as well as a second line along the midshaft of the metaphysis/epiphysis). Angulation in a given plane was defined as the angle between these two lines. Immediate post-reduction radiographs were used to determine residual shortening, angulation, and translation (both coronal and sagittal), as well as the 3-point cast index [12, 14]. Each of these variables was considered to be a potential risk factor for loss of fracture reduction. The minimum follow-up necessary for inclusion in the study was set at 6 weeks.
Follow-up radiographs from each visit were assessed for shortening, angulation, and translation. Loss of reduction was defined as angulation ≥15° in the coronal plane for all ages and/or angulation ≥20° in the sagittal plane for patients 11 years of age or older and ≥30° for children 10 years of age or younger. Additionally, all patients who were re-manipulated or closed reduced and percutaneously pinned were considered to have lost reduction. Risk factors were compared between the group that maintained reduction and the group that lost reduction at a univariate level using Mann–Whitney U tests. For those factors with univariate significance, multivariate logistic regression was performed to determine independent predictors for loss of reduction (SPSS version 16.0, SPSS Inc., Chicago, IL). Statistical significance was set at an alpha level of P = 0.05.
Results
Between January 2006 and June 2010, we identified 2,694 potential patients based on ICD-9 codes. Two hundred and seventeen patients had their closed reductions performed at our center. Of these, 93 met the initial criteria of a distal radius fracture and an intact ulna. Five patients were excluded for missing radiographs, one patient never received an adequate initial reduction (i.e., was never reduced below the criteria for loss of reduction), and 16 patients had less than 6 weeks follow-up. This left 76 patients as our study population (50 boys and 26 girls). Fourteen of the 76 patients had buckle fractures of the ulna, and 10 of 76 patients had ulnar styloid fractures. The average age of the patients in our series was 11.0 years (range 4.7–16.7 years). All patients were followed until fracture healing, with a mean follow-up of 11.5 weeks (range 6–38 weeks).
During the treatment period, 35 of 76 patients met the criteria for loss of fracture reduction (46%). Age, BMI, initial shortening, and initial angulation in the sagittal plane were not significantly different between those who did and did not lose reduction (Table 1). There was also no significant difference in the number of ulnar buckle fractures or styloid fractures between the two groups. Similarly, there was no significant difference between the two groups in terms of post-reduction angulation in the sagittal plane, post-reduction shortening, and the 3-point cast index. All fractures were reduced to angulations well below our definition of loss of reduction. Based on univariate statistical analysis, initial shortening, initial translation in the sagittal plane, initial translation in the coronal plane, initial angulation in the coronal plane, post-reduction translation in the sagittal plane, post-reduction translation in the coronal plane, and post-reduction angulation in the coronal plane were all significantly different between the two cohorts.
Risk factors for loss of reduction
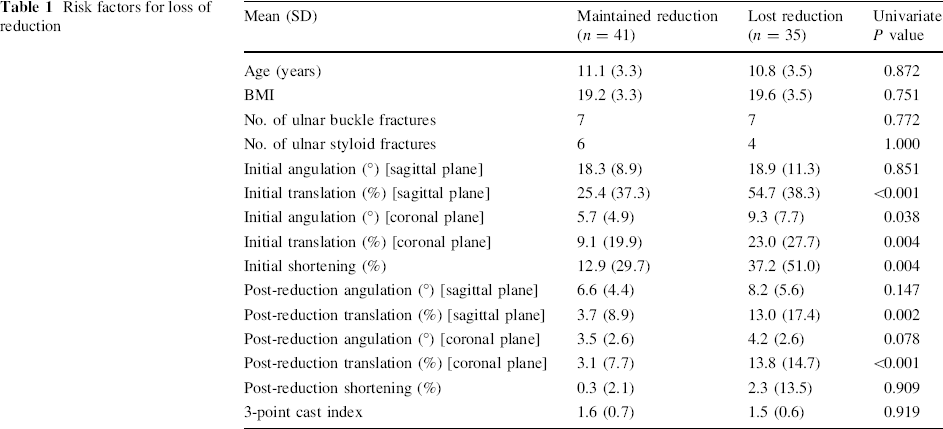
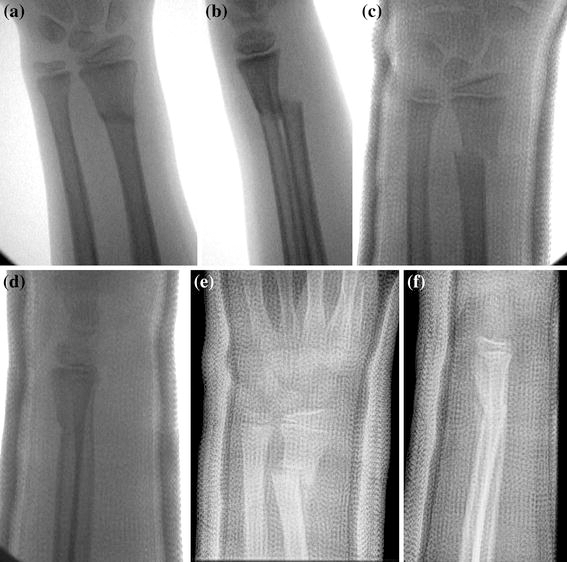
Multivariate logistic regression revealed that initial angulation in the coronal plane (5.7° vs. 9.3°, P = 0.033) and post-reduction translation in the coronal plane (3% vs. 14%, P < 0.001) were both independent predictors for loss of reduction. Patients with >11° of initial angulation in the coronal plane were 6.3 times as likely to lose reduction (confidence interval [CI]: 1.43–28.3, P = 0.015) and those with any amount of residual translation in the coronal plane after closed reduction were 7.8 times as likely to lose reduction (CI: 2.5–24.0, P < 0.001) (Figs. 1, 2).

Of the 35 patients who lost fracture reduction, two were re-manipulated without pinning, seven underwent repeat closed reduction with percutaneous pinning, and two had an open reduction and internal fixation. In 24 patients, the deformity was accepted with hopes that the fracture would remodel with time.
Discussion
Several authors have described the difficulty in treating the isolated displaced distal radius fracture with an intact ulna. Gibbons et al. [10] found that 10 of 11 such patients (91%) treated by closed reduction and casting alone required further manipulation compared to 0 of 12 patients who were closed reduced and percutaneously pinned. Those authors concluded that percutaneous pinning should be considered for all displaced distal radius fractures with an intact ulna, given the inherent instability of the fracture pattern. Roy [11] reported that 5 of 8 patients (63%) with completely displaced distal radius fractures with intact ulnas required remanipulation for loss of reduction. He noted the difficulty both in obtaining initial reduction and in maintaining that reduction with closed treatment. Other authors, however, have not found the presence of an intact ulna to be a significant risk factor for fracture instability [9, 13].
Our experience has been similar to Gibbons et al. and Roy: we have found the pattern of an isolated displaced distal radius fracture with an intact ulna to be particularly problematic in our practice. Like many busy pediatric trauma centers, we usually encounter these patients in an outpatient setting a week or so following initial closed reduction and casting under conscious sedation in our emergency department. At that time, a determination must be made as to which fractures would be best treated by early re-manipulation and pinning, and which ones will be successful with continued immobilization. Early identification of those fractures that are at a higher risk for loss of reduction could expedite surgical decision-making and minimize the need for late re-manipulation when the ability to restore anatomic alignment can be limited. As a result, we undertook this study in an effort to determine the specific risk factors for loss of reduction in patients with an isolated distal radial metaphyseal fracture and intact ulna.
Our results, like those of Gibbons et al. and Roy, suggest that loss of reduction in this fracture pattern is common (46%). In our study, the most important risk factors for loss of reduction of a distal radius fracture with an intact ulna were initial angulation in the coronal plane and post-reduction translation in the coronal plane. It is interesting to note that the 3-point cast index did not prove to be a significant factor on even the univariate analysis. It is generally well accepted that the quality of cast molding is an important factor in the risk of re-displacement following closed reduction of distal radius fractures in general [12, 14–16]. Specifically, the 3-point cast index has been shown to be superior to other cast measures in terms of sensitivity, specificity, positive predictive value, and negative predictive value [12]. Our study, however, did not prove the 3-point index to be a significant factor related to loss of reduction. Several previous studies have also established the importance of complete initial displacement in predicting the risk of redisplacement among all distal radius fractures, as this likely correlates with the amount of energy absorbed during the fracture and the degree of periosteal stripping [8, 12, 13, 17]. Mani et al. and Monga et al. highlighted the importance of initial translation rather than angulation in predicting later loss of reduction [13, 17]. Our study seems to suggest the opposite, that initial angulation (in the coronal plane) rather than initial translation is more predictive of loss of reduction. Similar to our study, those authors found that residual translation after closed reduction was another very important risk factor for loss of reduction.
In the present study, we used what we believed to be “real-world” criteria for defining loss of reduction as compared to some reports in the literature that use, perhaps, an overly strict definition of malalignment. In reality, there seems to be no true consensus on what constitutes unacceptable reduction of a distal radius fracture. The criterion used to define malreduction varies in the literature from 10 to 30° of sagittal plane angulation and 5–20° of coronal plane angulation, depending on the patient age and the specific series [7, 9, 12, 13, 17, 18]. Part of this ambiguity stems from a lack of consensus about the remodeling potential of the distal radius. Friberg reported that fractures with over 20° of dorsal angulation may not remodel completely, but Hughston demonstrated that, in children under 10 years of age, the distal radius can remodel up to 30–40° of angulation in the sagittal plane [8, 19–22].
For the purposes of this study, we considered both ulnar styloid fractures and buckle fractures to be intact and, therefore, included them in the series. Our rationale was that, in these cases, the ulnar “strut” remains in continuity; therefore, the effect on the adjacent fractured radius would be equivalent to a situation in which the ulna was not fractured at all.
A limitation of this retrospective study is the lack of sufficient follow-up to evaluate the degree of fracture site remodeling in those patients whose loss of reduction was accepted without re-manipulation. In addition, we do not have outcome data on these patients in order to determine whether or not the loss of reduction caused any functional deficits. However, it should be noted that this study makes no attempt to establish acceptable reduction parameters for isolated distal radius fractures; rather, we have relied on existing standards in the literature to determine what constitutes inadequate alignment.
Regardless of its limitations, this study, the largest dedicated series of distal radial metaphyseal fractures with intact ulnas, indicates that loss of reduction is common, and important risk factors include initial angulation in the coronal plane (especially in excess of 11°) and any amount of post-reduction translation in the coronal plane.