
Abstract
Abstract
Purpose
The aim of the study is to evaluate our group of paediatric patients with Monteggia lesion and its equivalents and to compare the characteristics of basic types of these lesions concerning therapeutic approach and results of the treatment.
Methods
Retrospective study of 111 children treated in the Department of Pediatric and Trauma Surgery of the Thomayer Hospital in Prague between 2001 and 2013 (13 years). When evaluating the outcome of the therapy, Bruce's criteria modified by Letts that assesses range of movement, pain and deformity of the elbow joint were applied. Regarding the therapeutic approach, four groups were compared: nonoperative treatment, reduction and casting, closed reduction and internal fixation (CRIF) and opened reduction and internal fixation (ORIF). Results were compared between three groups of patients (Monteggia lesions, displaced equivalents and non-displaced equivalents) using Fisher's exact test with α set to 0.05.
Results
In all, 46 patients were treated for (true) Monteggia lesion, 27 for non-displaced Monteggia equivalent and 38 for displaced equivalent. There is a statistically significant difference in therapeutic approach between all three groups of patients. There is no significant difference in outcome between Monteggia lesions and both types of Monteggia equivalents, but there is a statistically significant difference between displaced and non-displaced equivalents.
Conclusion
There are only two lesions that meet the criteria of Monteggia – (true) Monteggia lesion and displaced Monteggia equivalent. The non-displaced equivalent does not meet the criteria of Monteggia and, therefore, should not be termed a Monteggia equivalent.
Level of Evidence
Level III – Retrospective comparative study
Introduction
Monteggia lesion (Monteggia fracture-dislocation) is a rare and severe injury of both the paediatric and adult forearm and elbow. It was described for the first time by Giovanni Battista Monteggia in 1814, who reported two cases of fracture of the proximal third of the ulna with conjoint ventral dislocation of the proximal radius. 1 Then, 40 years later Joseph Francois Malgaigne stated that fracture of ulna at any level can be joined with ventral dislocation of the proximal radius and warned that with any fracture of the ulna, dislocation of the radial head must be considered. 1 In 1967 José Luis Bado published a classification scheme of Monteggia lesion based on the direction of the dislocation of the radial head. 2 This anatomical classification was suitable for both adults and children. Bado described four basic types of Monteggia lesion and a group of lesions with similar characteristics, which he termed Monteggia equivalents. Most of these equivalents he described as equivalents of type 1 of the Monteggia lesion. This heterogeneous group of Monteggia equivalents contained many lesions that are rarely typical for the growing skeleton or that are not comparable in severity and treatment approach with Monteggia lesions (e.g. pulled elbow syndrome) and, therefore, tendencies for revision of Bado's classification appeared. Olney and Menelaus 3 confirmed the applicability of Bado's classification for the growing skeleton and they created the paediatric modification of Bado's classification of Monteggia equivalents. In addition to these anatomical classifications there are also attempts to create classifications with emphasis on the predilection of the therapeutic approach based on fracture pattern of both the ulna and radius. One of the most comprehensive is the classification of Pešl and Havránek4,5 created in 2005. Although the definition of the Monteggia lesion is clear and widely accepted using Bado's criteria and classification, controversy remains about definition and classification of Monteggia equivalents.
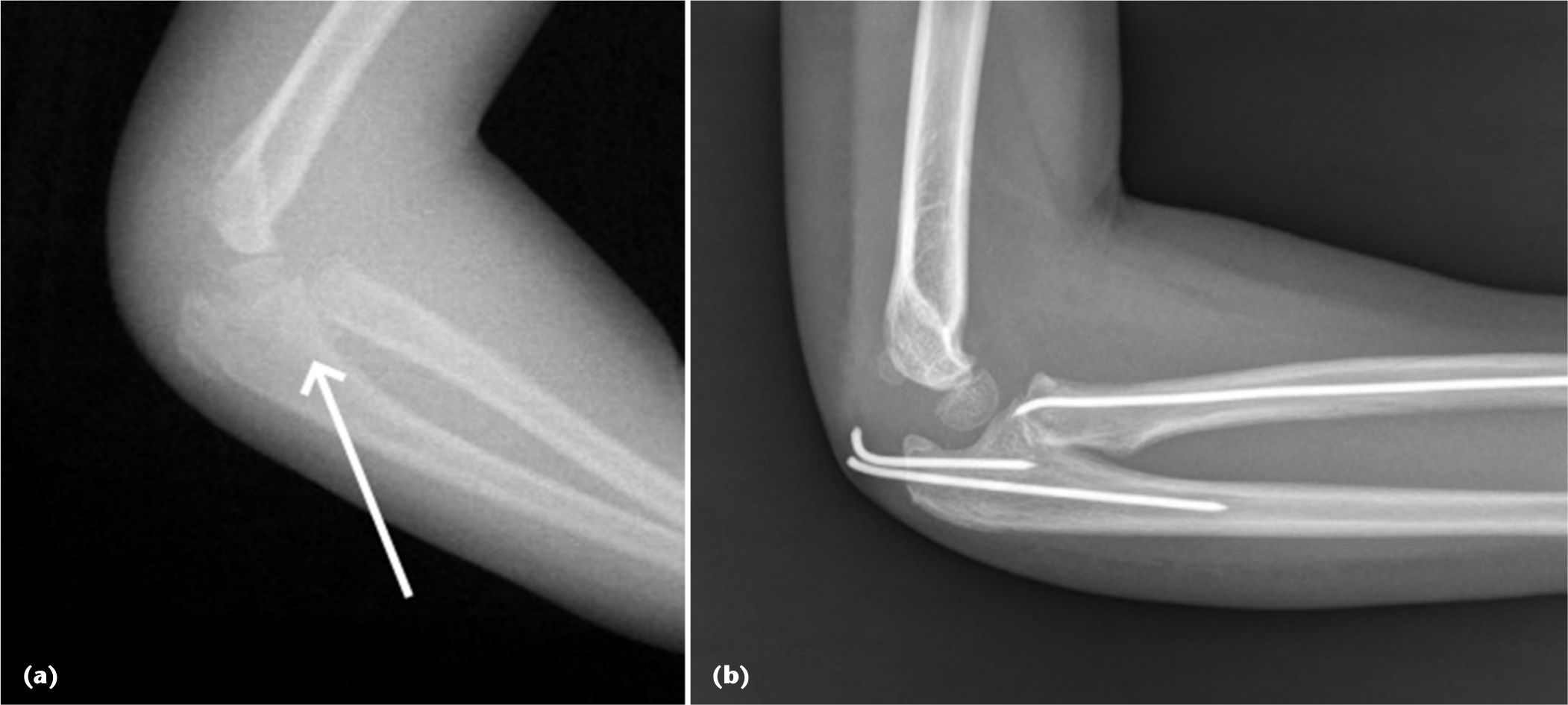
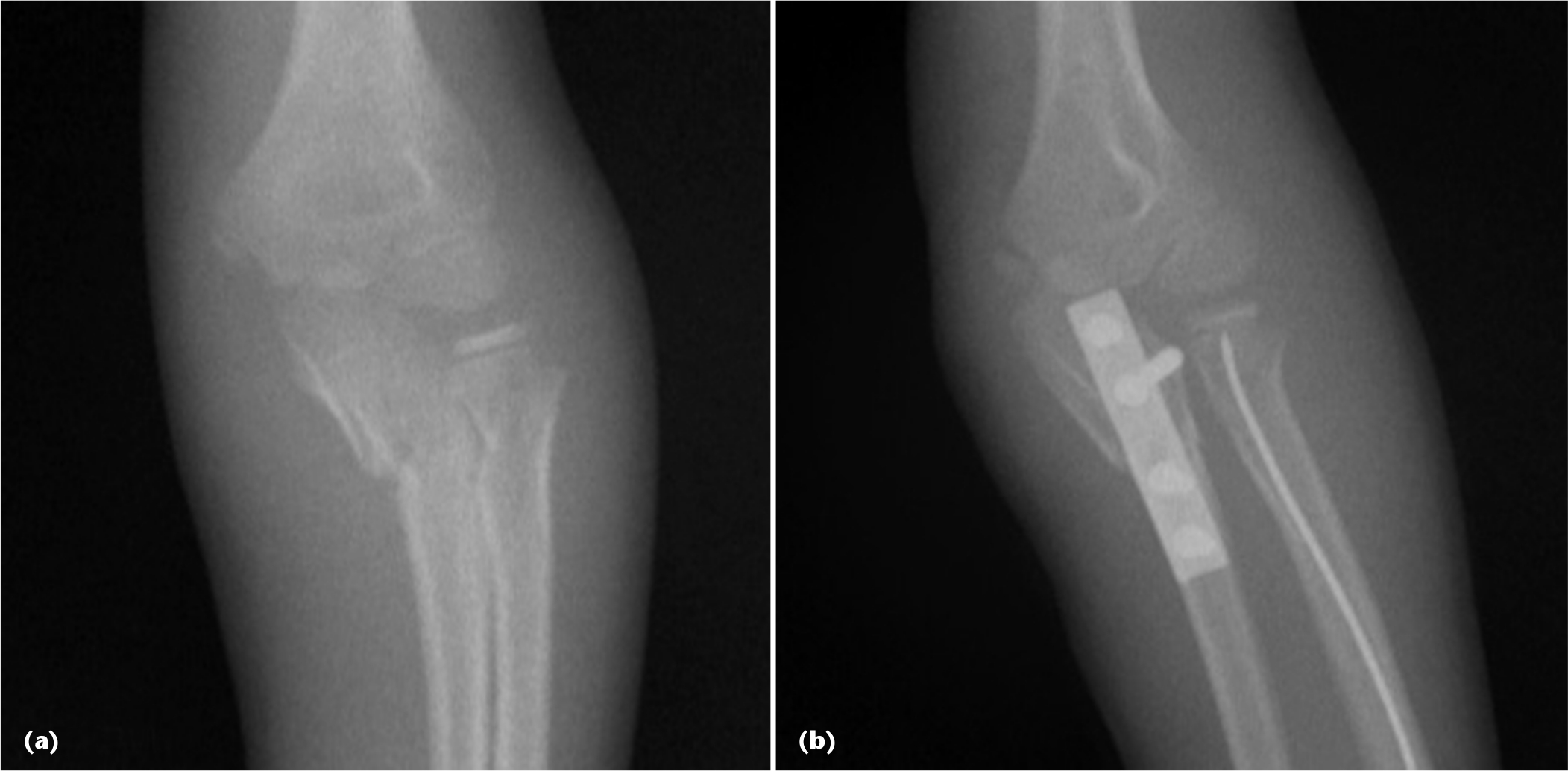
The aim of this study is to evaluate a group of paediatric patients with Monteggia lesion (Fig. 1) and its equivalents and to compare characteristics of basic types of these lesions concerning therapeutic approach and results of the treatment. In our study, we want to find shared and distinct attributes of both Monteggia lesions and Monteggia equivalents and to propose a new, streamlined classification scheme based on the therapeutic approach and results. The premise of the study is that Monteggia equivalents are a standalone diagnostic unit which has its specific diagnostic as well as therapeutic aspects and that this group can also be divided into two very unequal groups – displaced and non-displaced Monteggia equivalent, which differ in the degree of displacement of the proximal radius (Figs 2 and 3).
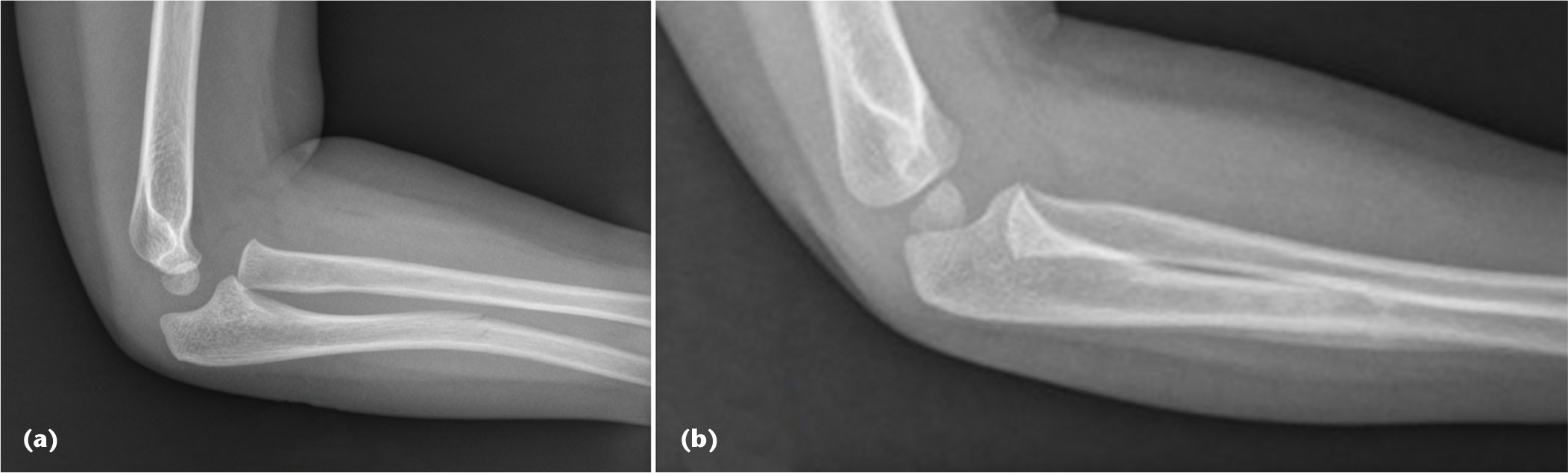
Greenstick fracture of the diaphysis of the ulna with ventral dislocation of the head of the radius - Monteggia lesion Bado type 1, treated with reduction and casting for four weeks. Injury radiograph (
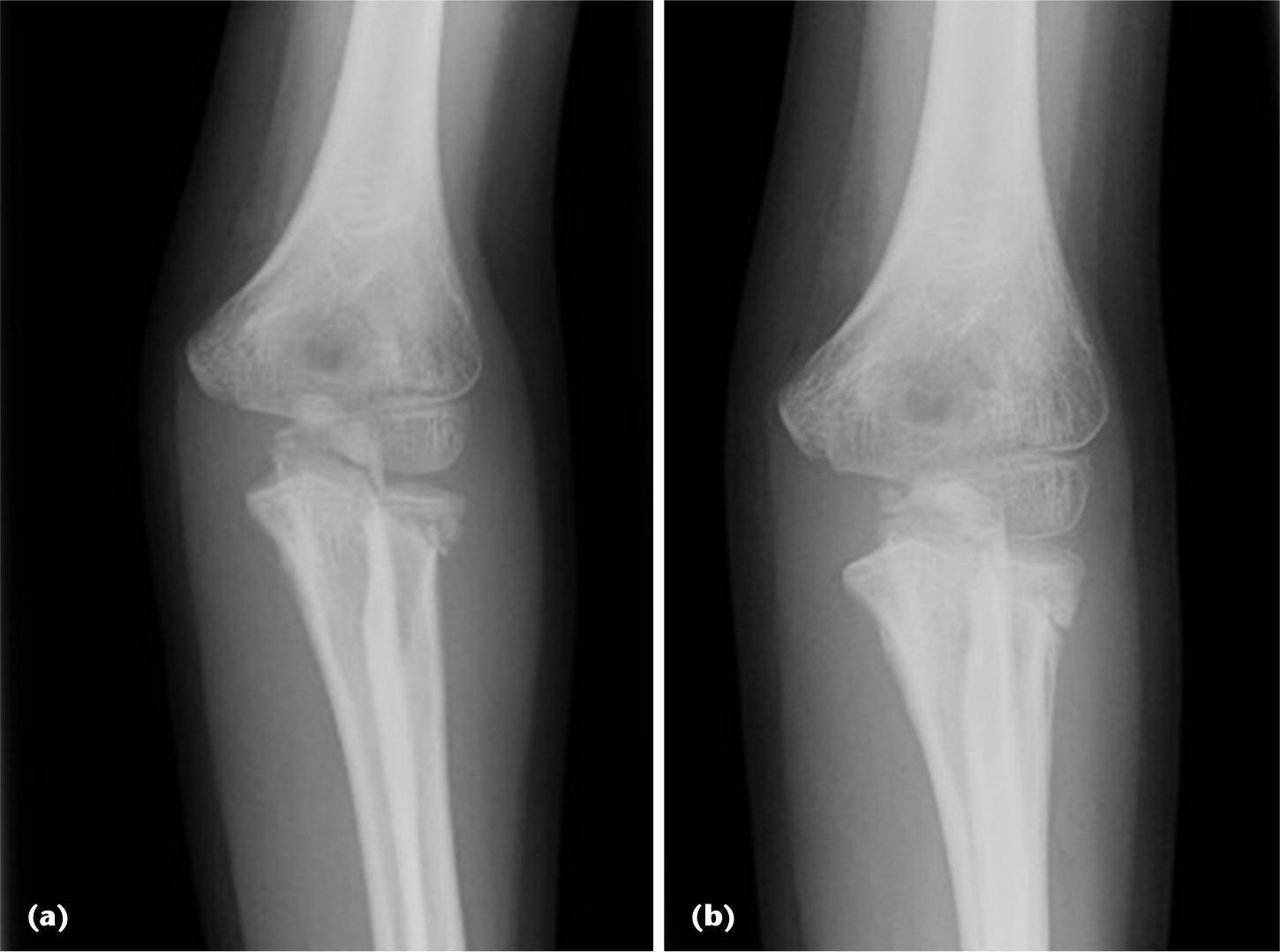
Non-displaced Monteggia equivalent (fracture of the olecranon and physeal injury of the proximal radius) – assessed by the degree of displacement of the proximal radius. Treated with simple casting only. Injury radiograph (
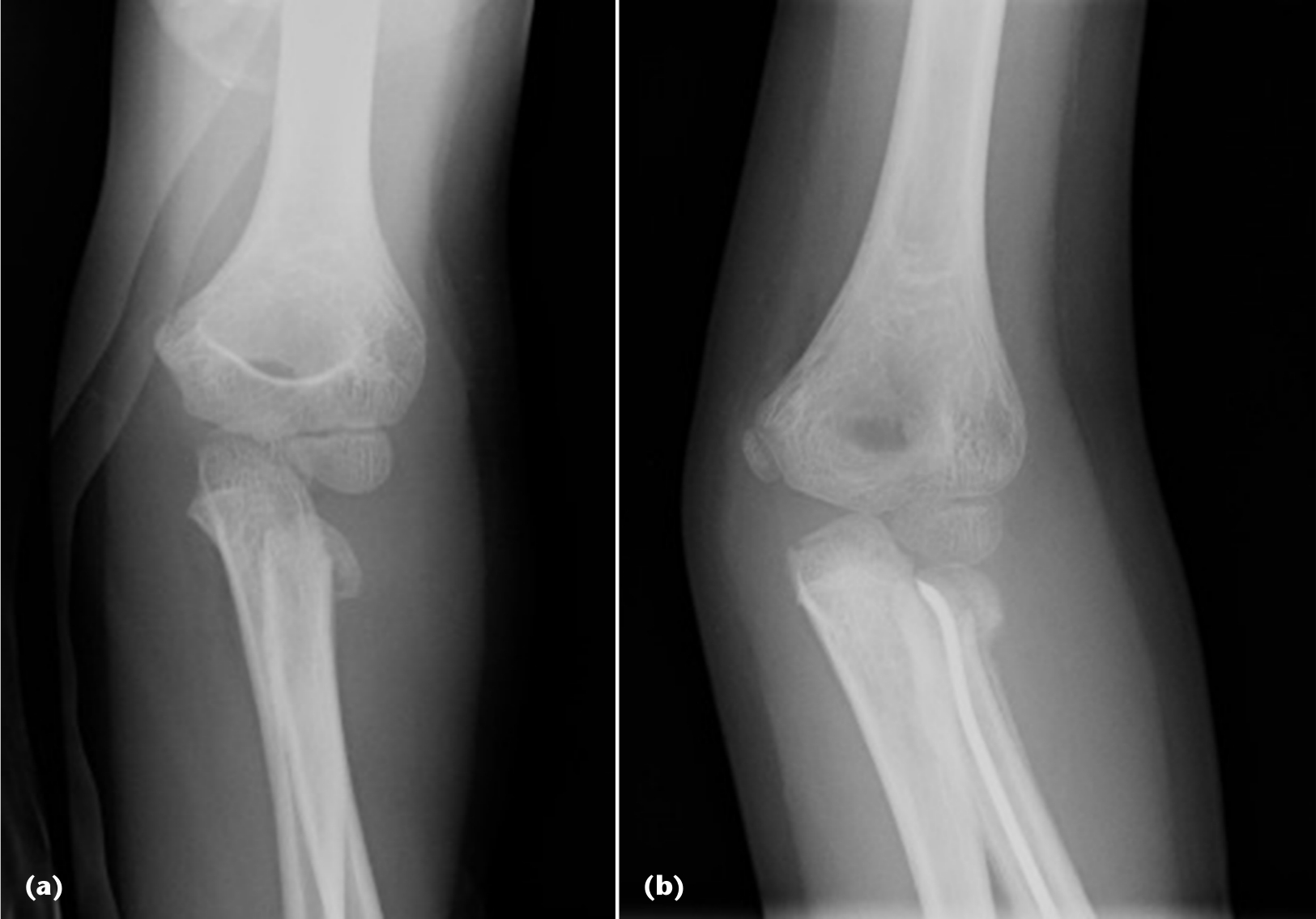
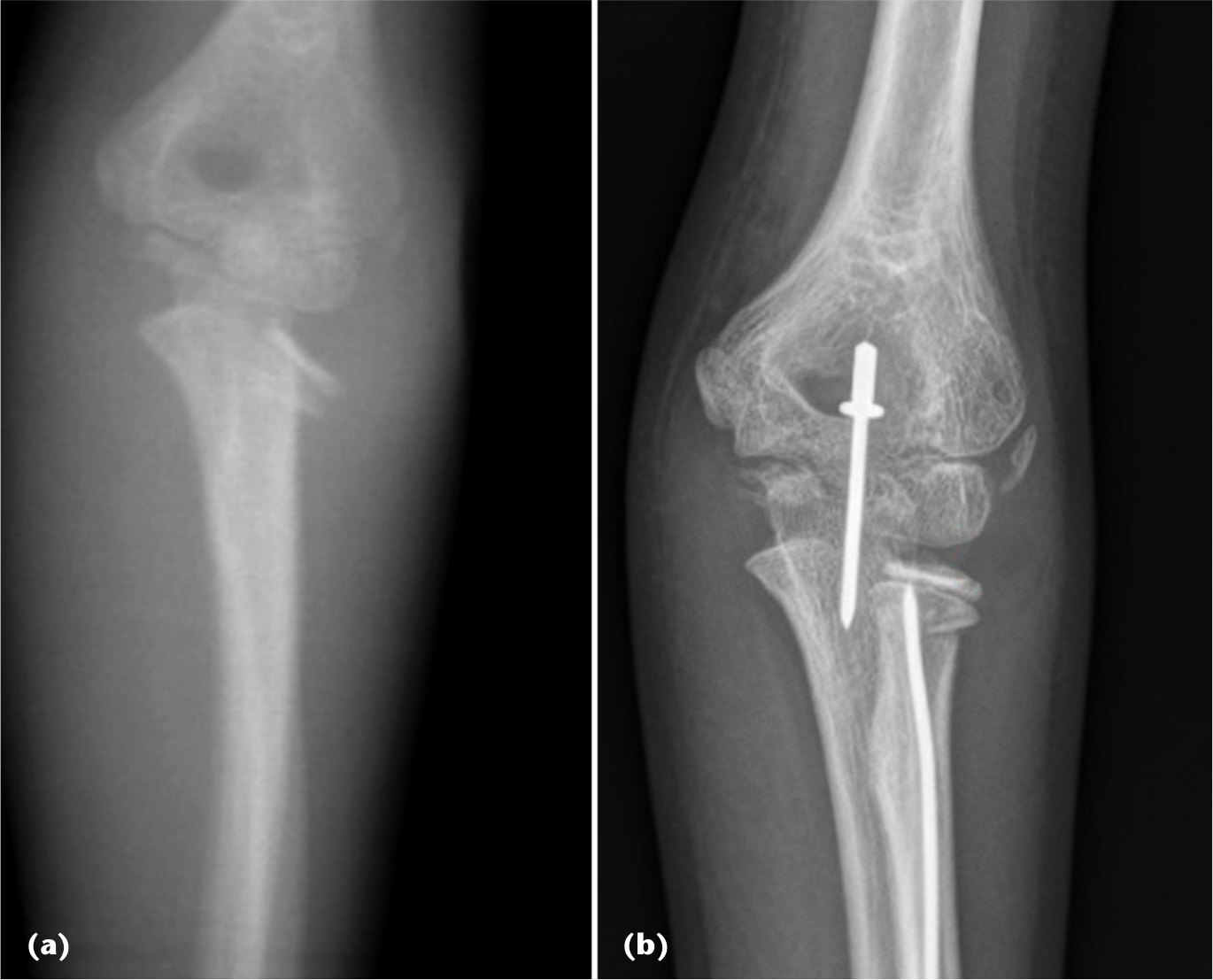
Displaced Monteggia equivalent (non-displaced fracture of the olecranon and displaced physeal injury of the proximal radius) – assessed by the degree of displacement of the proximal radius. Treated with closed reduction and internal fixation of the proximal radius using Métaizeau's technique. Injury radiograph (
Materials and methods
A retrospective study was performed on paediatric patients treated in the Department of Pediatric and Trauma Surgery of the Thomayer Hospital in Prague (level 1 paediatric trauma centre) between 1 January 2001 and 31 December 2013 (13 years). In this period, we treated 136 patients with a Monteggia lesion or its equivalent. From this group we excluded 15 patients with a chronic Monteggia lesion and ten patients that have not been followed in our department. In the remaining 111 children, we evaluated the patient age, level of the fracture of ulna, dislocation or fracture pattern of the proximal radius, therapeutic approach and its outcome.
Emphasis was put on comparison of therapeutic approach and its outcome in three different groups of our patients – with (true) Monteggia lesion, with displaced Monteggia equivalent and with non-displaced Monteggia equivalent.
For Monteggia lesions, we used Bado's definition and classification. 2 For Monteggia equivalents we used a reduced definition of Olney and Menelaus 3 and considered only fractures of the ulna at any level conjoined with fracture of the neck or physeal injury of the proximal radius. For displaced Monteggia equivalents we assessed all injuries of the proximal radius with displacement higher than the first degree of Judets’ classification 6 (≥ 1° of displacement ad axim).
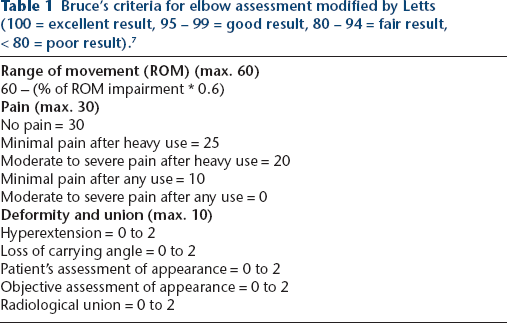
When evaluating the outcome of the therapy, we applied Bruce's criteria modified by Letts 7 (Table 1) that assesses range of movement, pain and deformity of the elbow joint. A perfect score of 100 was classified as an excellent result, 95 to 99 as good, 80 to 94 as fair and < 80 as a poor result.
Bruce's criteria for elbow assessment modified by Letts (100 = excellent result, 95 – 99 = good result, 80 – 94 = fair result, < 80 = poor result). 7
Regarding therapeutic approach, we divided patients into four groups – nonoperative treatment (simple casting only), reduction (in general anaesthesia) and casting, closed reduction and internal fixation (CRIF) and opened reduction and internal fixation (ORIF).
We compared both therapeutic approach and outcome between our three groups of patients (Monteggia lesions, displaced equivalents and non-displaced equivalents) using Fisher's exact test with α set to 0.05.
Results
Between 2001 and 2013 we treated 111 paediatric patients with a mean age of 6.7 years (11 months to 18 years) and the peak incidence between the third and 8th year of age. The gender ratio was balanced with 53 girls and 58 boys. In all, 46 of our patients were treated for (true) Monteggia lesion, 27 for non-displaced Monteggia equivalent and 38 for displaced equivalent. Regarding Monteggia lesions, 28 patients had Bado type 1, one patient type 2, 16 patients type 3 and one patient type 4.
Concerning the fracture pattern of the ulna in Monteggia lesion, the most frequent was fracture of the proximal third of the ulna in 18 patients (39% of Monteggia lesions), closely followed by fracture of the middle part of the diaphysis of ulna in 17 patients (37% of Monteggia lesions) and olecranon (both intraarticular and physeal injury) in 11 patients (24% of Monteggia lesions). There was, however, a difference in ulnar fracture pattern between type 1 and type 3 Monteggia lesion with the majority of diaphyseal fractures in type 1 (16, i.e. 57%) and fractures of the proximal third of the ulna in type 3 (11, i.e. 69%). In Monteggia equivalents, the most typical pattern was a fracture of the olecranon in both displaced (26, i.e. 72%) and non-displaced lesions (14, i.e. 52%).
The dominant fracture pattern of the proximal radius in Monteggia equivalents was separation of the proximal epiphysis of radius of Salter-Harris type II in both displaced (36, i.e. 95%) and non-displaced lesions (22, i.e. 81%), followed by fracture of the neck of the radius (two patients in displaced equivalent and four patients in non-displaced equivalent). We had only one patient in our group with non-displaced intraarticular fracture of the proximal epiphysis of the radius. We have seen all possible directions of the displacement of the proximal radius in our group of displaced Monteggia equivalents.
Regarding the therapeutic approach to Monteggia lesions, we treated 21 patients (45,5%) with reduction only, 22 patients (48%) with CRIF and three patients (6.5%) with ORIF. In the non-displaced Monteggia equivalent group, we treated 25 patients (92.5%) by simple casting and two patients (7.5%) with ORIF – one patient with intraarticular fracture of the proximal epiphysis of the radius and one with intraarticular fracture of the olecranon with significant distraction. In the displaced Monteggia equivalent group we treated 20 patients (52.5%) with CRIF, nine patients (23.5%) with ORIF, five patients (13%) with reduction only and four patients (11%) by simple casting. There is a statistically significant difference (p < 0.001) in therapeutic approach between all three groups of patients (Tables 2 and 3 and Fig. 4).
Therapeutic approach

Therapeutic approach comparison using Fisher's exact test

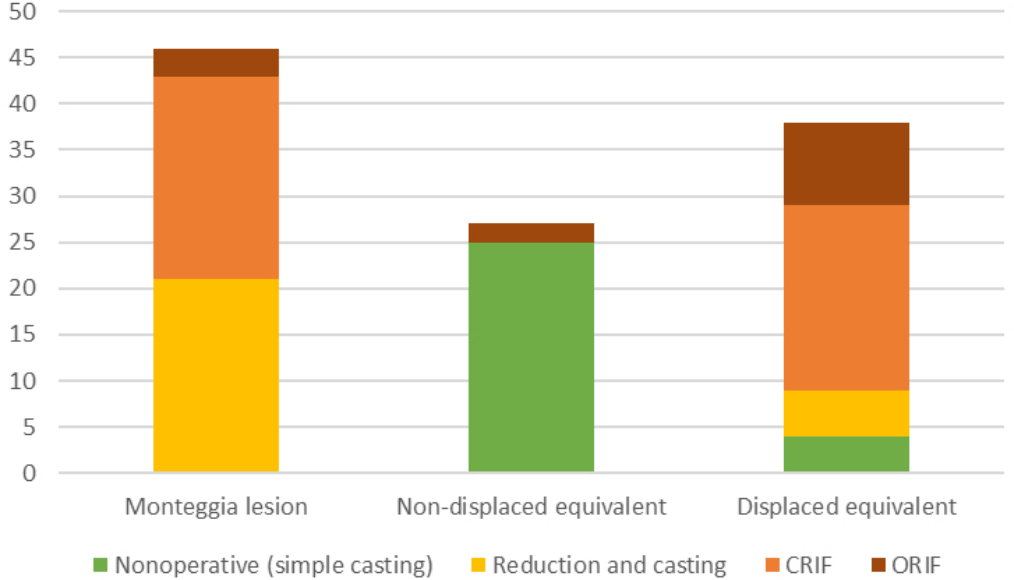
Therapeutic approach chart (CRIF, closed reduction and internal fixation; ORIF, opened reduction and internal fixation).
The outcome of therapy using Letts’ criteria in Monteggia lesions was excellent in 43 patients (93.5%), good in one patient (2%) and fair in two patients (4.5%). In displaced Monteggia equivalents outcome was excellent in 29 patients (76%), good in four patients (11%) and fair in five patients (13%). In non-displaced Monteggia equivalents, all patients had an excellent outcome. In all three groups we had no patient with a poor result. There is no significant difference in outcome between Monteggia lesions and both types of Monteggia equivalents, but there is a statistically significant difference (p = 0.016) between displaced and non-displaced equivalents (Tables 4 and 5 and Fig. 5).
Therapeutic outcome (using Letts’ criteria 7 )

Therapeutic outcome comparison using Fisher's exact test

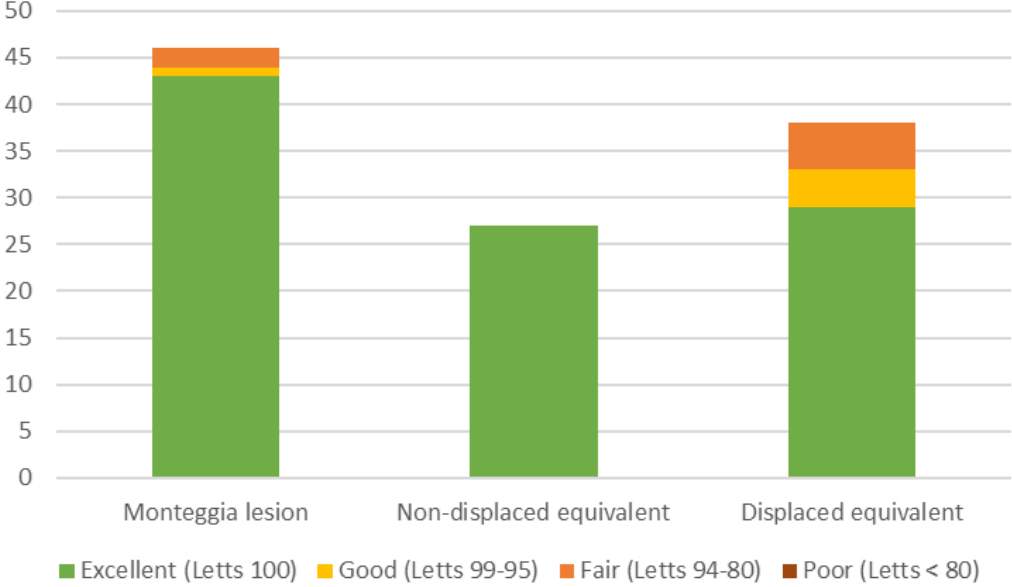
Therapeutic outcome chart.
We had seven patients with complications in our group. Three patients had radial nerve palsy, but in all cases it healed spontaneously without the need for surgical intervention. One patient developed compartment syndrome with the need for a dermatofasciotomy. Two patients had a light valgus deformity of the elbow and one patient had delayed union (both considered in the evaluation of the outcome).
Discussion
Bado's classification of Monteggia lesions is widely accepted in the literature, although not without discussion and tendencies for revision.7,8 It is suitable for the anatomical description of Monteggia lesions and an explanation of the mechanism of the injury. The treatment of Monteggia lesions should be aimed at reduction of the dislocation of proximal radius and preservation of the length of the ulna and its stability to prevent redislocation in the humeroradial joint. This ulnar fracture pattern-based approach to Monteggia lesions has been suggested by many authors.9–12
Monteggia equivalents remain controversial and are repeatedly criticized in literature. Some authors are trying to redefine them3,13–17 while others do not mention them at all.12,18–21 Based on our clinical experience, the only Monteggia equivalent is a fracture of the ulna in any level conjoined with fracture of the proximal radius (metaphyseal or physeal injury). All other lesions mentioned by some authors as Monteggia equivalents are either a ‘true’ Monteggia lesion (bowing fracture of ulna conjoined with dislocation of proximal radius) or do not meet the criteria for Monteggia lesion at all (pulled elbow syndrome, isolated dislocation of the proximal radius, fracture of ulna conjoined with dislocation of the whole elbow joint) and, therefore, should not be termed Monteggia equivalents. Although Monteggia equivalents are mainly termed as equivalents of the Bado type 1, in our group of Monteggia equivalents we have found the displacement of the proximal radius in all possible directions (Figs 6 to 9).
Monteggia equivalent of Bado type 1 – physeal injury of the proximal radius with dorsal displacement (angulation) of the distal fragment conjoined with the physeal injury of the proximal ulna. Treated with closed reduction and internal fixation – percutaneous pinning of the proximal ulna and proximal radius treated with Métaizeau's technique. Injury radiograph with an arrow pointing to the displaced head of the radius (

Monteggia equivalent of Bado type 2 – physeal injury of the proximal radius with ventral displacement (angulation) of the distal fragment conjoined with the physeal injury of the proximal ulna. Treated with closed reduction and internal fixation – percutaneous pinning of the proximal ulna and proximal radius treated with Métaizeau's technique. Injury radiograph (
Monteggia equivalent of Bado type 3 – physeal injury of the proximal radius with ulnar displacement (angulation) of the distal fragment conjoined with the comminutive fracture of the proximal metaphysis of the ulna. Proximal radius treated with Métaizeau's technique, ulna treated with opened reduction and internal fixation by splint. Injury radiograph (
Monteggia equivalent of inverted Bado type 3 – physeal injury of the proximal radius with radial displacement (angulation) of the distal fragment conjoined with the physeal injury of the proximal ulna. Treated with closed reduction and internal fixation – percutaneous pinning of the proximal ulna and proximal radius treated with Métaizeau's technique. Injury radiograph (
In our group of patients, we found three distinct subgroups of lesions – (true) Monteggia lesions, displaced Monteggia equivalents and non-displaced Monteggia equivalents. By evaluation of all three subgroups, we have found essential differences in therapeutic strategy as well as in results of the healing process. In the subgroup of (true) Monteggia lesions, stabilization of fractured ulna and simple closed reduction of dislocation of the proximal radius were crucial. This is in the agreement with the ulnar fracture pattern-based strategy of treatment. In the subgroup of non-displaced Monteggia equivalents, we preferred nonoperative therapy with a simple casting. In this group, only two patients required operative treatment. This treatment, however, was not meant to affect the stability of the humeroradial joint. In the subgroup of displaced Monteggia equivalents, the situation is far more complicated. Operative treatment (CRIF or ORIF) was indicated in most patients of this subgroup. In our department we prefer stabilization of the proximal radius using the technique proposed by Métaizeau et al 22 and stabilization of ulna based on its fracture pattern. We found a statistically significant difference in the strategy of therapy between all three subgroups.
The general opinion is that a promptly recognized and adequately treated Monteggia lesion has a good prognosis in paediatric patients, but Givon et al 23 warns of worse results of treatment of Monteggia equivalents and recommends considering Monteggia equivalents as a specific subgroup of Monteggia lesions with the need to increase attention regarding the therapy. Anatomical proportions of the proximal radius after consolidation have a crucial impact on the movability of forearm and elbow. In our three subgroups of patients, we had excellent results in most of our patients, but displaced Monteggia equivalent has the worst results of them all which confirms the opinion that Monteggia equivalents have a worse outcome than Monteggia lesions. However, there is a statistically significant difference between the outcome of non-displaced Monteggia equivalent (all patients with an excellent result) and displaced Monteggia equivalent (four good and five fair results) and, therefore, we suggest that the non-displaced Monteggia equivalent does not meet the criteria of Monteggia equivalent and Monteggia lesion regarding displacement in the humeroradial joint as well as expected outcome.
Based on our study, we have found three distinct types of injuries in the heterogeneous Monteggia lesion group and its equivalents. These groups differ in the anatomical description of the lesion as well as in the suggested strategy of therapy and its outcome.
Monteggia lesions are defined as a fracture of the ulna at any level conjoined with dislocation of the proximal radius. Fracture of the ulna can usually be found in the diaphysis. Bado's classification is suitable and widely accepted for the anatomical description of the lesion. The strategy of the therapy should be ulnar fracture pattern-based and aimed at the stability of the ulna and preserving its length. Reduction of the dislocation of the proximal radius is mandatory. The outcome of the therapy is good.
Displaced Monteggia equivalents should be defined only as a fracture of ulna at any level conjoined with a displaced fracture of the proximal radius in any direction and mean of displacement (> 1° of Judets’ classification). Fracture of the ulna is frequently found in the olecranon. The strategy of the therapy should be based on the reconstruction of anatomical proportions of the proximal radius, which is crucial for the outcome. In most cases it requires osteosynthesis of the proximal radius, preferably using the minimally invasive technique of Métaizeau. The outcome should be expected to be worse than in the Monteggia lesion. Displaced Monteggia equivalents need increased attention regarding therapy and follow-up.
Non-displaced Monteggia equivalents should be defined as a fracture of ulna at any level conjoined with a non-displaced fracture of the proximal radius (1° of Judets’ classification). Fracture of the ulna can be usually found in the olecranon and its eventual displacement is not considered regarding the classification between the displaced and non-displaced Monteggia equivalent. The strategy of therapy is mostly nonoperative and an operation is required only in rare cases of conjoined displaced ulnar fracture. The outcome of the therapy is excellent.
In our study we present comparatively large group of patients from one institution considering the rarity of both the Monteggia lesion and Monteggia equivalent in paediatric populations. We also use a streamlined and clear definition of the Monteggia equivalent which makes the results of our study more applicable for clinical practice. However, our study has several limitations. One is the retrospective aspect of the study where we collected data from medical reports made by several physicians and from radiographs. We also use the clinical outcome as a measure and there is a lack of the clear functional outcome, although partly represented in Letts’ criteria. Another limitation is a smaller number of patients in each of investigated subgroup.
Conclusion
Based on the presented group of patients we suggest that there are only two lesions that meet the criteria of Monteggia – (true) Monteggia lesion and displaced Monteggia equivalent. Moreover, the Monteggia equivalent should only be classified as a fracture of ulna in any level conjoined with a displaced fracture of the proximal radius. Non-displaced equivalents do not meet the criteria of Monteggia and, therefore, should not be termed a Monteggia equivalent.
Footnotes
TP: Study design, Data analysis, Wrote the manuscript.
PH: Study design, Supervision, Commented on the manuscript.
JH: Data collection.