
Abstract
Purpose:
The aim of the study is to evaluate the use of ultrasound imaging in diagnostics of Monteggia lesion in children where conventional radiographs and the use of the radiocapitellar line fail to provide an accurate diagnosis.
Methods:
Prospective diagnostic study of 70 patients treated between May 2018 and July 2021 in a pediatric level 1 trauma center. In 20 patients with the confirmed radiographic diagnosis of Monteggia lesion, an ultrasound of the humeroradial joint was performed to determine signs of both normal and dislocated elbow joint. In 36 patients with suspected humeroradial dislocation on plain radiographs, ultrasound imaging was performed to determine the definitive diagnosis. Overall, 14 patients with elbow joint injury other than humeroradial dislocation were excluded from the study.
Results:
The “double-hump sign” and the “congruency sign” were determined as normal findings on ultrasound of the humeroradial joint. These signs were applied to patients with unclear findings on radiographs. In three patients, the dislocation of the humeroradial joint was confirmed by ultrasound. In two patients, “defect in congruency sign” was seen during reduction despite normal radiographs, which required re-reduction. In 31 patients, dislocation of the humeroradial joint was refuted. In 34 out of the 36 patients, the diagnosis determined by ultrasound was confirmed in follow-up. Two patients did not attend the follow-up examination.
Conclusion:
Ultrasound imaging is an accessible, non-invasive, and dynamic point-of-care method that can be applied in children suffering from suspected humeroradial dislocation and/or subluxation.
Level of evidence:
Level III—diagnostic study.
Introduction
Monteggia lesion (Monteggia fracture-dislocation) in the pediatric population is a rare and severe injury defined as a fracture of the ulna at any level cojoined with dislocation of the proximal radius in the humeroradial joint. One of the criteria that affect the outcome of the Monteggia lesion is an early and accurate diagnosis of the radial head dislocation. When diagnosed and treated properly, the treatment leads to excellent results with normal functional outcome. If missed, such dislocation leads within weeks to irreversible changes in the humeroradial joint—chronic Monteggia lesion—which requires demanding reconstructive surgery, often with less satisfactory results.
In patients with a suspected injury of the humeroradial joint conventional radiographs of the elbow joint in both lateral and anteroposterior (AP) projection should be performed. The primary tool used to evaluate the alignment of the humeroradial joint is the radiocapitellar line (RCL). Although widely believed that it was proposed by Støren 1 in 1959, we can find the description of RCL by Smith 2 as early as 1947. RCL is defined as a line drawn in the center of and parallel to the long axis of the radius, which should cross the middle of the capitulum of the humerus in both AP and lateral projection. Due to the physiological curvature of the proximal radius, the ongoing discussion revolves around whether this line should be drawn parallel to the long axis of the shaft or the neck of the radius. However, multiple authors suggested that in the lateral projection RCL drawn through the neck has better significance.3,4
Despite regular use of RCL in diagnostics of the dislocation of the proximal radius, it has been proven that in younger children with unfinished ossification of the elbow, RCL misses the capitulum in its middle third or entirely.3–7 This results mainly from the eccentric ossification of the capitulum and limits the use of RCL in assessing the humeroradial joint in younger children. If there is any doubt, a child with suspected dislocation of the proximal radius usually undergoes repeated X-rays and/or manipulation under an X-ray amplifier under general anesthesia to confirm the diagnosis.
New landmarks on conventional radiographs of the elbow have been proposed to increase the accuracy of diagnostics of Monteggia lesion.8,9 Despite that, the need for a simple and accessible new method to improve and confirm the diagnosis is still high. Ultrasound imaging is established in both adult and pediatric traumatology and has the ability to display cartilaginous parts of bones. Although it has been suggested for use in the assessment of the humeroradial joint,10–12 the usage and benefits of this method have not yet been fully researched, and the literature resources are limited to singular case reports.13,14
The aim of this study is to evaluate the use of ultrasound imaging in diagnostics of Monteggia lesion in children where conventional radiographs and the use of RCL fail to provide an accurate diagnosis.
Material and methods
Approval was obtained from the Institutional Ethics Committee, and informed consent was given by all participants of the research and/or their parents.
A diagnostic study was performed on pediatric patients treated in a level 1 pediatric trauma center between May 2018 and July 2021 (3 years). The main inclusion criteria for the study were age 0–18 years and the ability to undergo ultrasound imaging of the elbow joint without the need of general anesthesia. The main exclusion criteria were known severe congenital or posttraumatic deformity of the elbow joint that could alter the sonographic image.
Ultrasound imaging of the elbow joint was performed in 70 patients aged 0–16 years. For the examination, Samsung MedisonTM RS85 with linear probe 3–16 MHz, and Toshiba XarioTM 100 with linear probe 7.2–14 MHz were used to obtain B-mode sonograms. The study was performed by a single experienced pediatric surgeon with no previous sonographic experience after training was provided by an experienced sonographer and radiologist.
Patients in the study were divided into three groups. The first group represented 20 patients with a confirmed Monteggia lesion on the radiograph (7) or patients without injury of the elbow joint (13). In patients with confirmed Monteggia lesion, the ultrasound was performed in general anesthesia both before and after the reduction. Elbow sonographs of these patients were used to determine sonographic signs of normal and dislocated humeroradial joint for further reference. Ultrasound imaging was performed on both elbows for comparison.
The second group represented 36 patients with suspected dislocation in the humeroradial joint. In these patients, RCL partially or entirely missed capitulum on conventional radiographs. In these patients, the ultrasound imaging was performed on both the injured limb and uninjured limb for comparison. Both the definitive diagnosis and choice of the treatment in this group were based on the result of the ultrasound imaging.
The third group comprised of 14 patients with elbow joint injury other than humeroradial dislocation and atypical findings on conventional radiographs (avulsion of the medial epicondyle, fracture and pseudoarthrosis of the proximal radius, fracture of the capitulum of the humerus, and Panner’s disease). These patients were excluded from the evaluation of this study.
The examination was performed in sitting and/or laying patient with the examined limb in semiflexion and supine or neutral position. Images of the humeroradial joint were obtained in the longitudinal axis from the anterior to the lateral and posterolateral aspect of the joint (Figure 1). No sedation and/or analgesia was needed except for patients with previously confirmed humeroradial dislocation on conventional radiographs (i.e. patients from the first group with confirmed Monteggia lesion). These patients required treatment in general anesthesia, and therefore, the ultrasound imaging was performed in the operating theater after the administration of anesthetics.

The technique of ultrasound imaging of the humeroradial joint—longitudinal imaging using a linear probe from anterior (a) to posterolateral (b) aspect of the joint in semiflexion and supination of the forearm.
Results
In the first group (confirmed Monteggia lesion or uninjured elbow) patients were aged 1–13 years (median 6.50, average 7.00) with a sex distribution of 12 boys and 7 girls.
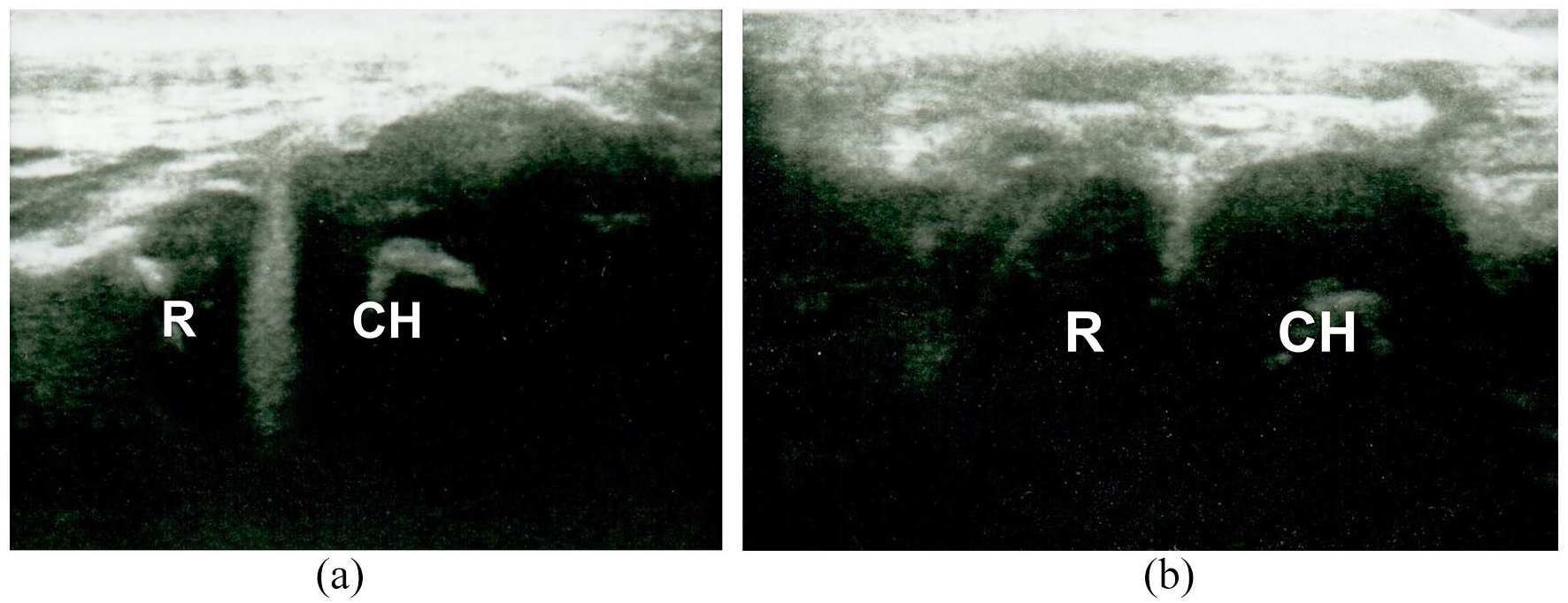
On sonographs of the uninjured elbow, we have determined the correct alignment of the humeroradial joint by the presence of two rounded consequent hypoechoic elevations of the same height, representing the radial head and capitulum cartilages. We termed this “double-hump sign” (Figure 2(a)). This sign is most expressed in the supinated forearm, while in pronation, radius elevation can impose to be above the capitulum, which can distort the result of the examination (Figure 2(b)).
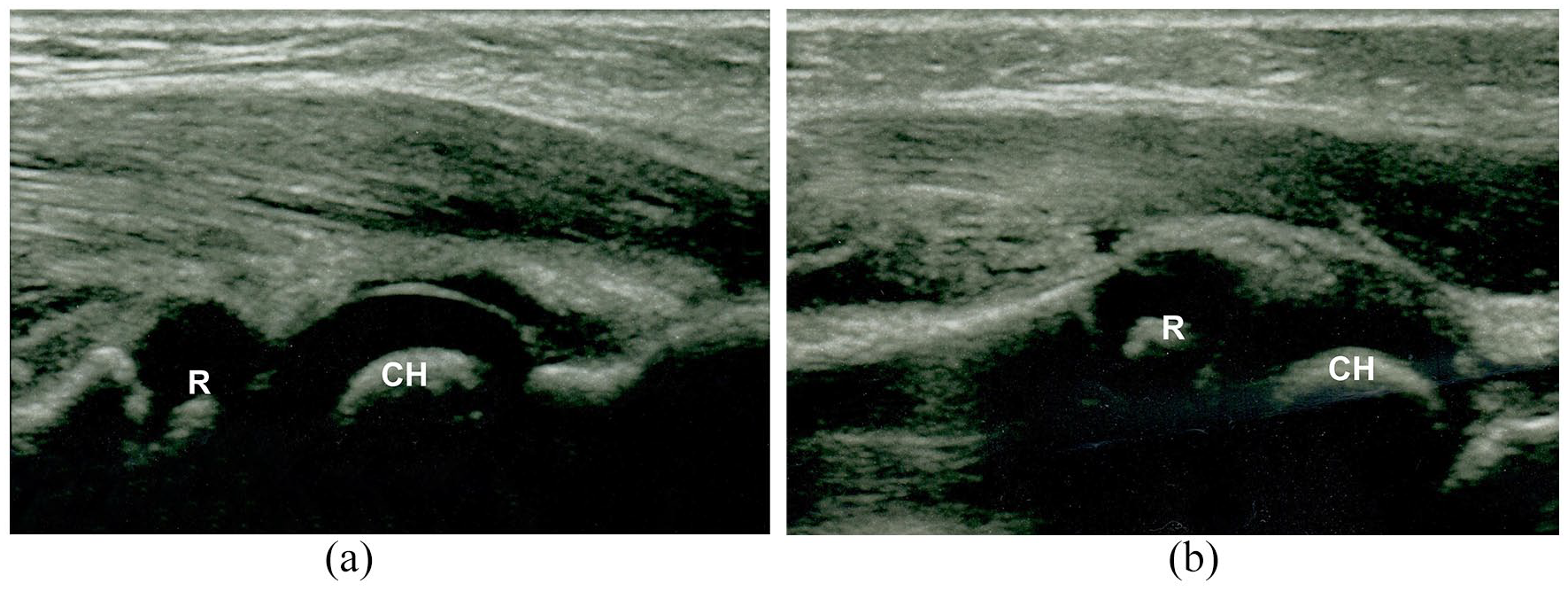
“Double-hump sign”—two consequent hypoechoic elevations of the radial head (R) and capitulum of the humerus (CH)—in supination (a) and pronation (b) of the forearm.
The second sign of the correct alignment of the humeroradial joint is corresponding articular surfaces of the radius (concave) and the humerus (convex). We termed this “congruency sign” (Figure 3). This sign is usually expressed in posterolateral projection, where the small wedge of synovial plica on the periphery of the joint can also be seen. The “congruency sign” is more pronounced in the injured elbow, where ultrasound can reach between articular surfaces due to increment of the intraarticular fluid (usually hemarthrosis) and synovial plica is accentuated due to bleeding.
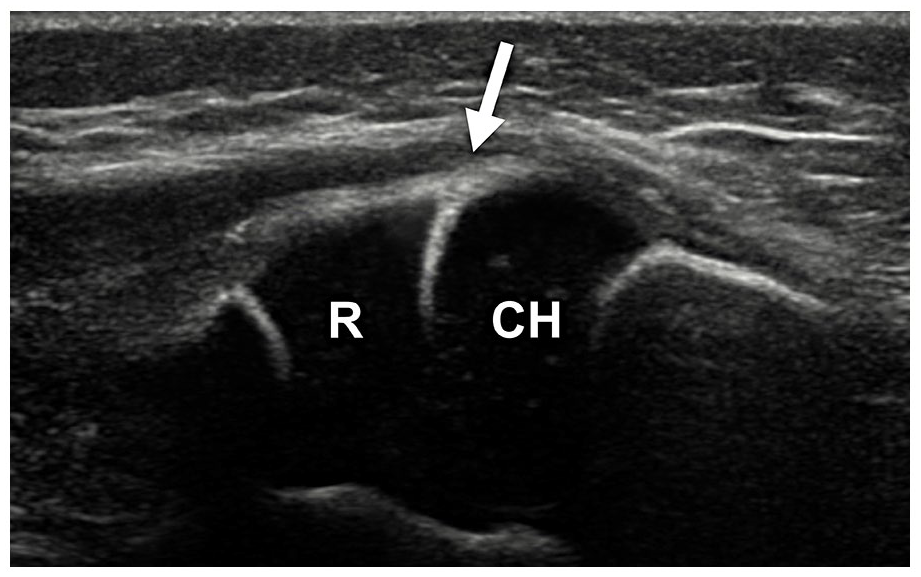
“Congruency sign”—an arrow pointing between the concave articular surface of radius (R) and convex articular surface of the capitulum of the humerus (CH).
In patients with dislocation or subluxation of the proximal radius, “double-hump sign” and/or “congruency sign” is not present, radial and humeral elevations do not correspond, and they are usually displayed in different projections (Figure 4).
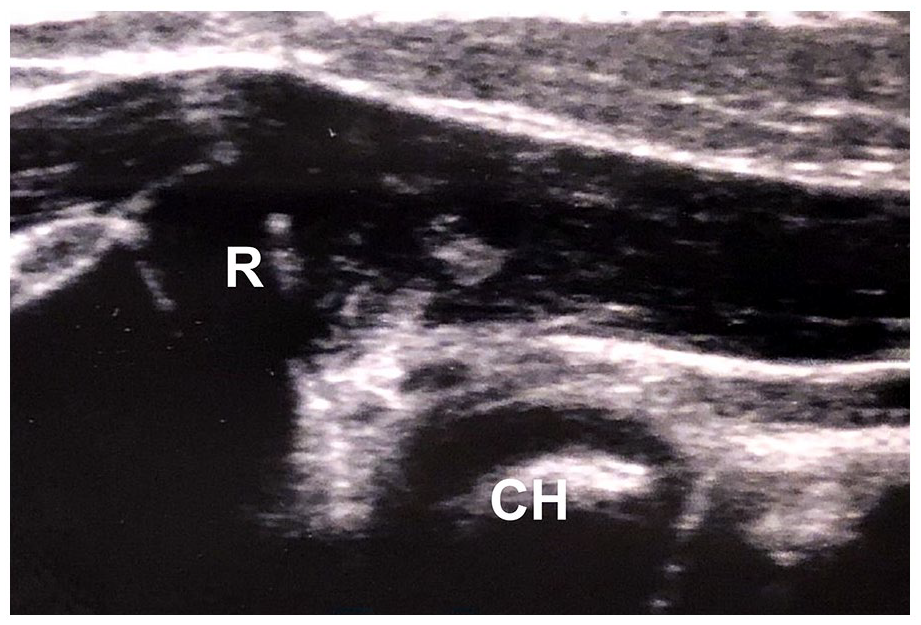
Ultrasound image of dislocation in the humeroradial joint—head of the radius (R) is completely missing capitulum of the humerus (CH).
In the second group (suspected dislocation in the humeroradial joint), patients were aged 0–16 years (median 6.00, average 6.08) with an even sex distribution of 18 boys and 18 girls.
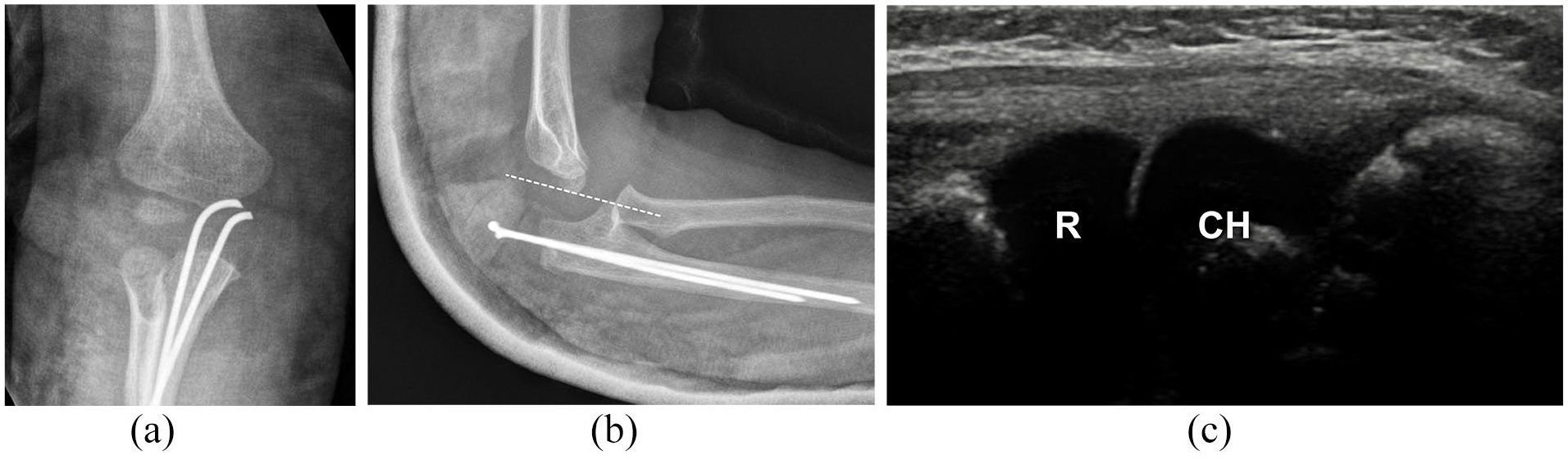
In total, 14 patients from the second group had a solitary fracture of the ulna, which is a rare injury often cojoined with dislocation of the proximal radius. This fracture pattern represents the highest risk factor for the presence of a Monteggia lesion. These patients all had normal findings on sonographs, and Monteggia lesion was not confirmed in any (Figure 5).
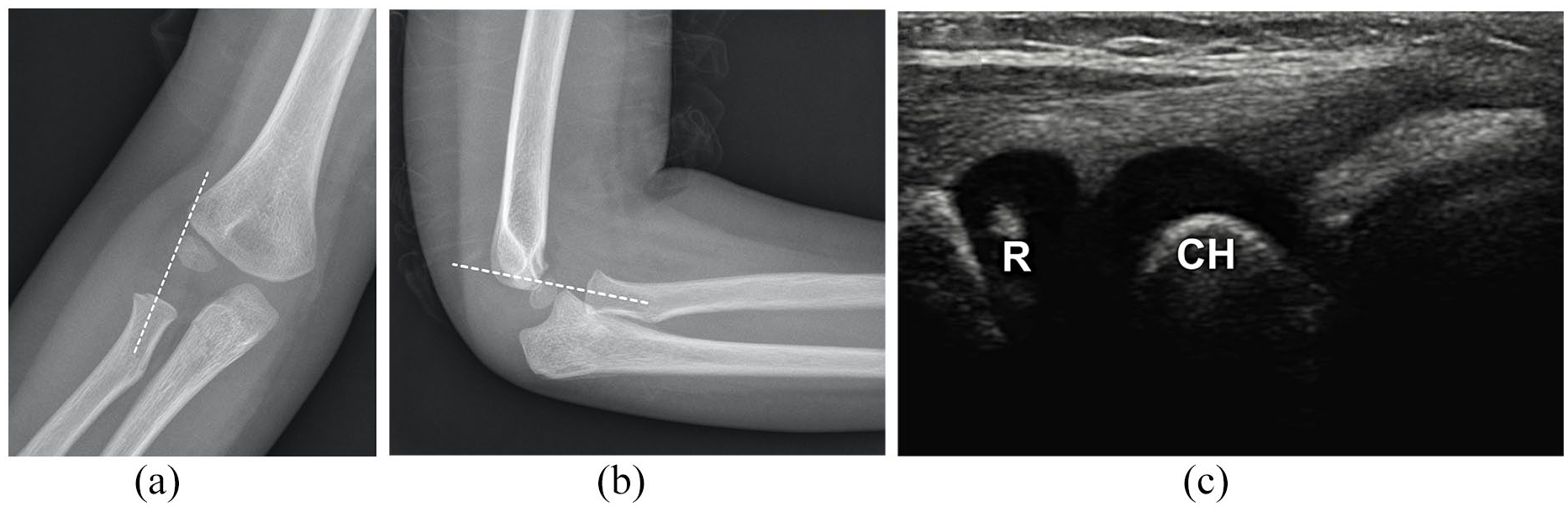
Boy, 6 years old, with fracture of the proximal ulna. RCL drawn through the neck of the radius misses capitulum in both AP (a) and lateral (b) projection. (c) Ultrasound imaging showing good congruence of the radial head (R) and capitulum of the humerus (CH).
Six patients from the second group sustained an elbow joint injury other than ulnar fracture (i.e. proximal radius and/or distal humerus) with suspected cojoined dislocation in the humeroradial joint on conventional radiographs. Using ultrasound imaging, dislocation was not confirmed in any of these patients.
Nine patients from the second group had suspected redislocation after the treatment of the Monteggia lesion on radiographs after the surgery (either simple reduction or osteosynthesis). Eight of these patients had normal ultrasound findings (Figure 6), and one patient was indicated for re-reduction due to confirmed subluxation of the proximal radius on ultrasound.
Girl, 21 months old, after osteosynthesis for Monteggia lesion type Bado 2 (a-b) with suspected persistent dislocation of proximal radius in lateral projection. Ultrasound imaging showing good congruence of the radial head (R) and capitulum of the humerus (CH) with both “double-hump sign” and “congruency sign” (c).
One patient from the second group had undergone reconstructive surgery for the chronic Monteggia lesion and had suspected subluxation 1 month after the surgery. This subluxation was confirmed with ultrasound imaging.
Two patients from the second group had confirmed Monteggia lesion but met the criteria for the second group for distinctive ultrasound findings during the reduction in general anesthesia. Peroperative radiographs in these patients showed sufficient reduction, but we have seen a defect in the “congruency sign” on the ultrasound, which indicated persisting subluxation of the proximal radius. After following repeated reduction, both the “double-hump sign” and “congruency sign” appeared on ultrasound as a sign of both successful treatment and physiological alignment of the humeroradial joint (Figure 7).
Boy, 4 years old, after reduction of Monteggia lesion—confirmed by X-ray—with both radius (R) and capitulum (CH) showing concave articular surfaces as “defect in congruency sign” (a) and normal image of both “double-hump sign” and “congruency sign” after re-reduction (b).
Three patients from the second group had suspected congenital subluxation of the proximal radius. In one of these patients, the congenital subluxation has been confirmed on sonographs, while in the other two, it has been refuted.
One patient from the second group sustained a traumatic brachial plexus lesion during delivery with suspected dislocation in the humeroradial joint. The ultrasound has not confirmed dislocation in this patient.
Overall, 34 of 36 patients from the second group were followed up for 1–16 months (average 4.2 months, median 2 months) to confirm the diagnosis. In all these patients, the diagnosis made by ultrasound has been confirmed. Two patients with suspected congenital subluxation (one confirmed and one refuted) did not attend the check-up appointment.
Discussion
Although RCL is commonly used for assessing the alignment of the humeroradial joint, it has been challenged multiple times. Studies proved that in children with not fully ossified elbow joint, RCL misses capitulum in its middle third in up to 80% of cases and entirely in up to 17% of cases.4–7 These studies also proved that RCL drawn through the neck of the radius is more accurate than the line drawn through the shaft.3,4 This accentuates in younger children, which has been proven in this study, as only four of our patients from the group with suspected dislocation of the humeroradial joint were older than 10 years, and half of them (18) were younger than 6 years. These children are most prone to false diagnosis of Monteggia lesion.
Alternative landmarks on conventional radiographs have been suggested to improve the accuracy of diagnostics of humeroradial dislocations. Wang and Su 9 suggested P-line crossing the middle of the proximal and distal radial physes, and Souder et al. 8 suggested a lateral humeral line drawn along the lateral edge of the ossified condyle parallel to the long axis of the humeral shaft. Although P-line has significantly better results in the evaluation of the humeroradial joint, it still passes the center of the capitulum in only 88.23% of patients on AP view and in 72.50% on the lateral view. It also requires a radiograph of the whole forearm, which is not usually taken when assessing the elbow joint. The lateral humeral line is suitable only for AP projection and lateral dislocation of the proximal radius (Monteggia lesion type Bado 3). It also requires precise AP projection, which can be challenging in younger children with an acute elbow injury.
Even with referred landmarks, the need of an alternative method for assessing the humeroradial joint is high. Literature mentions the use of computed tomography (CT), magnetic resonance imaging (MRI), arthrography (AG), as well as the possibility of ultrasound imaging.10–13 However, these methods are rarely used for their disadvantages. CT is limited by an excessive amount of radiation. MRI represents an expensive, time-consuming method that requires sedation of younger children. AG represents an invasive method that also requires sedation. Sonography, on the other hand, is a widely available and accessible point-of-care method that does not require sedation of a child. Yet it is operator dependent, and it is believed that it requires familiarity with ultrasound of the pediatric elbow to assess humeroradial joint dislocations correctly. For this lack of experience, ultrasound imaging is not commonly used in diagnostics of Monteggia lesion.
Ultrasound of the elbow joint is widely discussed in literature. Most articles focus on diagnostics of the supracondylar fracture of the distal humerus in children.15,16 Others focus on soft-tissue injuries, occult fractures, and intraarticular free bodies.10,12 Regarding humeroradial joint in children, the literature mainly deals with the diagnosis of pulled elbow.17,18 Although many articles mention the possible use of ultrasound imaging in Monteggia lesion, we have found only two singular case reports of ultrasound in patients with suspected humeroradial dislocation—one with ultrasound-confirmed 14 and one with ultrasound-refuted diagnosis. 13 Our study is the first to present a larger cohort of patients with suspected Monteggia lesion assessed with ultrasound imaging. In the follow-up, we were able to confirm our ultrasonographic diagnosis in all patients.
The ultrasound imaging technique of the elbow is well described in multiple sources.10–12 In compliance with existing literature, we found the linear probe best for the examination of the humeroradial joint. Although the sources describe the humeroradial joint mainly from the anterior aspect of the extended elbow, for the Monteggia lesion, it is necessary to examine both the anterior and (postero) lateral aspect of the joint. We also found semiflexion of the elbow to be more suitable for the examination, with emphasis on supine or neutral position.
We have described two signs of the correct alignment of the humeroradial joint in our patients—the “double-hump sign” and the “congruency sign.” Although a normal ultrasound image of the humeroradial joint can be commonly found in existing literature,10–12 the “congruency sign” has not been mentioned before. While it can be challenging to display in joints without hemarthrosis, we consider it more important if the “defect in congruency sign” is visible than the presence of the “congruency sign” itself. Therefore, it is important that the ultrasound operator thoroughly examines the whole humeroradial joint from its anterior to posterolateral aspect to search for the eventual “defect in congruency sign.” We also consider it crucial to compare ultrasound image of the injured and uninjured elbow in the same patient.
In our study, we had two patients with “defect in congruency sign” during the reduction in general anesthesia despite normal radiographs. After repeated reduction, the success of the treatment has been confirmed with ultrasound. This has never been published before. However, Lee et al. 18 have published an ultrasound study of the pulled elbow, which demonstrated a similar image of entrapped anular ligament and enlarged synovial fringe. Our study suggests that ultrasound imaging can be performed in patients with Monteggia lesion during reduction to prevent this persisting pulled-elbow-like subluxation which is not visible on plain radiographs. The importance of these peroperative findings should be investigated further.
In the third group of patients who were excluded from the evaluation of this study, we found more diagnoses (e.g. avulsion of the medial epicondyle of the humerus) where ultrasound could improve the diagnostics. Further research on a larger cohort of patients should be done regarding these diagnoses.
Our study indicates that the use of point-of-care ultrasound can be the ideal auxiliary method for assessing the humeroradial joint in children with a not fully ossified elbow. This method can significantly reduce radiation dose from repeated radiographs and/or the need of manipulation in general anesthesia in children suffering from suspected humeroradial dislocation.
The limitations of our study are a relatively small cohort of patients with suspected Monteggia lesion and the fact that the ultrasound imaging has been performed by a single operator. However, such a cohort of patients has not been presented before.
The strength of our study is its prospective setup and the follow-up procedure that confirmed ultrasound findings.
Conclusion
Ultrasound imaging is an accessible, non-invasive and dynamic point-of-care method that can be applied in children suffering from suspected humeroradial dislocation and/or subluxation. We also suggest that ultrasound can be used as an auxiliary method in addition to conventional radiographs during the reduction of Monteggia lesion to refute persisting subluxation.
Footnotes
Author contributions
Martin Čepelík: Study design, performed ultrasound imaging examination, data analysis (radiographs and ultrasound images), wrote the article.
Jan Hendych: Data analysis (radiographs), wrote the article.
Hana Melínová: Ultrasound imaging tutor, ultrasound imaging supervision, data analysis (ultrasound images), commented the article.
Petr Havránek: Study design, commented the article.
Tomáš Pešl: Study design, commented the article, senior author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The work has been approved by the Institutional Ethics Committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Health, Czech Republic—conceptual development of research organization (Thomayer Hospital—TH, 00064190).
Informed consent
Informed consent was given by all participants of the research and/or their parents.