
Abstract
Abstract
Purpose
Unstable paediatric diaphyseal both-bone forearm fractures requiring fixation have traditionally been treated with rigid internal fixation with plate and screws. Intramedullary stabilisation has grown in popularity over the last 25 years but may be associated with rotational deformity and subsequent loss of pronosupination. This systematic review aims to establish which treatment method provides better functional outcome.
Methods
A systematic review of the published literature was performed, searching Medline, Embase, Pubmed and the Cochrane Library for English-language studies comparing intramedullary nailing with plate and screws in patients less than 18 years old with both-bone diaphyseal forearm fractures.
Results
Seven studies met the inclusion criteria. They were all retrospective comparative studies (level III or IV). One was age- and sex-matched. Three looked specifically at older children. No study reported a significant difference in functional outcome with either treatment.
Conclusions
The currently available literature shows no difference in functional outcome between intramedullary nailing and plate and screw fixation, even in older children with less remodelling potential. Intramedullary nailing may therefore be the treatment of choice for simple fracture patterns due to shorter operative time, better cosmesis and ease of removal. Plating may still have a role in more complex injuries.
Introduction
Diaphyseal forearm fractures comprise 3–6% of all paediatric fractures [1–3] and are the second most common fracture type among adolescents [4]. While 85% can be successfully treated with closed reduction and casting [5], some children can be left with a loss of forearm rotation after conservative management [6, 7]. Internal fixation may be indicated if conservative treatment fails to maintain alignment, in children nearing skeletal maturity, and in open fractures [8, 9]. Diaphyseal forearm fractures are known to remodel poorly, with a high incidence of mal-union [10]. Residual angulation or rotational deformity can lead to a significant reduction in pronosupination [11], particularly in older children in whom there is less potential for bone remodelling. Anatomical reduction may therefore be of greater importance in this age group as they can tolerate a lesser degree of mal-union. It is thought that restoration of the position and magnitude of the radial bow is the most important factor in preserving forearm range of motion [12].
In recent years the proportion of paediatric forearm fractures treated with internal fixation has increased [13], with a particular rise in the use of intramedullary nailing (IMN) [14]. This increase may be driven by improved understanding of the functional implications of mal-union, technological advances, societal expectations or fear of litigation.
Traditionally, internal fixation of unstable paediatric forearm fractures has been achieved by open reduction and rigid internal fixation with plate and screws (ORIF) with good results [7, 9], especially in terms of restoration of anatomy. IMN with Kirschner wires or elastic stable intramedullary nails has become popular due to improved cosmesis, shorter operative time, less soft tissue dissection and ease of removal, with good results reported [15–17]. Although anatomical reduction may be harder to achieve, the internal splint maintains alignment and length, whilst allowing micro-movement at the fracture site to occur, encouraging callus formation and potentially speeding union [18]. Significant complications have been reported, including pin site infection, osteomyelitis, synostosis and loss of reduction [19].
Due to the potential benefits and drawbacks of each surgical intervention, this systematic review of the literature aims to establish if internal fixation with plate and screws or an intramedullary device leads to better functional outcome when diaphyseal fractures of the radius and ulna in children are treated surgically.
Methodology
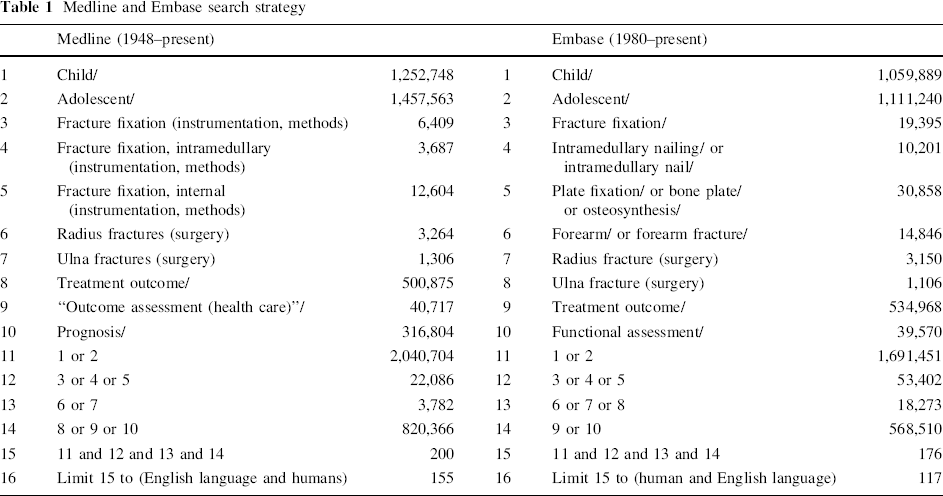
A search was performed of Medline (1948–present) and Embase (1980–present) on 10 September 2011 by the first author (DW) and repeated 1 month later by the second author (RJ). The strategy for these searches is detailed in Table 1. The Cochrane Library was also searched with the terms ‘forearm fracture’, ‘paediatric fracture’, ‘intramedullary nailing’, ‘flexible nailing’ and ‘elastic nailing’. Pubmed was searched with the term ‘pediatric forearm fracture fixation’. Only English-language original studies were included that reported functional outcome following surgical fixation of both-bone diaphyseal forearm fractures in a population with an average age less than 18 years, with comparisons drawn between a group treated with an intramedullary device and a group treated with plate and screws. If there was any disagreement as to whether an article was suitable for full-text assessment, it was included. All levels of evidence were included but case reports and case series with fewer than 10 patients in each group were excluded.
Medline and Embase search strategy
Results
A total of 155 studies were identified in Medline, 117 in Embase and 94 in Pubmed. Twelve were selected for full-text assessment on the basis of their abstract as detailed in Fig. 1. Following full-text assessment, one was found to have fewer than 10 patients in the IMN group and it did not differentiate between groups when reporting functional outcome [20]. One was excluded as functional outcome was not reported [21]. Two were excluded as data specific to each treatment modality could not be extracted for comparison [14, 22]. One was excluded as only two patients had IMN and the fractures were not solely diaphyseal [9]. The Cochrane Library contained one relevant abstract but the full text of the study could not be identified in the archive of the journal as cited [23]. The seven included studies are detailed in Table 2. All the included papers were retrospective comparative studies of level III or IV evidence. No study was randomised but in one case the groups were age- and sex-matched [24]. Three studies looked specifically at older children, thought to have less potential for remodelling [25–27]. Pooled statistical analysis was not attempted due to the inconsistencies of functional outcome reporting. Formal evaluation of methodological quality was therefore not performed as no weighting would be attributed to results.
Flowchart demonstrating the process of article selection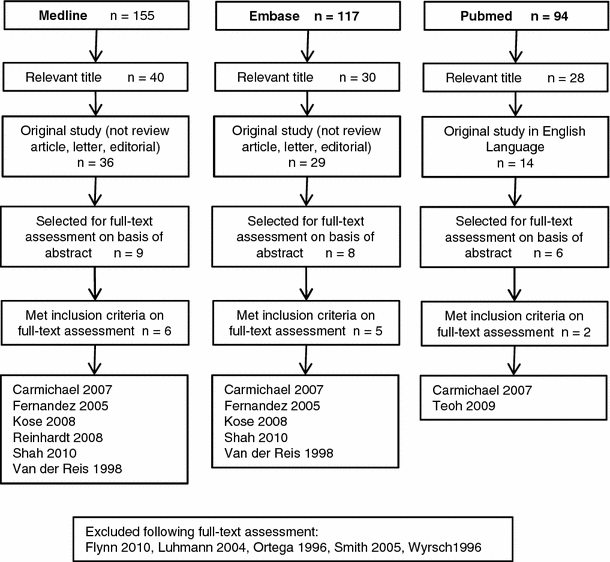
Included studies
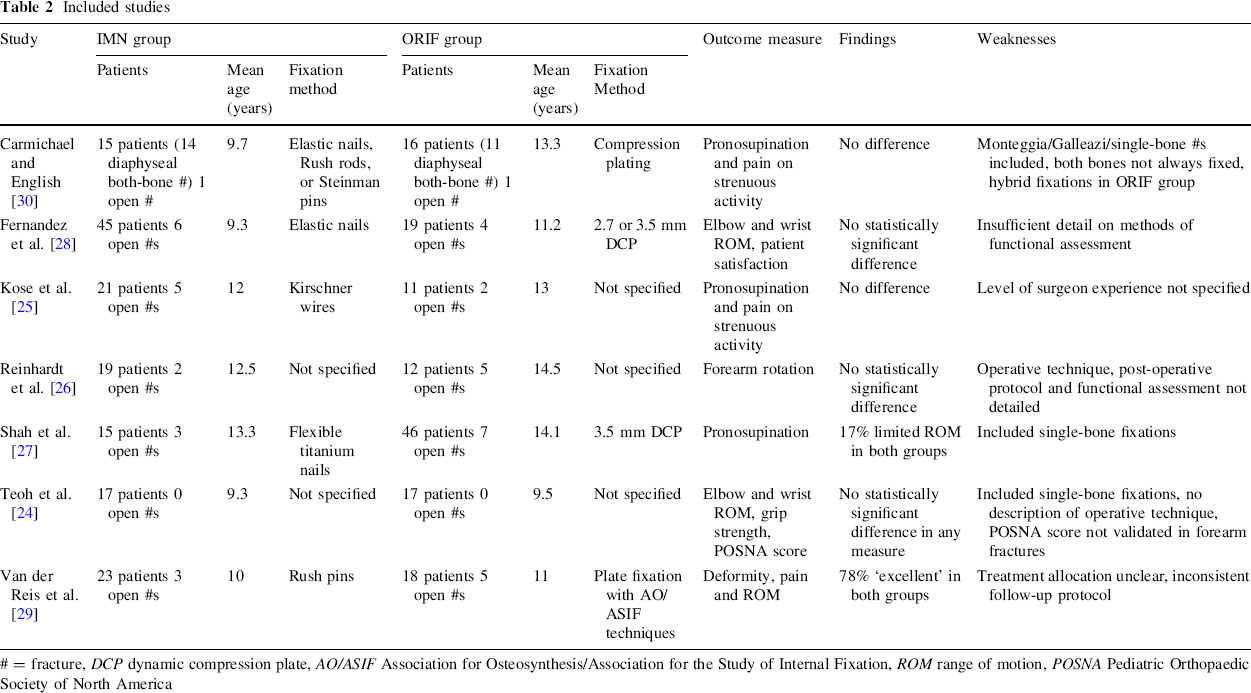
= fracture, DCP dynamic compression plate, AO/ASIF Association for Osteosynthesis/Association for the Study of Internal Fixation, ROM range of motion, POSNA Pediatric Orthopaedic Society of North America
Functional outcome was assessed in various methods, including range of motion, subjective contentment [28], parent-reported functional scores and dynamometric grip strength [24]. No study demonstrated any significant difference in functional outcome. Two studies identified patients in the IMN group with rotational deformity and loss of pronosupination, while no patients in the ORIF group had similar deficit. However, statistical significance could not be attributed [26, 29].
Discussion
On the basis of the results of the included studies, it is not possible to state any significant difference in functional outcome between IMN and ORIF for paediatric diaphyseal both-bone forearm fractures. The studies examine various age groups and feature different treatment modalities, with inconsistencies between them regarding the inclusion of open fractures and the fixation of one or both bones [24, 27, 30]. The study by Teoh et al. [24] stands out in terms of its methodology, with the use of matching, established outcome measurements and a dedicated research review clinic but it is let down by its comparatively small sample size (partly a consequence of the matching process). Two studies reported a few patients treated with IMN who were left with rotational deformity and loss of rotation, while there were no similar deficits in those treated by ORIF. These differences were not highlighted by the authors, as statistical significance could not be attributed, likely due to the small sample sizes.
Important methodological flaws pervaded the studies in this review, first and foremost that of selection bias. Most of these retrospective studies stated that the treatment received was decided by the treating orthopaedic surgeon. Importantly, the ORIF group was older in all seven included studies, which may reflect a conscious decision to treat older children with ORIF, so that anatomical reduction can be achieved in those with less capacity to remodel. It should be noted that three studies looked specifically at older children and found no difference in function [25–27].
Functional outcome is not the only consideration. Cosmetic results may be of high importance in children and two of these studies suggest improved cosmesis with IMN [25, 28]. Three of the included studies demonstrated shorter operative time with IMN [25, 26, 28]. The chance of complications (including non-union) should always be considered when evaluating an operative intervention but the studies do not consistently show a difference in this aspect. The importance of radiographical outcome is questionable as there does not seem to be strong correlation in these studies between restoration of an anatomical appearance on X-ray (namely size and location of maximal radial bow) and the final functional outcome [24, 26, 27].
Since this review shows no evidence of a difference in functional outcome, the authors recommend intramedullary stabilisation for paediatric both-bone diaphyseal forearm fractures due to the other advantages previously described. However, these studies tended to exclude more complex fracture patterns and there is likely to remain a role for ORIF in these cases.
Although these studies have methodological shortcomings, they are of use in generating a hypothesis for further investigation and the authors await a randomised trial to add weight to the evidence in this area. Any further studies should specify single- or both-bone fixation, type of implant and post-operative protocols (especially duration of immobilisation, physiotherapy and removal of metalwork). Outcome measures should include clinician- and patient-reported evaluations using validated research tools, assessing function, cosmesis, and the social and financial implications of each treatment.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.