
Abstract
Introduction:
Elastic stable intramedullary nailing is widely recognized for treating pediatric forearm fractures due to its stable fixation and minimal impact on soft tissue. Traditionally, casting has followed elastic stable intramedullary nailing; however, recent studies question its necessity. This study evaluates the outcomes of omitting casts post-elastic stable intramedullary nailing, examining healing speed and quality of life compared to cases where casting was applied.
Materials and Methods:
A prospective study was conducted from 2022 to 2024 in an urban hospital, where children with both-bone midshaft forearm fracture were randomized to receive or not receive casting after elastic stable intramedullary nailing. Age- and sex-matched patients were selected to allow for accurate comparison. The study included patients aged 5 to 14 years. Outcomes were measured using radiographic scores and quality-of-life assessments.
Results:
From a total of 355 patients, 136 cases were included in the assessment. Analysis indicated faster healing in patients without postoperative casting, as evidenced by higher REBORNE scores at 3 weeks and 2 months. Quality of life, measured by the Pediatric Quality of Life Inventory, was also significantly improved in the no-cast group at 6 weeks.
Discussion:
Our findings suggest that elastic stable intramedullary nailing provides sufficient stability for both-bone midshaft forearm fracture, making additional casting unnecessary. Early mobilization led to better functional outcomes without increasing complications. Although some minor early discomfort was reported, the cast-free approach proved effective and safe.
Conclusion:
Elastic stable intramedullary nailing remains the gold standard for treating pediatric forearm fractures. Our preliminary results indicate that for both-bone midshaft forearm fracture, elastic stable intramedullary nailing can be safely performed without postoperative casting, promoting faster healing and better patient satisfaction.
Introduction
Pediatric both-bone midshaft forearm fractures (BBFF) represent a frequent type of injury, accounting for approximately 3%–6% of all fractures in children and reaching an incidence rate of up to 35.9 per 100,000 person-years, with peak rates in girls at age 10–12 and boys at age 12–14 attributed to the pubertal growth spurt and increased activity levels.1 –3 The incidence of pediatric BBFF is almost twice the incidence in adults, it is increasing worldwide, and the reason is yet to be determined.1,4 One proposed cause is the rising prevalence of obesity, which is established as a significant risk factor in pediatric populations. 5 Regarding laterality, BBFF shows a notable tendency toward the nondominant arm, likely due to the use of the dominant right arm to break falls or engage in activities that increase the risk of injury to the opposite side.3,6
Since its introduction by Metaizeau and Prevot, elastic stable intramedullary nailing (ESIN) has become the gold standard technique for treating pediatric forearm fractures due to its stable fixation with minimal soft tissue disruption. 7 ESIN provides excellent functional results in children with high rates of healing and seldom complications, and without interfering with growth.8 –10 It is a widely accepted surgical technique for treating pediatric forearm fractures, particularly when fractures are unstable or displaced. The advantages of this technique include cosmetic incisions for nail insertion, minimal to no periosteal disruption, the potential for smaller incisions during open reduction if necessary, and reduced implant costs compared to traditional plate-and-screw constructs. 11 Postoperative management has often involved immobilization in plaster casts, but recent studies have debated the necessity of using such casts versus forgoing them, strengthening the original indications of Metaizeau. 12
Our study aimed to assess whether pediatric patients with BBFF, treated with ESIN, could benefit from early active motion and rehabilitation without the need for postoperative casting.
Materials and methods
Study design
The investigation was carried out at the Pediatric Orthopedics Outpatient Clinic, part of the “Grigore Alexandrescu” Children’s Emergency Clinical Hospital in Bucharest, Romania. This clinic serves as an essential primary healthcare resource for children living in both the urban environment and the adjacent areas. The study received approval from the hospital’s ethics committee on September 10, 2021, and was assigned identification number 17. Written informed consent was obtained from the parents or legal guardians of all participating children. Data collection spanned from January 2022 to January 2024. Figure 1 illustrates the selection process.
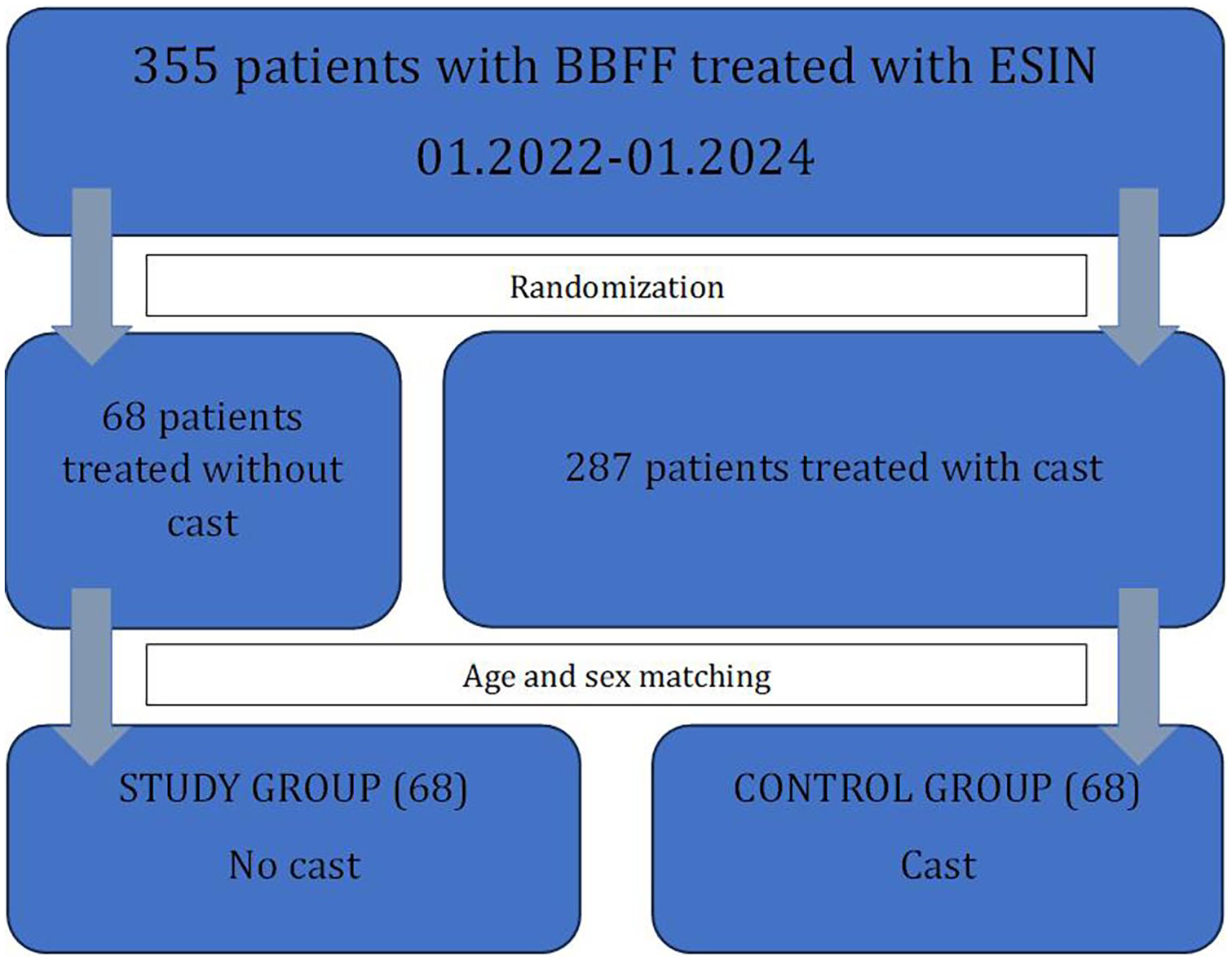
A diagram that shows the patient selection for the study. To enhance the data quality, after establishing the study group through randomization, we were able to match a control group from the entire patient pool treated in the selected timeframe.
Participants
A prospective, single-center investigation occurred from January 2022 to January 2024. The study involved children ranging from 5 to 14 years old who presented as emergencies with BBFF.
The inclusion criteria comprised a positive diagnosis of BBFF that are classified as AO (Arbeitsgemeinschaft für Osteosynthesefragen) type 2R2A and 2U2A—denoting simple diaphyseal fractures of the radius and/or ulna—midshaft fractures that are angulated without comminution, treated through closed reduction and ESIN, informed consent to participate in the study, and complete clinical and radiological follow-up until healing or at least 6 months.
The exclusion criteria encompassed the absence of patient history or informed consent, mental health comorbidities, complex trauma with open fractures/floating elbow/polytrauma that may alter the healing process, medical comorbidities, and open reduction (evacuation of the healing callus may interfere with the healing process).
The age selection for this study was based on established treatment protocols for pediatric forearm fractures. Specifically, patients under five were excluded from the ESIN treatment group, as they typically undergo closed reduction and casting. Conversely, children older than 14 years were excluded from ESIN treatment due to the preference for internal fixation with plates and screws, which is commonly indicated in adolescents with more mature skeletal structures. Thus, the study primarily focused on patients aged 5–14 years, where ESIN is the treatment of choice for BBFF, providing a balance between stability and the potential for early mobilization.
Study procedure
Following triage, patients underwent clinical assessment through anamnesis, a comprehensive physical examination, including evaluation of vascular supply distal to the injury, and a neurological assessment. The diagnosis of BBFF was confirmed via anteroposterior (AP) and lateral X-ray imaging. A temporary splint was applied for pain management, in conjunction with intravenous analgesics. Surgical intervention was performed on the same or the following day. The allocation of patients into the no-cast (n = 68) and cast (n = 287) groups was performed using a randomized distribution approach. Patients in the no-casting group were instructed to begin active movements from the first postoperative day. Sutures were removed on postoperative day 14. The control group consisted of patients who received postoperative immobilization with an above-elbow cast for 3 weeks. Both groups were clinically assessed postoperatively using the Pediatric Quality of Life Inventory (PedsQL) instrument.
ESIN was performed on the translucent table through the same technique: retrograde nailing for the radius through a lateral distal entry point, and antegrade nailing for the ulna through the proximal olecranon entry point. The diameter of the selected intramedullary nail was 40% of the intramedullary canal at the isthmus. 13 Figure 2 illustrates the AP and lateral X-ray of a 6-year-old patient before and after ESIN.
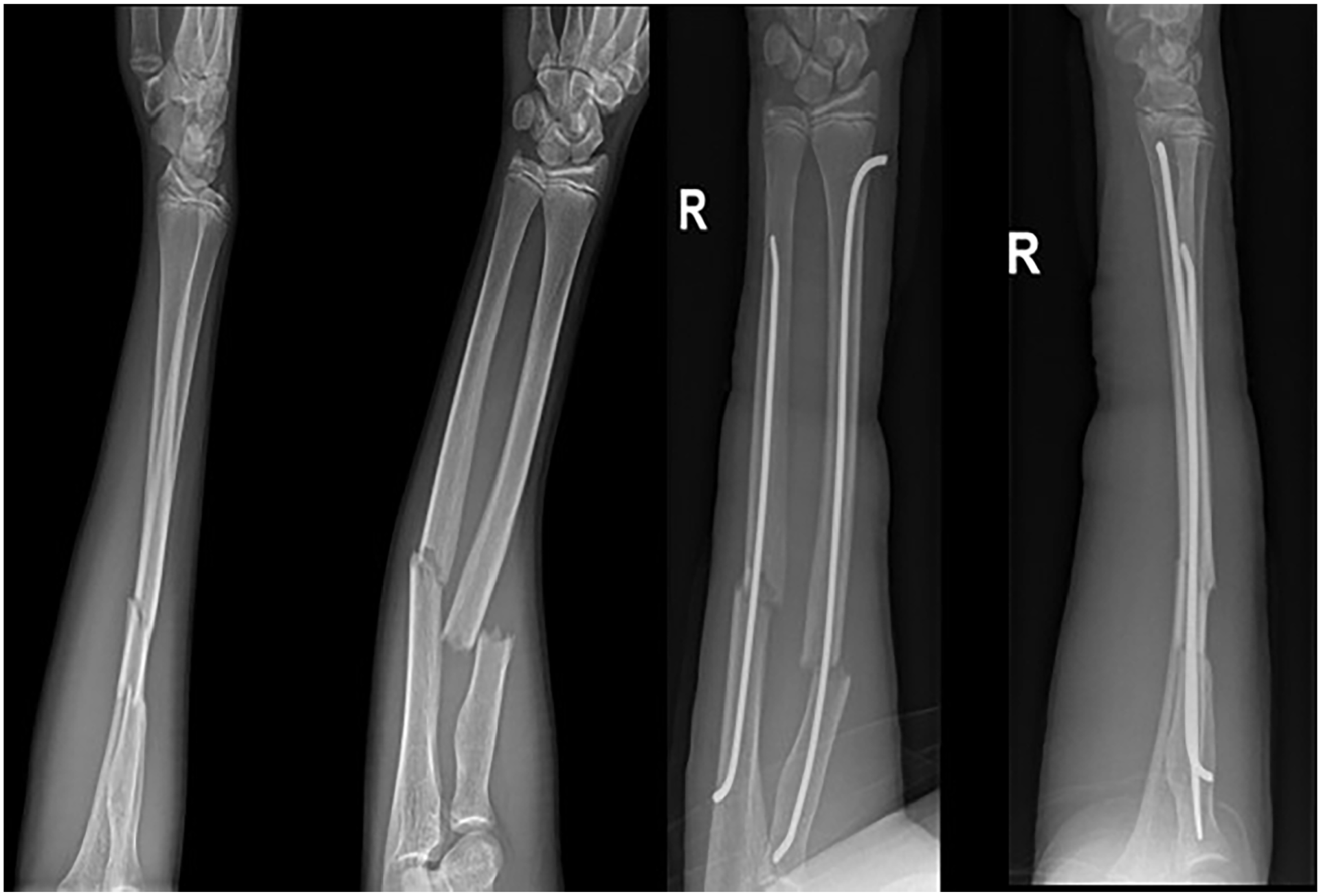
AP and lateral views pre- and postoperative of a 14-year-old who suffered a transverse radial and oblique ulnar BBFF.
Patients underwent clinical and radiological follow-up on postoperative day 1, as well as at 3 weeks, 6 weeks, 3 months, and 6 months postoperatively. PedsQL was conducted at 6 weeks postoperatively, based on the child’s or the parents’ evocative capacity.
Participants in the study were systematically monitored for potential short-term complications, such as elevated pain levels, fracture displacement, and issues related to sutures, and for long-term complications that can occur within 6 months, such as iterative fracture, nonunion, limited or loss of range of motion, or pseudarthrosis.
The PedsQL is a widely used tool to assess the health-related quality of life in children and adolescents. 14 The PedsQL evaluates multiple domains of a child’s well-being, providing a comprehensive understanding of how a specific health condition, such as a fracture, impacts various aspects of daily life, including physical, emotional, social, and school functioning. 14
The REBORNE callus score is a radiographic scoring system designed to assess the quality and progression of callus formation in bone healing, particularly in the context of pediatric fractures. This score is calculated by summing the cortical scores for the internal, external, anterior, and posterior aspects of the fracture site, which are then divided by 16. It is only valid if at least three cortices can be evaluated.
Statistical analysis
Information was gathered and stored in the institutional informatics system. IBM® SPSS® Statistics (Version 26, IBM; Armonk, New York, USA) and Microsoft Excel Office 2016 (Microsoft; Redmond, Washington, DC, USA) were utilized for data analysis. The data encompassed categorical qualitative variables such as sex, as well as continuous quantitative data, including age at evaluation, REBORNE callus score at 3 and 6 weeks, callus index (CI) at 3 and 6 weeks, and PedsQL at 6 weeks.
The Kolmogorov–Smirnov test was used to test for a normal distribution, and the results (KS Statistic, p-value) indicated that the data was not normally distributed. Therefore, the Wilcoxon signed-rank test, effect size, and visual representations were performed. Statistical significance was attributed to results where the p-value was less than 0.05.
Results
A total of 355 patients were admitted for surgery, of whom 287 were allocated to the cast group and 68 to the no-cast group, as seen in Table 1. To enable accurate comparison, age and sex-matching were performed, resulting in two equal-sized groups. The no-cast group was considered the study group, while the cast group was the control group. A prospective analysis was conducted further for both groups in a total of 136 children. The cohort included 112 male patients (82.35%) and 24 female patients (17.65%), aged 5–14 years. The overall mean age at diagnosis was 9.88 years, SD = 3.13, CI 95% [9.38–10.43]. Among male patients, the mean age was 10.55 years, whereas for female patients, it was 6.75 years. 86.76% of the fractures were oblique, and 13.24% were transverse. The study group (68) started active movements from the first day postoperatively, and the control group (68) had a postoperative cast for 3 weeks.
Demographics of the patients treated with ESIN and early active movement (left column) and with ESIN and plaster cast (right column).
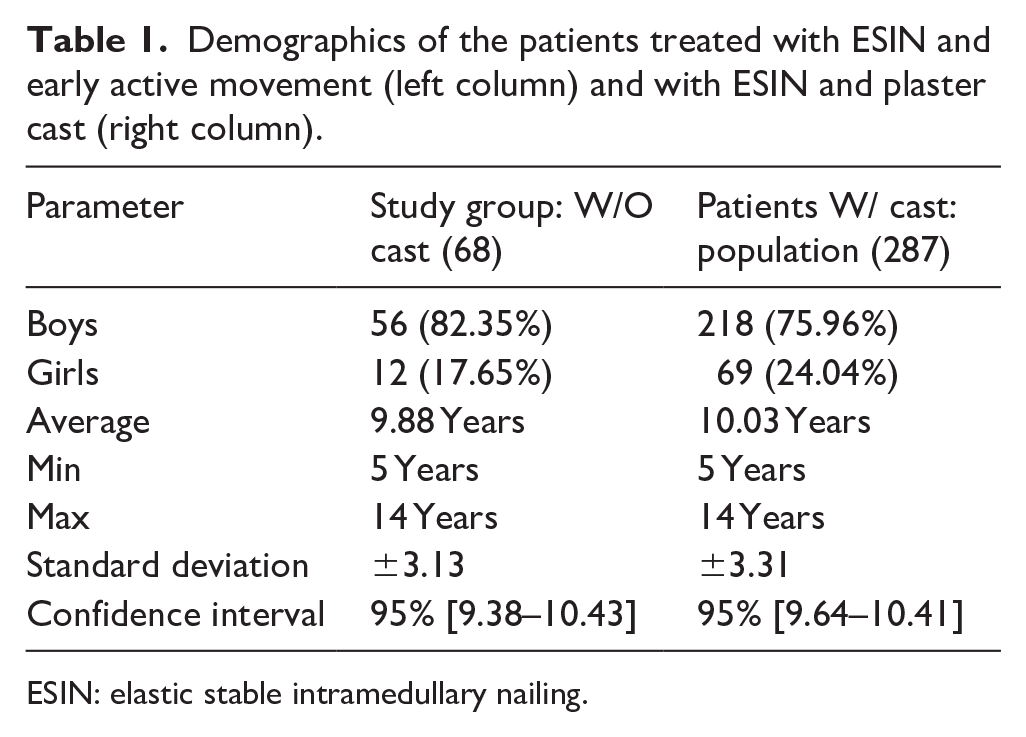
ESIN: elastic stable intramedullary nailing.
Table 1 illustrates the basic demographics for the study group and the whole cohort of patients classically treated with ESIN and postoperative cast. The control group was further selected through age- and sex-matching from the patient pool of 287.
Clinical and radiological assessments were conducted according to protocols.
Figure 3 illustrates the AP and lateral X-rays of two boys aged 7, representing a study pair. The callus differences are illustrative of the REBORNE score differences.
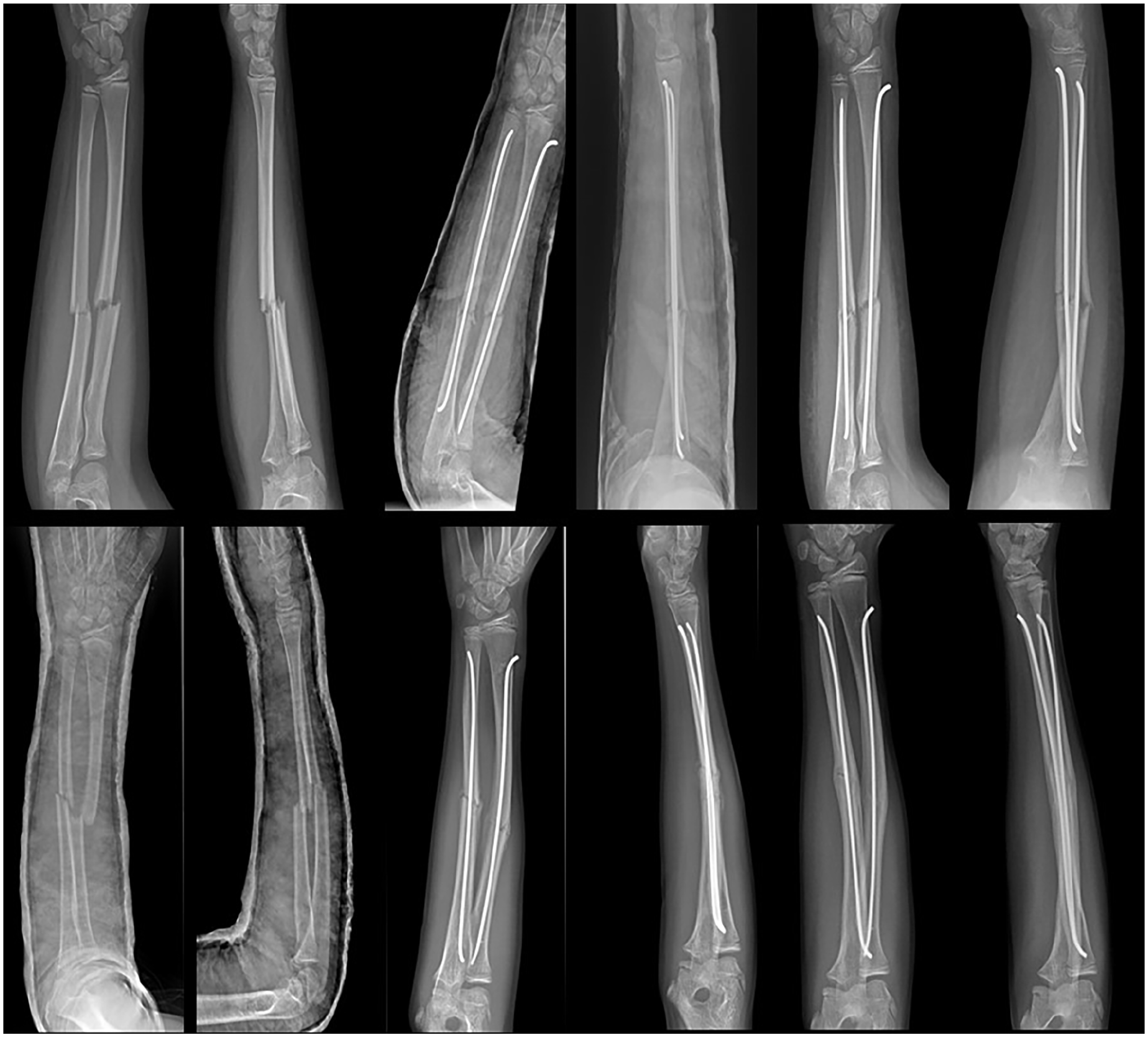
Paired AP radiographs showing fracture healing in two boys aged 12, in three moments: on admission, after 3 weeks, and after 6 weeks. The first row represents a control case, and the second row represents a study case.
Figure 4 illustrates, in a box and whiskers graph, the differences between the two groups regarding the REBORNE score at 3 weeks. The differences between the age- and sex-matched groups were statistically significant (Z-value = −6.64. p-value < 0.05) following a Wilcoxon signed-rank test.
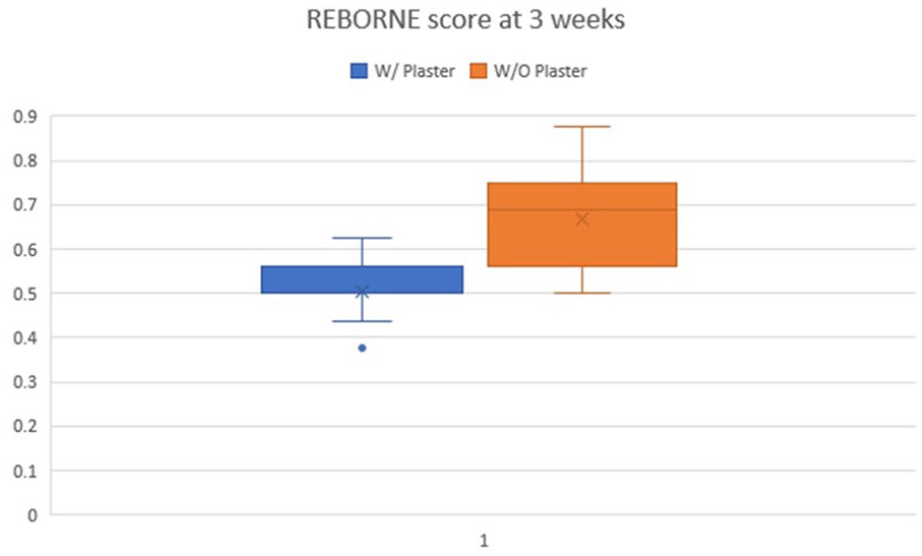
Differences between REBORNE callus scores at 3 weeks postoperative between the study group and the control group.
As shown in Figure 5, representing an age-sex match, the active early motion treatment patients demonstrated superior radiographic healing compared to the control subjects. As illustrated in Figure 5, the callus differences were further maintained at the 6-week postoperative evaluation. Again, the differences were statistically significant using the non-parametric test (Z-value = −6.84, p-value < 0.005; Figure 6).
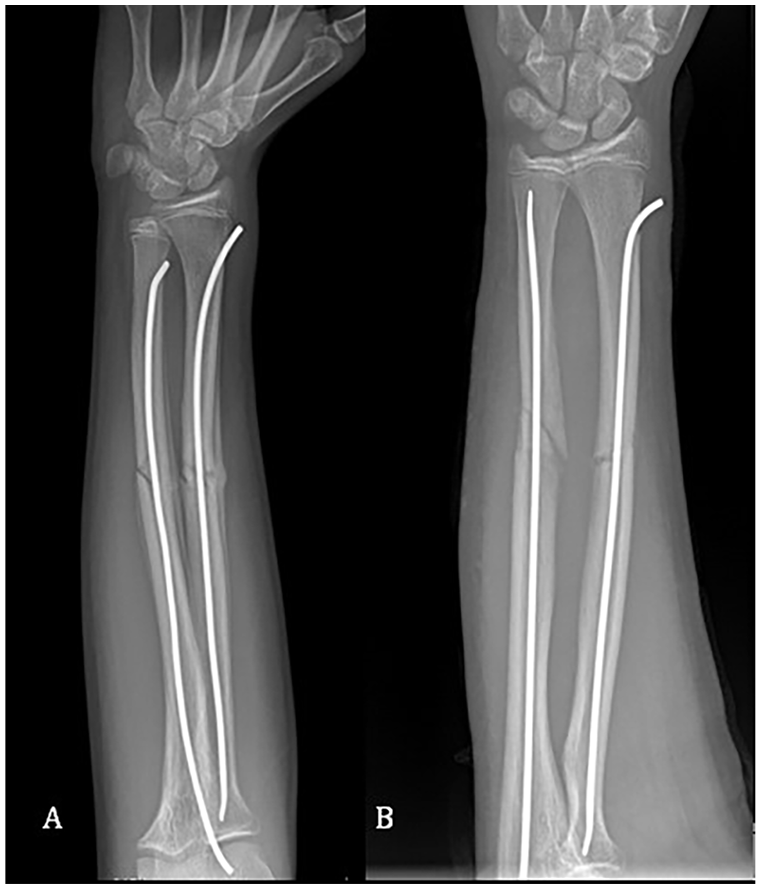
Two 8-year-old girls with left BBFF with AP X-rays at 3 weeks of follow-up. The image on the left (A) corresponds to a patient in the study group, while the image on the right (B) represents a patient in the control group.
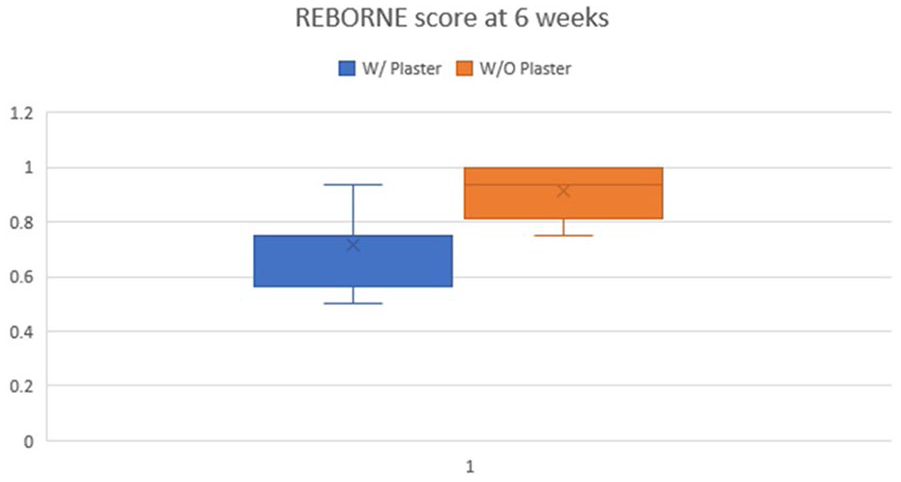
Differences between REBORNE callus scores at 6 weeks postoperative. Both the median values and the margins (whiskers) were notably higher in the study group, suggesting a faster radiological healing time for the patients who did not receive plaster casts.
Figure 7 illustrates an example of callus formation, observed after 6 weeks, in a pair of 10-year-old boys who underwent the same surgical technique.
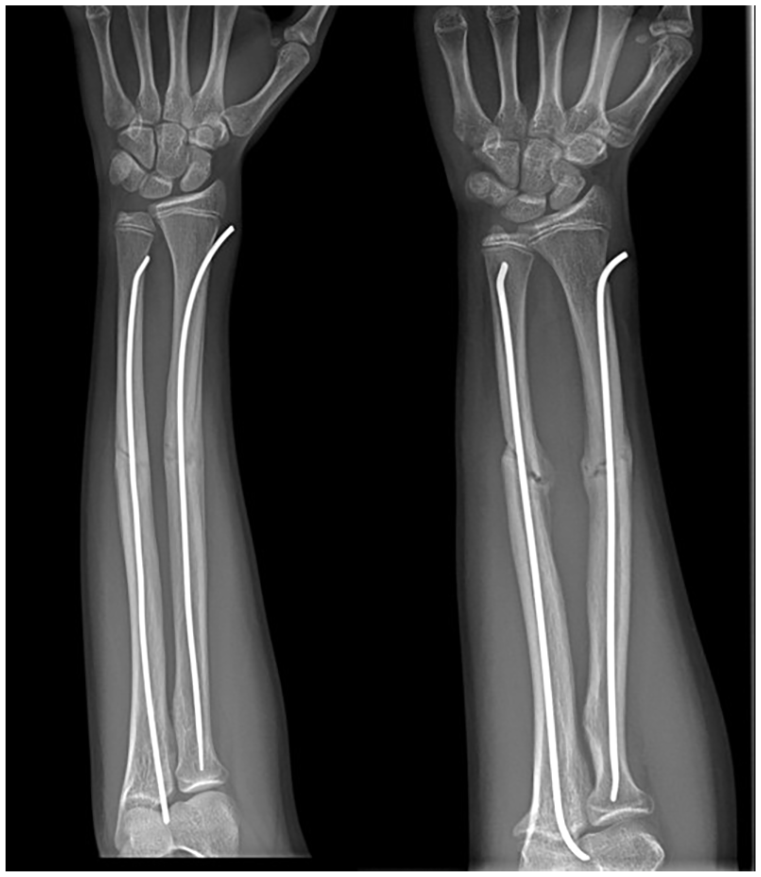
The AP X-rays presented here depict the forearms of two 10-year-old boys with similar bone ages, taken at a 6-week follow-up. The right image shows the patient treated with postoperative casting, while the left image highlights a case with noticeably faster healing compared to the corresponding patient.
PedsQL was performed at 6 weeks for both groups. Upon conducting the Wilcoxon signed-rank test, we obtained a statistically significant difference between the two groups, in favor of the children who did not wear casts (Z-value = −4.36, p-value <0.05). Figure 8 represents the median scores for the two groups.
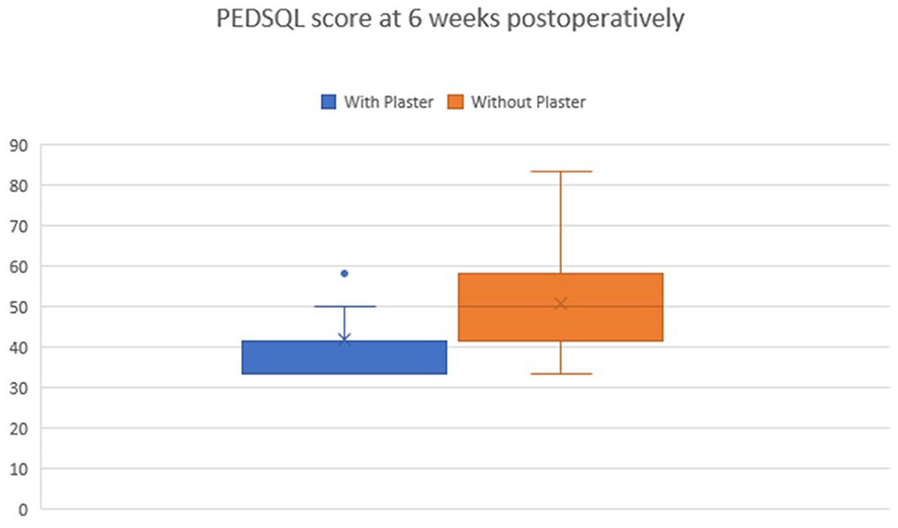
Median PedsQL scores at 6 weeks postoperative. The patients who started early active movement scored a better return to daily activities and tasks at 6 weeks postoperative.
Discussion
ESIN represents the gold standard for treating pediatric forearm fractures. Our study aimed to assess whether forgoing plaster casts may help children return to school and sports faster.
Since 1984, Metaizeau et al. concluded that ESIN has a low complication rate and cast is unnecessary, giving way for early mobilization.15,16 According to their study, osteosynthesis is sufficiently stable, so any complementary immobilization by a cast is unnecessary and also detrimental to the formation of the external callus and its molding by movements of pronosupination. 16 One study involving 173 pediatric patients found that ESIN without post-surgical immobilization achieved good functional outcomes with low complication rates, suggesting that plaster casts may not always be necessary after ESIN. 12 Our findings align with their conclusions regarding both treatment stability and healing time.
Andaloussi et al. noted that although plaster casts provide an extra layer of protection, especially in cases with higher fracture instability, they did not reduce long-term complications such as delayed healing compared to cast-free approaches. 17 We found no complications in our 6-month follow-up and 100% fracture union either for the children treated with postoperative cast for 3 weeks or for the study group. Antabak et al. concluded that an above-elbow splint for 7 days following the surgery helps avoid the risk of loss of reduction. 8 Having included diaphyseal BBFF, we obtained zero incidences of loss of reduction for both groups.
Our study aimed to evaluate the healing speed of pediatric forearm fractures treated with ESIN without plaster cast immobilization, using the REBORNE score and callus formation as assessed through radiographic scoring, and to compare it with an age-sex matched patient pool who received plaster casting for 3 weeks after ESIN.18,19 In addition, we aimed to compare the quality-of-life outcomes between patients treated without casting and those who received postoperative casting. By assessing both objective measures of fracture healing and patient-reported outcomes, we sought to determine whether forgoing plaster immobilization in favor of early mobilization could lead to faster recovery and better overall patient satisfaction without compromising fracture healing quality.
Andaloussi et al. also concluded that although ESIN is minimally invasive, it is still more invasive than orthopedic treatment, and should only be performed when optimal functional outcomes cannot be achieved through closed reduction and casting. 17 On the other hand, Salonen et al. affirmed that conservative treatment alone may lead to poor results in up to 50% of patients and that reduction without fixation frequently leads to limited pronosupination. 20 Our clinic’s experience suggests that same-level diaphyseal BBFF in children over 5 years is associated with an increased risk of iterative fracture and loss of motion (because of inadequate tension in the interosseous membrane) when treated conservatively, and the protocol comprises ESIN. For historical context, it is noteworthy that in 1990, Pierre Lascombes affirmed that ESIN is recommended for children over the age of 10 or when conservative treatment proves insufficient, and confirmed Metaizeau’s opinion that there is no need for postoperative immobilization in his series of 85 children. 16 Ostermann et al. recommend orthopedic treatment for distal and midshaft fractures, and ESIN for proximal forearm fractures. 21 There are authors like Franklin et al., whose work in the search for predictors of conversion from conservative to operative treatment concluded that a fracture is more prone to be operated on if the child is older, has a more proximal ulnar fracture, and more shortened radius fracture. 22 Curiously, Flynn et al. chose to treat BBFF through the fixation of a single bone and rotating the other bone into a reduction. 23
The study’s strengths include its prospective design and the use of age- and sex-matched controls, enhancing the validity and comparability of outcomes between the two samples selected from an adequate population. In addition, it incorporated objective radiographic scoring, such as the REBORNE callus score, and patient-centered outcomes via the PedsQL instrument, providing a comprehensive evaluation of both clinical and quality-of-life impacts.
This study has several limitations. First, it was conducted as a single-center investigation, limiting the generalizability of its findings to populations from different geographical and socioeconomic backgrounds. Although the sample size was sufficient, it may not capture less common outcomes, such as refracture rates or wound infections, particularly among patients treated without casting and those from socioeconomically unstable backgrounds, because we did not register complications in these patient samples. Randomization was performed using an odd-even methodology, which, while effective, may not be as robust as alternative randomization strategies. The research did not include laboratory data on serum vitamin D levels, which are established factors that facilitate bone healing and may account for differences observed among children. 24 Future research is prone to include this topic.
Although existing literature on BBFF is extensive, few studies specifically address the benefits of early mobilization and the omission of plaster casting after ESIN. Our findings indicate that the study group experienced accelerated healing, likely facilitated by micromovements within the elastic stable construct and early active movements of the upper limb. These factors may also support faster improvements in quality of life. Future research is needed to determine conclusively whether forgoing plaster casting in BBFF cases contributes to faster recovery and earlier return to sports.
Conclusions
Our preliminary findings show that ESIN for diaphyseal BBFF can be safely conducted without plaster casting.
Prompt recovery of forearm movements promotes faster healing of the fracture and improves patient satisfaction.
Omitting postoperative casting in pediatric forearm fractures treated with ESIN accelerates healing and may improve functional recovery, without compromising clinical outcomes. Faster mobilization enhances patient satisfaction, making this approach a viable alternative to traditional casting.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521251352323 – Supplemental material for Forearm fractures treated with elastic stable intramedullary nailing: Is casting still necessary?
Supplemental material, sj-pdf-1-cho-10.1177_18632521251352323 for Forearm fractures treated with elastic stable intramedullary nailing: Is casting still necessary? by Alexandru Herdea, Mihai-Codrut Dragomirescu, Mara Tiron and Alexandru Ulici in Journal of Children’s Orthopaedics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.