
Abstract
Purpose:
Unstable forearm shaft fractures in children are preferably treated surgically using elastic stable intramedullary nails. The radius is nailed retrograde from the distal metaphysis. There is a risk of surgery-related soft-tissue complications during the operation. Close evaluation of occult surgery-related soft-tissue lesions has not been possible previously, due to the titanium alloy hardware used in the process. The aim of the present study was to evaluate the potential findings in the surrounding soft tissues after intramedullary nailing of the radius, by using magnetic resonance imaging.
Methods:
The study population comprised 15 pediatric patients with forearm shaft fractures treated by polylactide-co-glycolide biodegradable intramedullary nails and postoperatively evaluated via magnetic resonance imaging. The main outcome was signal abnormality in any tendon at the entry point postoperatively. Secondarily, other changes in the soft tissues related to nailing were determined. Furthermore, the precise location of the entry point and the anatomic characteristics of the soft-tissue tunnel were described.
Results:
In total, 5 of 15 patients (33.3%) had transient signal pathology in a tendon postoperatively. Edema around the superficial radial nerve was detected in 13 of 15 patients (86.7%). The most common surgical approach was between the extensor pollicis brevis and the extensor carpi radialis longus tendons, which was applied in 10 of 15 patients (66.7%).
Conclusions:
One in three patients exhibited transient and occult surgery-related intraparenchymal signal pathology in a tendon, after forearm intramedullary nailing. Caution with surgical prepare of the soft-tissue cleavage is recommended.
Level of evidence:
Keywords
Introduction
Diaphyseal forearm fractures account for 3%–5% of all pediatric fractures.1,2 Elastic stable intramedullary nailing (ESIN) is the preferred treatment for unstable forearm shaft fractures.3–12 With this technique, the pre-bent nail is inserted through a 1–2 cm incision at the lateral side of the distal radius, proximal to the growth plate.4,8,13,14 Despite the bone in that area being superficial, there are still several tubular structures therein that are vulnerable to surgery-related complications, such as the branches of the radial nerve and the abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor carpi radialis longus (ECRL), and brevis tendons (ECRB) (Figure 1). These may be damaged during the operation or postoperatively, while the nail end is left protruding above the bone surface.
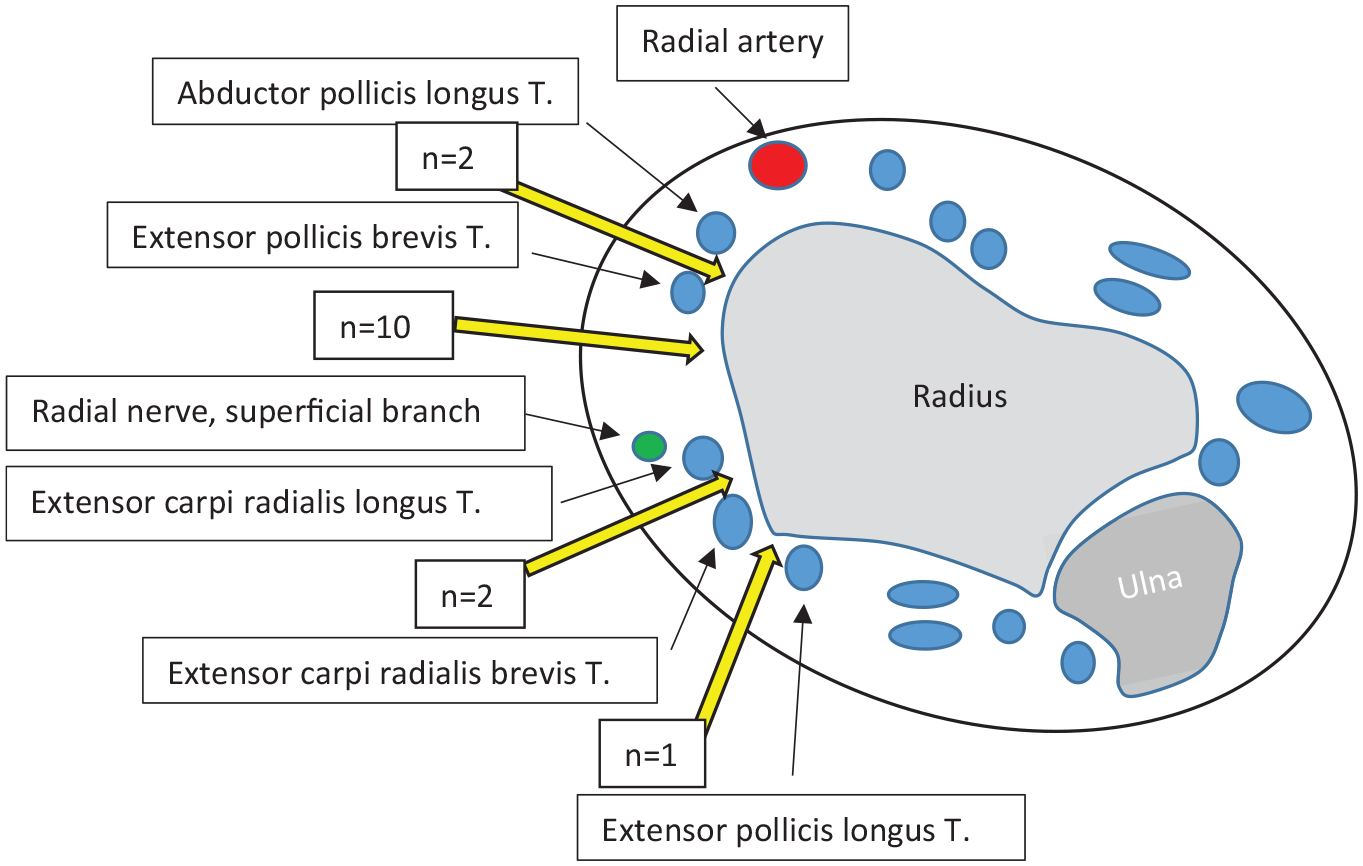
Anatomical soft-tissue structures at the lateral side of the distal radius.
Although intramedullary nails are inserted under both visual and fluoroscopic control, the exact route of the nail and the potential surgery-related consequences to the soft tissues remain unclear. Occult injuries may become detectable in clinical examinations, not during the early stages but upon complete rupture. Because of titanium alloy or stainless-steel implants, imaging investigations through magnetic resonance imaging (MRI) have not been reliable. However, because of the BIN technique of intramedullary nailing using biodegradable polylactide-co-glycolide (PLGA) nails, 15 a comprehensive postoperative MRI of the distal radius can be performed.
The aim of this study was to determine early postoperative soft-tissue findings in MRI related to retrograde nailing of the radius, as well as exact determination of the entry route of nailing until the bone surface.
Materials and methods
An observational study of children aged 8–14 years (mean, 10.5; standard deviation (SD), 1.6), who were treated for unstable forearm shaft fracture by intramedullary nailing using bioabsorbable implants in 2011–2015, was conducted. The study population comprised 15 patients with postoperative MRI, 8 of whom were boys and 7 were girls. The implant material was bioabsorbable PLGA with a tri-calcium-phosphate marker in the tip of the nail (Figure 2). The implants were from Bioretec Ltd., Tampere, Finland. The study was performed at two centers, Oulu University Hospital, Oulu and Päijät-Häme Central Hospital, Lahti, Finland. Patients with open fractures, pathological fractures, previous fractures, significant soft-tissue injury, or infection of the fracture site were excluded. Patients suffering from systemic disease or metabolic bone diseases or who were taking medication affecting bone quality or resistance to infection were excluded. Fractures older than 7 days were also excluded.16,17

Ten-year-old boy with diaphyseal forearm fracture treated with bioabsorbable nails.
As a primary outcome, any abnormal finding of any tendon of the lateral wrist area (APL, EPB, ECRL, ECRB) was recognized. Irritative tissue reaction of the tendon was suspected if there was increased signal within the tendon in at least two consecutive slices of T2 and fat-saturated proton density (PD) images. Local edema around a tendon, referring to peritendon inflammation or tissue irritation reaction, was also evaluated. The lesions of the superficial branch of the radial nerve and the radial artery were studied. However, the radial nerve is such a tiny structure that nerve lesion was considered to be undetectable in imaging; thus, perineural edema was analyzed. Hematoma in any tissue layer at the operation area was recognized and the volume or greatest length was measured. Second, the exact soft-tissue path of the biodegradable nail in the proximal radius was assessed. The surgical approach was lateral in 14 patients and dorsal in 1 patient. In addition to imaging findings, potential functional and sensory defects distally to forearm were evaluated.
The patients underwent MRI imaging using a Siemens Magnetom Espree 1.5 Tesla or Siemens Magnetom Avanto 1.5 Tesla (Siemens, Erlangen, Germany) equipment. The sequences were T1, short tau inversion recovery (STIR), and three-dimensional (3D) T2 fat-saturated gradient echo in the sagittal plane, and T1, T2, and fat-saturated PD in the axial plane. According to the original prospective research plan, the imaging protocol included MRI 1, 3, 6, 12, and 24 months after operation. 16 All patients did not attend all follow-up visits. The first available MRI examination during the postoperative follow-up was performed at a mean of 34 days (range, 4–56 days) and the second MRI at a mean of 122 days (range, 78–203 days) after the operation. Nine out of 15 patients had a third MRI at a mean of 201 days (range, 171–251 days) after operation. All performed MRI examinations with identical imaging protocols during the first follow-up year were analyzed to recognize potential recovery. A pediatric radiologist (M.P.) with 20 years of experience in pediatric musculoskeletal radiology evaluated all examinations. The clinical outcome was evaluated according to grading system described by Price et al. 18 during follow-up visit at mean 122 days (range, 78–203 days) after operation along with second MRI.
Statistical methods
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26 (Armonk, NY, IBM Corp.).
Ethics
This research was based on the prospective, randomized, controlled trial originally approved by the Medical Ethics Committee and the Hospital Ethics Committee of Pirkanmaa Hospital District, Tampere, Finland (§R09231/2009) and recorded in the annals of the Northern Finland Hospital District, Oulu, Finland. The Medical Ethics Committee of Northern Finland Hospital District, Oulu, Finland approved the extension of the study (30.1.2019, 112/2018). Permission for the study was also provided by Päijät-Häme Central Hospital (06.11.2019, D/2219/13.00.00.00/2019). The Finnish National Supervisory Authority for Welfare and Health (Valvira) approved the implant in question for the study purpose in this researcher’s intended study. Written informed consent was obtained from the eligible pediatric patients and/or their guardians.
Results
Postoperative tendon lesions
Five out of the 15 patients showed increased T2 signal in at least one tendon parenchyma; two injuries affected the APL tendon and another two EPB tendon (Table 1). In one patient, the ECRL or the ECRB tendon was injured (Figure 3). It is shown in the images of four out of five patients that the nail end has no contact to the tendons with increased T2 signal. In two patients, the signal abnormality in a tendon is clearly more distally, that is, in the nail tract, than the nail tip on the bone surface. In one patient, the nail tip bulges slightly out from the cortex, and irritation caused by nail tip is possible. However, the signal abnormality within ECRB tendon in this particular case disappeared by 6 months. The postoperative tendon lesions did not proceed to rupture in any patient during the follow-up; instead, the findings disappeared at the second follow-up MRI in all other patients.
MRI findings at the insertion area of the intramedullary bioabsorbable nail in distal radius.
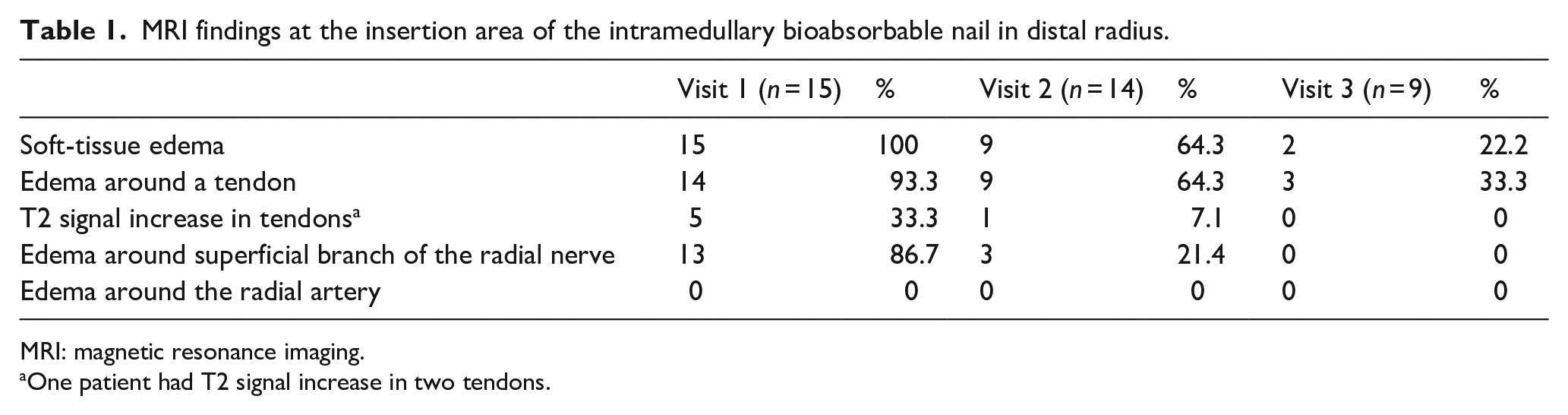
MRI: magnetic resonance imaging.
One patient had T2 signal increase in two tendons.
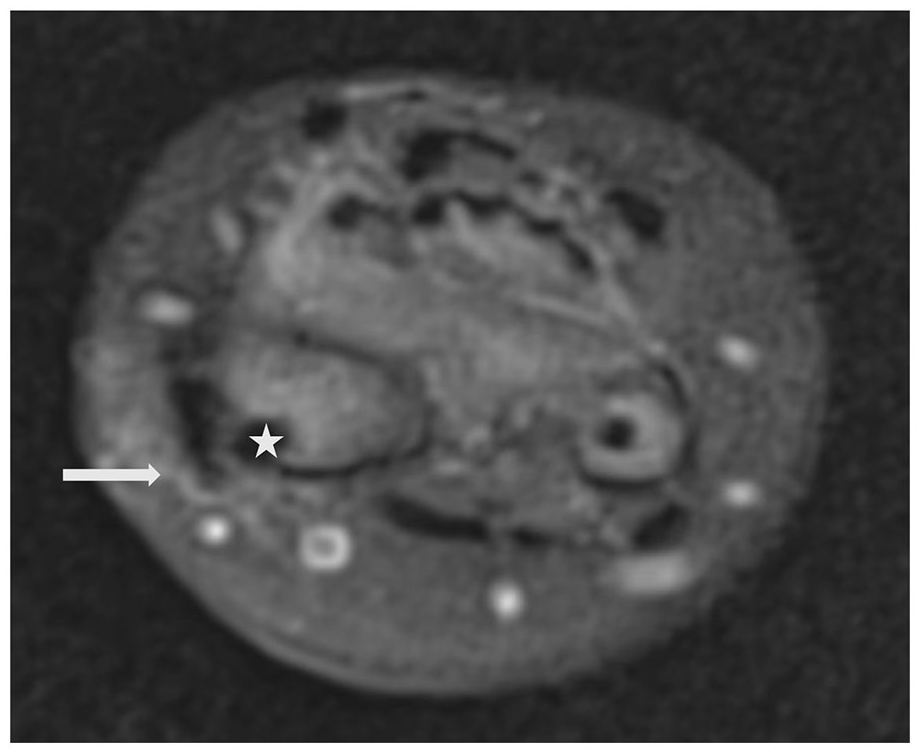
Increased signal in the extensor carpi radialis brevis tendon (white arrow) and edema around the tendon appearing as a high-signal border. The nail (white star) is passing lateral to the tendon. PD fat-saturated image on the axial plane.
Fourteen out of the 15 patients had edema in the surrounding of at least one tendon in the first postoperative MRI. Edema was avoided in one patient whose nail was inserted medial to the ECRB tendon. Five patients had edema around all four tendons located near the radial styloid process, indicating a wide soft-tissue irritation.
Subcutaneous reactions
There was diffuse subcutaneous edema around the nail tract in all patients. By the second postoperative MRI at a mean of 122 days postoperatively, edema had disappeared in 5 out of 14 patients.
Soft-tissue hematomas
No uniform hematomas were found in the study patients.
Tissue irritation around the radial nerve
There was soft-tissue edema in the path of the radial nerve in 13 out of the 15 patients in the first postoperative MRI. The second follow-up MRI showed edema at the vicinity of the radial nerve in three patients. All three underwent a third MRI 6 months after operation without signal abnormalities around the nerve.
Radial artery lesions
The radial artery was not involved or damaged in any patient. The radial artery lies on the palmar side of the radial processus styloideus and away from the nail tract.
Clinical outcome
The objective findings at clinical examination were good/excellent in 13 out of 14 patients. A fair clinical outcome was reported in one patient without signal abnormality in any tendon or around radial nerve at MRI taken at the same follow-up visit. The reason for complaint was painful prominent callus formation of ulnar fracture. By third follow-up visit, the patient’s clinical outcome was good/excellent. There was neither subjective complaint of symptoms related to irritation of superficial radial nerve. One patient experienced implant failure and did not attend the second follow-up visit.
Surgical approach
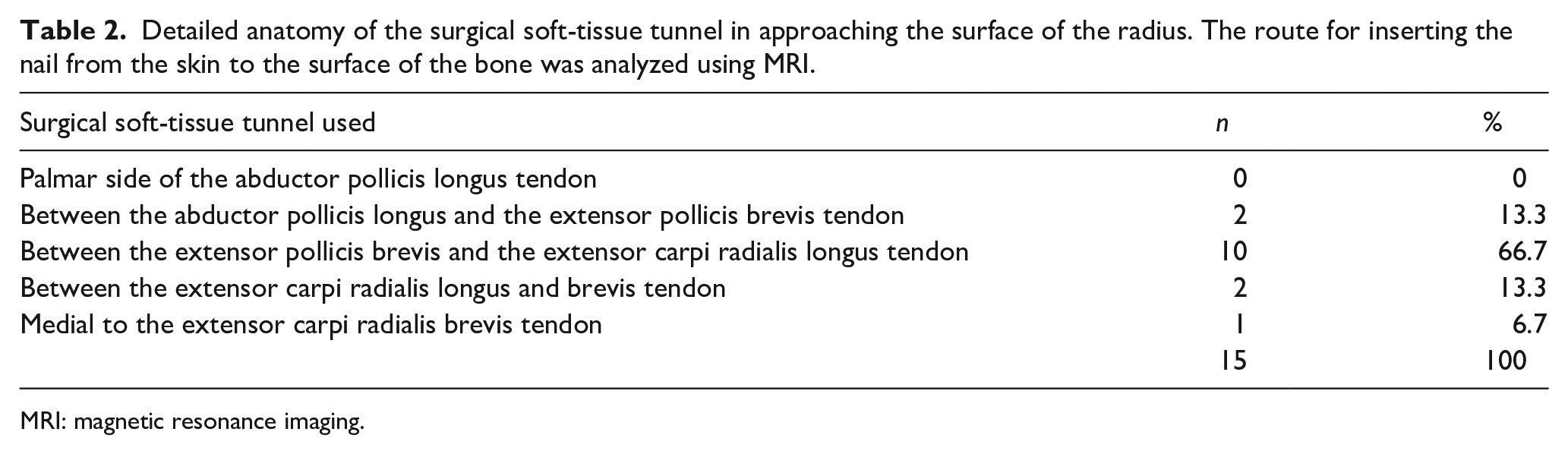
The most common soft-tissue tunnel from the skin to the surface of the bone was between the EPB and ECRL tendons (Figure 4). This route was used in 10 out of 15 patients. In two patients, tissue cleavage between the APL and EPB tendons was applied, and another two nails were placed by using the cleavage between the ECRL and ECRB tendons. In one patient, the nail was inserted medially to the ECRB tendon (Table 2, Figure 1).
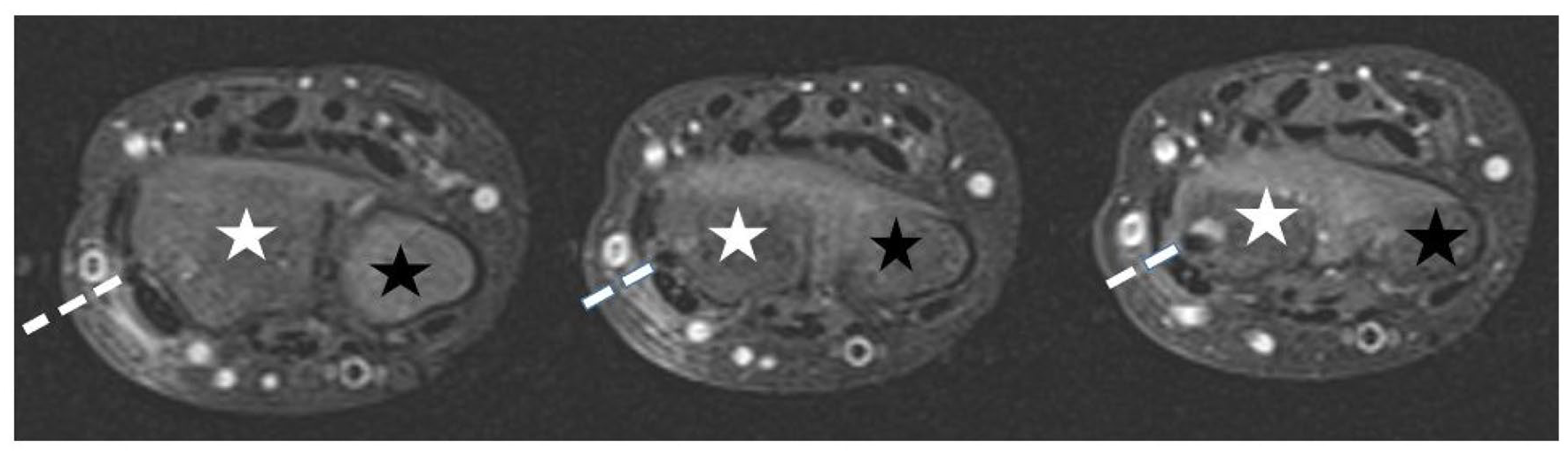
Insertion tract of the nail (dashed line) between the extensor pollicis brevis and the extensor carpi radialis longus tendon in a patient. Three consecutive fat-saturated PD axial images; radius (white star) and ulna (black star).
Detailed anatomy of the surgical soft-tissue tunnel in approaching the surface of the radius. The route for inserting the nail from the skin to the surface of the bone was analyzed using MRI.
MRI: magnetic resonance imaging.
Discussion
The first important result of this study was that one in three patients who had been operated on using intramedullary nailing of the radius had surgery-related abnormal soft-tissue findings in any tendon at the wrist area postoperatively. The signal abnormality within tendons disappeared during follow-up indicating transient irritation. At second follow-up, almost all the patients (14 out of 15 cases) had other tissue irritation reactions, such as edema, in the surroundings of a tendon. These findings may be due to surgical dissection and insertion of the implant, and thus have potentially clinical importance. There are previous reports of increased T2 signal indicating edema due to ongoing degradation process around the bioabsorbable device within bone.19,20 Nevertheless, soft-tissue edema was found at around the nail insertion canal, away from the nail location inside the bones, meaning that tissue reaction was an independent finding.
In the literature, ruptures of the extensor pollicis longus (EPL) tendon or extensor carpi radialis tendons have been reported6,13,21,22 as a consequence of friction over a sharp nail end. Complete rupture is easily identified clinically, and reconstructive surgery is necessary in these cases. With bioabsorbable implants, such tendon rupture is not probable because the nail is cut tangentially on the surface of the bone. However, while there was no complete tendon rupture in this study, retrograde nailing still seemed to irritate tendons in one-third of patients, treated by intramedullary nailing. We therefore suggest that irritation of a tendon may be a result of the surgical procedure per se, and not only based on the protruding tip of a metal implant.
As another main finding, we found that the most common surgical approach to reach the cortical bone of the distal radius is the tissue cleavage between the EPB and ECRL tendons (67%). From an anatomic point of view, this approach offers straight access to the distal radius, which explains its popularity. Treating surgeons had not recorded the exact soft-tissue route in the operation note but just performed “lateral” or “dorsal” approach. In the future, the correlation between surgeon’s own view of the used soft-tissue canal and the objective MRI findings of the soft-tissue canal would be analyzed. Nevertheless, we found in this study edema at the area of the radial nerve course in a great majority of the patients (13 out of 15 patients, 87%) in the first postoperative MRI. The superficial branch of the radial nerve lies laterally to radius, and more dorsal opening beyond the extensor carpi radialis brevis may be safer soft-tissue route, in regard to the position of the radial nerve.21,22 In using the dorsal approach in pediatric forearm shaft fracture treatment with ESIN, Lister’s tubercle is generally palpable. 14 On the contrary, the dorsal approach has been reported to cause late EPL tendon ruptures.23,24 In this study, dorsal opening was performed in one patient, and the case was not associated with any tendon pathology.
In general, the complications related to the intramedullary nailing of children’s forearm fractures include delayed union, non-union, refracture, implant failure, nerve palsy, tendon injuries, compartment syndrome, infection, and synostosis.5,6,12,13,21,22,25 The reported complication rates vary from 7.7% to 24.4%. The complications related to the insertion site of the radial nail are infections, tendon ruptures, and superficial radial nerve injuries. The standard procedure in ESIN is to cut the nail above the bone surface to make the removal of the nail possible after fracture healing.13,14 This kind of sharp tip of the nail may cause soft-tissue damages. However, also the surgical procedure itself may harm the sensitive soft-tissue structures, which was found in this study. Our findings warrant caution in surgical preparation of the soft tissues and making a route to the bone, in order to avoid the potential radial nerve injury and tendon lesions, even the occult ones.
As a limitation of the study, there were no more than 15 patients treated with biodegradable implants and were investigated through MRI, who comprised the study population. In the future, a larger study setting is necessary to confirm the findings of this pioneering research. When using a small study population, more infrequent soft-tissue injuries may not have been revealed. A larger study population would also aid in conducting a comparison of the different surgical approaches. Based on this small pilot study, we were not able to draw any conclusions regarding the clinical importance of these MRI findings. However, our study adds new insights to the literature regarding the surgical technique and soft-tissue reactions in the operation tract. As a fundamental strength of the study, BIN technique with biodegradable implants was utilized for pediatric patients with an unstable forearm shaft fracture, making postoperative MRI possible. MRI could not have been used previously without significant artifacts because traditional implants are made of titanium alloy or stainless steel. To the authors’ knowledge, this study is the first to comprehensively analyze the exact anatomical location of the nail entry path and the soft-tissue findings after retrograde intramedullary nailing of the radius.
Conclusion
One in three of the pediatric patients treated with retrograde intramedullary nailing of the radius presented occult surgery-related intraparenchymal tendon MRI signal alteration close to the nail entry site. The majority of the patients showed signal pathology at the superficial radial nerve surroundings. These surgery-related soft-tissue findings at MRI were not related to clinical symptoms in this small study. Further prospective adequately powered studies are required to confirm our findings.
Footnotes
Acknowledgements
Juhani Merikanto, MD, PhD, is highly acknowledged for the conceptualization, methodology, and project administration of the original study protocol for biodegradable intramedullary nailing of children’s forearm fractures. We also thank Jarmo Lehtonen, MD, and Martti Soiva, MD, PhD, for organizing the medical imaging of the study patients in Päijät-Häme Central Hospital. Furthermore, we thank Sini Tompuri, MD, for her accomplished help during the study in Päijät-Häme Central Hospital.
Author contributions
Conceptualization: J.-J.S. and M.P.; methodology: M.P. and J.-J.S.; software: M.P.; validation: J.-J.S., M.P., and J.N.; formal analysis: M.P. and J.-J. S.; investigation: M.P., A.K., and J.-J.S.; resources: J.-J.S. and J.N.; data curation: M.P.; writing—original draft preparation: M.P.; writing—review and editing: all authors; visualization: M.P.; supervision: J-J.S. and J.N.; project administration: J-J.S. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.-J.S. declares research grants from Alma and KA Snellman Foundation, Emil Aaltonen Foundation, Foundation of Pediatric Research, and national VTR-funding, J.-J.S. has consulted with Bioretec Ltd for surgical issues. J.-J.S. is an expert at Patient Insurance Center. J.-J.S. is the Section Editor of Scandinavian Journal of Surgery and member of the editorial board of Journal of Children Orthopedics. A.K. declares research grants from national VTR-funding for the years 2017 and 2018, and these are transferred to be consumed in the years 2021–2022. These fundings were granted for another study. A.K. declares grant from Erkki Poikosen säätiö (Erkki Poikonen’s Foundation) in 2019 for preventive medical work, which was not linked with this study. The others declare no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bioretec Ltd has given the bioabsorbable intramedullary nails and instruments used in operations of this study to Päijät-Häme Central Hospital and reimbursed for costs of imaging studies to Päijät-Häme Central Hospital. Bioretec Ltd has paid the local transportation expenses of the study patient concerning the study visits to Päijät-Häme Central Hospital. Otherwise, this research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors. The authors received no financial or material support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants and/or their guardians included in the study.