
Abstract
Flexible intramedullary nailing is a common method used to treat pediatric femur fractures. Complication rates can be high, but most complications are considered minor and do not result in additional unplanned surgeries. Proximal nail penetration is a complication that has only been described once before. The penetration may be asymptomatic, but is still best to be avoided. Two cases of proximal nail penetration of the femoral neck region during nail insertion are presented. A review of the literature with regard to complications and suggestions for avoidance of proximal nail penetration is offered.
Introduction
Flexible intramedullary nailing has become an accepted treatment for pediatric femur fractures [1–6]. Complications of nailing have been described as occurring in up to 62% of cases [7]. Complications that do not require further unplanned surgery include pain that may or may not limit motion, hardware prominence, delayed union, clinically insignificant malunion, neuropraxia, and mild insertion site infections [7–10]. Complications that can require additional unplanned surgery include very prominent hardware, loss of reduction, compartment syndrome, nerve injuries, and deep infections [7–10]. Acute synovitis of the knee from insertion site intraarticular penetration has been described [11].
Proximal nail penetration has been described only once previously. This previous report described a case of proximal penetration of the tip of the nail through the femoral neck leading to a sciatic neuropraxia that resolved with nail repositioning [9]. Intraoperative imaging did not diagnosis this penetration, and it became apparent 2 weeks after the injury. One other study mentions a proximal nail penetration among the 43 patients who had undergone elastic intramedullary nailing. The authors repositioned the nail and include a radiograph documenting the proximal penetration [12]. Proximal nail penetration of the femoral neck can occur during flexible nail insertion even when fluoroscopy is used. Two cases are used to illustrate how nails inserted in a retrograde fashion can penetrate the femoral neck during insertion or final positioning. In these two cases, the nail penetrations were asymptomatic and had no consequences. However, if a penetration were to lead to a femoral neck fracture in a young child, then it could have serious consequences. Therefore, the potential for such a complication should be considered because it is not always obvious on intraoperative radiographs.
Materials and methods
This was a retrospective medical chart review approved by our Institutional Review Board. We looked at all pediatric patients who had undergone flexible intramedullary nailing of femur fractures during a 5.5-year period from 2001 to 2006. To be included in the study patients must have had a Synthes titanium elastic nail (Synthes Corp., Paoli, PA) retrograde insertion from distal to proximal.
Results
We identified 19 patients who had retrograde flexible intramedullary nailing of their femur fractures during a 5.5-year period. The average age of these patients was 9.9 years. There were 5 girls (26%) and 14 boys (74%) Of those patients, two (10.5%) were noted to have proximal femoral neck penetration at follow-up in the clinic. Those two cases are described below.
Case 1
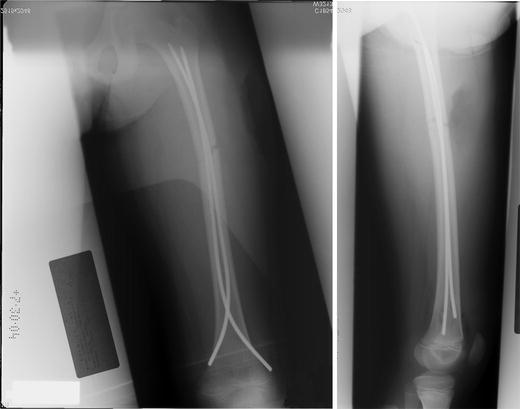
A 9-year-old boy was knocked down while playing with a dog. He sustained a transverse femur fracture at the level of the middle and proximal one-third junction. He was cleared of other injuries and underwent flexible intramedullary nailing. The surgery was done the next day by a pediatric orthopedist. A retrograde technique was used to insert the nail from distal to proximal. The fracture was shortened about 3 cm, and an adequate reduction could not be obtained. A limited open reduction was used to remove entrapped muscle and button-holed periosteum in order to pass the nail. Two 3.5-mm Synthes flexible nails (Synthes Corp., Paoli, PA) were inserted from distal to proximal. Intraoperative fluoroscopy and conventional radiographs were taken that showed good reduction of the fracture (Fig. 1). Note that the lateral view does not include the proximal neck region well.
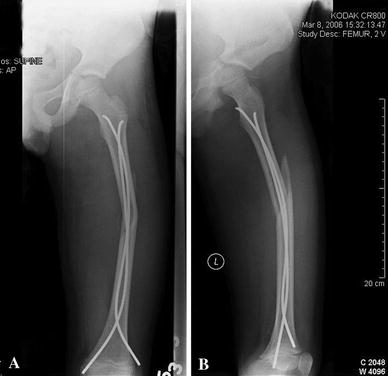
A clinic follow-up 10 days after surgery showed adequate fracture alignment with well-placed nails. The lateral radiograph (Fig. 2) was not orthogonal to the sagittal axis of the femur and as such was not a true lateral view, but was actually an oblique view. A quality lateral radiograph 17 days after surgery shows that one of the flexible nails is protruding through the posterior femoral neck/intertrochanteric region (Fig. 3). The anteroposterior (AP) radiographs do not show any proximal migration of either of the flexible nails. The patient and parents were notified of the findings, and a decision was made to observe him.

The patient was asymptomatic with regard to the proximal nail and his fracture was allowed to heal without nail repositioning. He underwent elective hardware removal 1 year after surgery without complications. His weightbearing was protected and activities limited for 6 weeks following removal. Six weeks after removal he was allowed activities. He returned to full activities and at present is without complaints, pain, or limb-length inequality.
Case 2
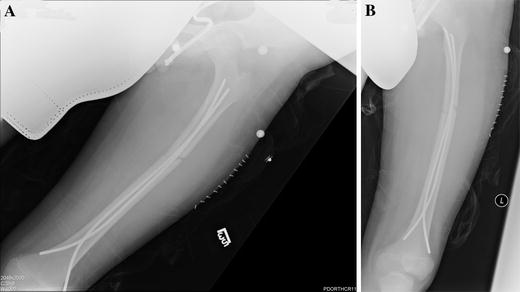
An 8-year-old boy sustained a long oblique fracture while playing football. The fracture was shortened about 2 cm, and the surgery was done at night by an adult orthopedist. The patient underwent closed reduction and flexible intramedullary nailing with two retrograde 3.0-mm Synthes flexible nails (Synthes Corp., Paoli. PA). The intraoperative radiographs showed adequate reduction, but were taken prior to final hardware placement (Fig. 4). The uncut nails were then cut close to the skin and tamped into place after the final radiographs. At the 9-day postoperative follow-up in the clinic, the nail tip was noted to be protruding through the proximal femoral neck/intertrochanteric region similar to the first case (Fig. 5).

The patient and parents were informed, and a decision to observe was made. The fracture had angulated slightly by the time of first follow-up. The fracture pattern was axially unstable because it was a long oblique pattern. The parents were offered revision surgery with external fixation or open reduction and internal fixation, but declined. At his 6-month follow-up, the patient has about 1.5 cm of shortening on the fractured side. The hardware was removed uneventfully.
Discussion
Most complications associated with the use of flexible nails for pediatric femur fractures are well described. The most frequent complication is nail insertion site irritation [7–11]. Narayanan et al. noted that patients with nails protruding more than 10 mm from the cortex were 4.5 times more likely to complain of insertion site pain [9]. Complications noted in that study, in order of prevalence, were irritation at insertion site, malunion, loss of reduction, nail migration/skin perforation, refracture, neurological deficit, and superficial wound infection [9]. In a study by Flynn et al. [10], problems were categorized as those with satisfactory results and those with poor results. The problems encountered in patients with satisfactory results, in order of prevalence, were malalignment of 5°–10°, 1–2 cm of limb length inequality, soft tissue irritations and nail prominence, refracture after nail removal, and nail back out. Of the 58 fractures, the only poor result was an angulation of 20° of varus [10].
Complications, such as angulation, are more frequently encountered when flexible nails are used in fracture patterns deemed unstable [7] or in fractures located in the proximal one-third of the femur [10]. Mismatched nail sizes have also been correlated to loss of reduction or malunion [9]. The patient described in case 2 of the current report did have an unstable fracture pattern and had both angulation and fracture shortening. Sink et al. reported a 62% complication rate and divided the complications into minor and major [7]. Minor complications did not require an unplanned surgery, while major complications did require unplanned surgery. Luhmann et al. also noted a high complication rate of 49% in 21 of the 43 patients [13]. They had 18 minor postoperative complications and two major complications.
Narayanan et al. described a case of proximal nail penetration of the femoral neck [9]. The patient presented after 2 weeks with a sciatic neuropraxia. Radiographs revealed a very prominent nail that was not noted on intraoperative AP radiographs, but was very noticeable on lateral radiograph. The neuropraxia resolved with nail repositioning, and good intraoperative films were recommended to avoid this complication. Buess also describes a proximal nail penetration that was treated with nail repositioning [12].
The two cases presented herein both had asymptomatic proximal femoral neck penetration. Neither of the patients’ intraoperative films demonstrated the femoral neck penetrations. Case 1 was performed by a pediatric orthopedist, and the other was performed by an adult orthopedist on call. The first case had a transverse pattern suitable to flexible nailing, while the second had a long oblique pattern. Long oblique and spiral patterns can be unstable to flexible nailing [6]. Nineteen cases in 5 years are a small number of patients, and inexperience could have played a role in the two-nail penetration described in this report.
In both cases, the intraoperative radiographs were less than ideal. In one case the lateral radiograph did not include the proximal femur (Fig. 1). The fracture was visible on both AP and lateral radiographs, and a decision was made not to perform repeat radiographs. The follow-up films taken in the clinic were also suboptimal. Because the patient was in pain, obtaining a true lateral was difficult. It was thus decided to accept the oblique view (Fig. 2), which does not demonstrate proximal nail penetration well.
The second case had intraoperative radiographs before the final nail seating (Fig. 4). After the nail is trimmed it is tamped into place, which is likely when the penetration occurred. The early follow-up radiographs showed the proximal penetration (Fig. 5). The second case can also be used to point out some of the technical difficulties that occurred and may have contributed to penetration and secondary displacement. Ideally, the two nails should be opposed with their bow at the fracture site to create an internal splint [5]. As the nails are inserted their orientation must be controlled with the T-handle so the nails do not cross each other and so that the proximal insertion can be precisely controlled [5]. The second case had nails that were wrapped around one another, which can make it difficult to control the individual nail's proximal insertion points precisely. This case also had nails with both of their concavities posterior and not crossing at the fracture site, which may have contributed to the secondary displacement after surgery (Figs. 4, 5).
Fluoroscopy should be used intraoperatively, and attention should be focused on the fracture site and the proximal extent of the nail. Both the AP and lateral projections are needed. The nail should not be directed in an anterior or posterior direction, which is best demonstrated on a lateral view. During final seating of a nail the focus is often on the AP projection. The AP projection is easily obtained and is usually the projection used to judge how far proximal the nail is to be inserted. The lateral projection is more difficult to obtain, but is essential to avoid neck penetration. A frog leg lateral view is relatively easy to obtain with a patient under anesthesia. The penetration can occur during initial insertion of the nail or during the final tamping performed after the nail is trimmed. Careful attention should be paid during insertion, and final radiographs should be closely examined. Any substandard radiograph should be repeated while the patient is still in the operating room. Even though penetrations may be asymptomatic or, as in this case, without consequences, we recommend that any nail penetration of the femoral neck region should be repositioned if noticed intraoperatively.
Conclusion
Proximal femoral neck penetration can occur during insertion of a retrograde flexible nail in pediatric femur fractures. Careful attention to both AP and lateral projections on fluoroscopy can avoid this complication. The lateral projection is needed during final seating to avoid anterior or posterior directed nail tips, which may penetrate the femoral neck. The nails should be centrally located on both the AP and lateral projections. The penetration may be asymptomatic, but it creates a stress riser in the femoral neck region and is best avoided.
Footnotes
Acknowledgments
The authors gratefully acknowledge the editorial assistance of Kristi Overgaard during the preparation of this manuscript.