
Abstract
Abstract
Purpose
The containment orientated treatment of Legg-Calvé-Perthes disease (LCPD) affected hip joints is broadly accepted in the literature. The prerequisite is early recognition of loss of containment. An often-used quantitative MRI containment parameter is the cartilaginous acetabulum-head-index (CAHI). Based on ultrasound (US), we analyzed the newly created ‘femoral head extrusion angle’ (HA) as a containment parameter in comparison with the CAHI in severe LCPD.
Methods
In a prospective study with 40 children (mean age 5.8 years sd 2.3) with unilateral LCPD classified as Catterall group III/IV, we measured the CAHI versus HA to assess the containment of the femoral head. HA in US was determined by the tangent from the bony acetabular rim to the cartilaginous cranio-lateral femoral head.
Results
The HA was significantly higher in LCPD-affected hip joints (25° sd 7°) than in healthy ones (13° sd 5°; p < 0.001). Correlation analysis of all hip joints revealed a significant correlation between HA and CAHI (r = −0.69; p < 0.001). Hip joints with a low CAHI indicating loss of containment showed a higher HA in sonography.
Conclusion
The results of our study suggest that the HA in US is a reliable containment parameter in severe LCPD with a HA > 22° defining a pathologic value. In comparison with the CAHI, HA measurement in ultrasound is easier than the assessment of various parameters to calculate an index. Frequent sonographical follow-up assessment in critical joints is an alternative if MRI is not available, helping to detect an impending loss of containment early enough.
Level of Evidence
Level II
Introduction
Legg-Calvé-Perthes disease (LCPD) is a self-limiting idiopathic avascular necrosis of the capital femoral epiphysis. 1 Assessing the centering of the femoral head inside the acetabulum is crucial in order to choose the right therapy, for monitoring and to evaluate the prognosis of the disease. The concept of containment of the femoral head within the acetabulum is broadly accepted.2–4 The most important parameter indicating a loss of containment is lateralization of the femoral head as a ‘head-at-risk-sign’.5,6 Hence, diagnosing a loss of containment is highly relevant since adequate conservative or surgical therapy should be started as soon as possible to avoid further deformities of the femoral head. 7 In addition to the extent of epiphyseal necrosis, a late onset is also associated with a poor prognosis.8–10 MRI seems to be the best method for indicating early the extent of the femoral necrosis and evaluating risk cases. 11 An established parameter for the quantitative determination of containment in MRI is the cartilaginous acetabulum-head-index (CAHI) that showed good agreement between two observers. 12 According to prior studies, a loss of containment is present if the CAHI is < 75% 12 or < 77%. 13
Studies evaluating the use of sonography for monitoring LCPD are very limited. Some studies have shown that sonography can be used for follow-up examination in containment assessment in LCPD.12,14,15 The advantages of sonography are its ready availability, low cost and lack of side-effects. 16
In the healthy hip joint of the child, the labrum can be displayed below the bony acetabular rim in the ultrasound examination covering the femoral head. In contrast, the impending loss of containment is characterized by an elevated labrum and incipient epiphyseal deformation, whereas a complete loss of containment is typically shown by a cranialized labrum and an epiphyseal extrusion with indentations from the bony acetabular rim.15,37
With the assessment of the distance between the lateral cartilaginous femoral head to the bony acetabular rim (LCD), Terjesen 17 introduced a useful parameter for containment assessment. However, for the correct assessment of the LCD, a direct measurement during the ultrasound procedure is necessary, which can be very challenging in younger children due to reduced compliance. Therefore, the development of an easy and reliable sonographic containment parameter would be of high clinical relevance.
The aim of this study was the evaluation of a new sonographic containment parameter, the femoral head extrusion angle (HA), for containment assessment in LCPD.
Materials and methods
Study group
In this prospective study, we examined 40 children (ten female) with unilateral LCPD classified as Catterall group 5 III (27 children) or IV (13 children) who had received an MRI examination of the pelvis, a sonography of both the affected and the healthy hip joint as well as an initial plain radiography. In addition, 34 children of our collective were re-examined once or several times (maximum six times) after conservative therapy or surgery (77 re-examinations). These follow-up sonographies and MRI examinations were evaluated separately in this study as these children were already known to the examiners which could possibly influence their containment evaluation. All patients were recruited in the paediatric orthopaedic consultation-hour of our university hospital. The study was approved by the local ethics committee.
Ultrasound
For the evaluation of the hip sonography, a lateral longitudinal ultrasound was performed according to the guidelines of the German Society of Ultrasound in Medicine (DEGUM). 18 The patients were placed in a supine position with the lower leg hanging freely over the edge of the examination bed, guaranteeing a reproducible examination with both legs in neutral rotation and the hips fully extended. A 7.5 MHz linear transducer (Siemens AG, Berlin/Munich, Germany) was used for all examinations.
The measurement of the sonographic HA is orientated to Graf-technique in congenital hip dysplasia.19,20 For HA measurement, we also used the basic line by Graf, that is parallel to the longitudinal ilium bone in lateral longitudinal ultrasound (Fig. 1). The basic line is then shifted in parallel to the most lateral point of the bony acetabular rim (LA). In contrast to the Graf-technique, we determined the HA by drawing a second line from the LA that is tangent to the cartilaginous femoral head, i.e. the cartilage-capsule-border, whereas Graf calculated the beta-angle by drawing a line from the LA to the inner surface of the labrum. The difference between the low echo of the cartilaginous femoral head and the high echo of the hip capsule can be identified easily. The HA is measured in degrees. An experienced paediatric orthopaedic surgeon (M.H.F.S.) with good expertise in infant musculoskeletal ultrasound (DEGUM instructor level III) performed all sonograms. In a second step, the examiner M.H.F.S. (O1) and a second observer M.S. (O2) took the measurements on the initial sonogram of both hips and on the sonograms of the follow-up examinations independently. O2 did the measurements a few days after the sonograms were performed and with no knowledge of the affected hip joint. He is a practising general surgeon with good knowledge of musculoskeletal ultrasound, but no knowledge in ultrasound of the infant hip joint and did not work in the same university hospital.

Measurement of the femoral head extrusion angle (HA) in lateral longitudinal ultrasound (LA, lateral margin of the bony acetabular rim; L, labrum; C, margin of the cartilaginous femoral head; B, bony femoral head): (
Additionally, an examination of joint effusion was performed in all hips using an anterior sonographic scan in a longitudinal plane along the axis of the femoral neck, which is most relevant for effusion assessment. All hips were categorized in three groups: no joint effusion, small (capsular distention < 3 mm in comparison with the contralateral healthy hip joint) or large joint effusion (capsular distention > 3 mm), similar to prior categorization of capsular distention. 21
MRI
The T1-weighted MR images of the pelvis (repetition time 400-600ms, echo time 10-20ms) were obtained using 4-mm slices. For analysis, the coronal slice showing the maximum diameter of the femoral head was used. The distance from the medial cartilaginous femoral head to the lateral cartilaginous acetabular rim and the maximum femoral head diameter were measured (Fig. 2). The index was calculated in the same way as in previous studies. 12
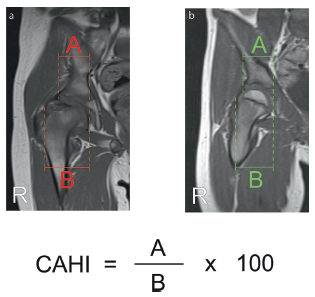
Quantitative determination of containment with the cartilaginous acetabulum-head-index (CAHI) as a percentage (
All data were digitalized and analyzed using Scion Image Beta 4.02 (Scion Corporation, Frederick, Maryland). The measurement of the CAHI in healthy and LCPD-affected hip joints was done by the first observer only (O1).
Plain radiography
We classified all LCPD-patients by plain radiography according to Catterall. 5 Radiographs were taken at their first presentation in our outpatient clinic. The bony acetabulum-head-index (AHI) was calculated as follows: 22 the distance from the medial margin of the femoral head to the most lateral point of the bony acetabular rim was divided by the horizontal width of the femoral head and converted into a percentage (Fig. 3). An AHI < 80% has been reported to identify early displacement of the femoral head. 23
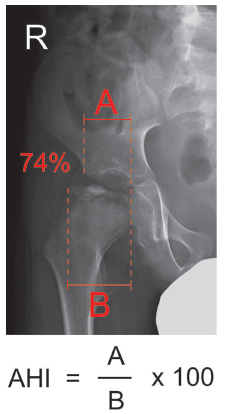
Plain radiography of the right hip joint of a six-year-old boy with Legg-Calvé-Perthes disease and calculation of the acetabulum-head-index (AHI): the distance (
Statistical analysis
The statistical analysis was performed using SPSS (IBM Inc., Armonk, New York; version 22.0.0.1). The interobserver variability of the new HA assessment was evaluated using intra-class correlation (ICC) analysis. The interrelation between the HA and the CAHI or AHI was evaluated using the Pearson correlation. It was visualized using linear regression.
The comparison of the HA and the CAHI or AHI of healthy hip joints and LCPD-affected hip joints was done with paired t-tests. Normal values were defined by the mean value ± two standard deviations for the HA in healthy hip joints and compared with the determined CAHI values.
In a subgroup analysis, LCPD patients were split into two groups with an age of less than six years or six or more years for further analysis with t-tests, as age is an important prognostic parameter in LCPD. 10
In a second step, we also analyzed sonographic follow-up examinations of LCPD-affected and healthy hip joints separately by using ICC analysis.
If not stated otherwise, we report the mean value (sd). All calculated HA in degrees and CAHI in percentages were rounded to the nearest integer.
Results
The mean age of the patients at the time of the examinations was 5.8 years sd 2.3 with a range from two to 11 years. Between MRI examination and hip sonography, a mean time of three weeks passed (3.0 weeks sd 3.5).
The values for the HA and the CAHI in both healthy and LCPD-affected hip joints were normally distributed.
In all healthy hip joints, no joint effusion was found in the anteroposterior sonography scan. In LCPD-affected hip joints, nine patients showed no joint effusion, but in some patients discrete (n= 16) or clearly detectable joint effusion (n = 15) was found.
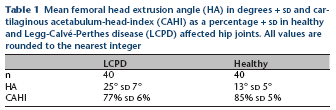
The mean HA in LCPD-affected hip joints (25° sd 7°) was significantly higher than in healthy hip joints (13° sd 5°; T(1,39) = 9.06; p < 0.001) (Table 1). Consistent with that, the mean CAHI as a MRI containment parameter in LCPD-affected hip joints (77% sd 6%) was significantly lower than in healthy joints (85% sd 5%; T(1,39) = −6.66; p < 0.001). We found a significant negative correlation between HA and CAHI in all hip joints (r = −0.69; lower 95% CI: r = −0.80, upper 95% confidence interval (CI): r = −0.53; p < 0.001) (Fig. 4). Hip joints with a low CAHI indicating a loss of containment showed a higher HA in sonography. In plain radiography, the mean AHI in LCPD-affected hip joints (87% sd 9%) was significantly lower than in healthy joints (93% sd 8%; p = 0.002). In all hip joints, the AHI correlated moderately with the CAHI in Pearson correlation analysis (r = 0.45; lower 95% CI: r = 0.27, upper 95% CI: r = 0.61; p < 0.001) and ICC analysis (ICC = 0.43; 95% CI: 0.22 to 0.60; p < 0.001) measured at the first examination. In 11 out of 19 hip joints with loss of containment according to MRI criteria (CAHI < 75%) 12 a normal AHI > 80% 23 was present.
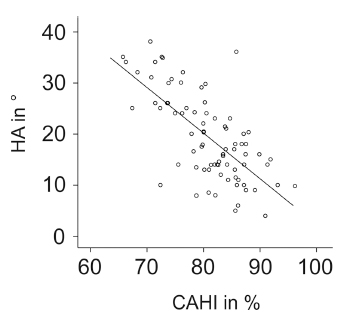
Linear regression between the femoral head extrusion angle (HA) in ultrasound and the cartilaginous acetabulum head index (CAHI) in all hip joints measured.
Mean femoral head extrusion angle (HA) in degrees + sd and cartilaginous acetabulum-head-index (CAHI) as a percentage + sd in healthy and Legg-Calvé-Perthes disease (LCPD) affected hip joints. All values are rounded to the nearest integer
Subgroup analysis of LCPD-affected hip joints of children less than six years (n = 23) showed no significant differences in comparison with children six or more years of age (n = 17) for the HA (26° sd 7° versus 25° ± 8°; T(1,38) = 0.28; p = 0.78) or CAHI (77% sd 7% versus 77% sd 5%; T(1,38) = 0.02; p = 0.98).
The comparison of the HA measurement between two independent observers showed a strong correlation in all examined hip joints (ICC = 0.91; 95% CI: 0.86 to 0.94; p < 0.001) (Fig. 5). The mean difference between the HA measurement of O1 and O2 was 1° sd 3°.
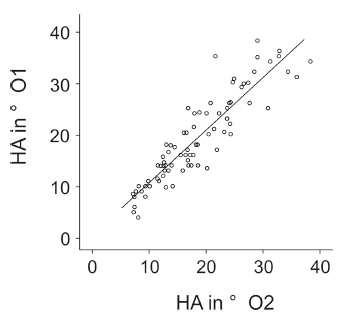
Linear regression between the femoral head extrusion angle (HA) in ultrasound assessed by observer O1 and observer O2 in all hip joints measured.
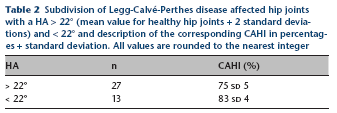
Using the mean HA + two sd of healthy hip joints, an HA of > 22° was defined as a pathologic containment. LCPD-affected hip joints with a HA > 22° (n = 27 of 40) showed a mean CAHI of 75% sd 5%, but with a HA < 22° (n = 13 of 40) the mean CAHI was 83% sd 4% (Table 2).
Subdivision of Legg-Calvé-Perthes disease affected hip joints with a HA > 22° (mean value for healthy hip joints + 2 standard deviations) and < 22° and description of the corresponding CAHI in percentages + standard deviation. All values are rounded to the nearest integer
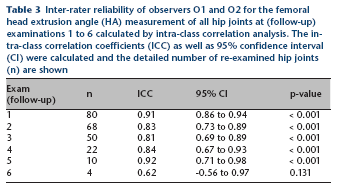
Most of the children of the collective (n = 34) were re-examined once or several times by sonography and MRI in the course of the disease. The time between the first and the last examination ranged from three weeks to 2.4 years for sonographic follow-up and from seven weeks to 2.5 years for MRI follow-up scans. The inter-rater reliability between both observers for the HA assessment of all hips at follow up examinations 2 to 5 was high. The calculated ICCs ranged between 0.81 and 0.92 (Table 3). LCPD-affected hip joints in follow-up examinations with a HA > 22° (n = 32 of 77) showed a mean CAHI of 74% sd 5%. The mean CAHI for healthy hip joints in follow-up examinations with a HA < 22° (n = 76 of 77) was 85% sd 5%.
Inter-rater reliability of observers O1 and O2 for the femoral head extrusion angle (HA) measurement of all hip joints at (follow-up) examinations 1 to 6 calculated by intra-class correlation analysis. The intra-class correlation coefficients (ICC) as well as 95% confidence interval (CI) were calculated and the detailed number of re-examined hip joints (n) are shown
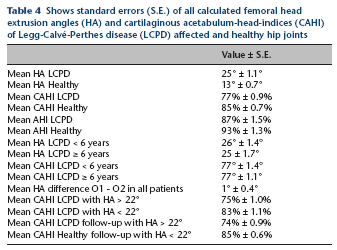
In Table 4 we show all results of our data analysis with standard error.
Shows standard errors (S.E.) of all calculated femoral head extrusion angles (HA) and cartilaginous acetabulum-head-indices (CAHI) of Legg-Calvé-Perthes disease (LCPD) affected and healthy hip joints
Discussion
In containment-oriented therapy for LCPD, several parameters for the binary or quantitative determination of femoral head containment may be considered. For the evaluation of containment, the acetabular roofing of the femoral head is most suitable. 24 In 1950, Heyman and Herndon 22 described the acetabulum-head-index (AHI) for the quantitative determination of containment on radiographs. In clinical research, the AHI is rarely used today. Compared with binary parameters, quantitative parameters are preferred for the assessment of containment. 25
Terjesen 17 compared epiphyseal protrusion using sonography with X-rays. In this study, the containment diagnostic was further developed as sonography was compared with MRI. In contrast to conventional X-rays, MRI can display the cartilaginous portions of the femoral head and the acetabulum, which allows for a very precise determination of containment. Some authors speak of true containment in MRI.26,27 With MRI, not only is an early diagnosis of LCPD possible, 11 so is an early determination of the loss of containment. Arthrography and MRI reveal a loss of containment, although it was not detectable in conventional X-ray photography. 28 This is in line with our radiographical containment assessment. The AHI of all hip joints correlated only moderately with the CAHI and in approximately 58% of our LCPD-affected hip joints with loss of containment in MRI a normal AHI in plain radiography was present. This could be explained by the fact that the calculation of the CAHI in MRI considers the cartilaginous structures of the hip joint. Compared with arthrography, containment assessment in MRI showed no significant differences.28,29 For the first time, a new sonographic parameter – the HA – was compared with MRI containment diagnostics. We showed that the HA has high validity and shows low interobserver variability. The HA of LCPD-affected hip joints was significantly higher than in healthy hip joints. Fittingly, the reference MRI examination showed a significantly lower CAHI in LCPD-affected hip joints. For all hip joints, a reduced CAHI was linked with a higher HA. Age does not seem to influence the HA as we found comparable HA values in both subgroups with an age less than six years or six or more years. Similar to former studies, 30 we obtained our data from contralateral healthy hip joints to identify a limit for the HA in sonography. In our sample of 40 healthy hip joints, the mean HA + two sd was 22°. We defined a HA > 22° as a pathological value. When the HA values in LCPD-affected hip joints were above 22°, a highly pathologic mean for the CAHI of < 75% was present. Additionally, the analysis of follow-up examinations showed also a highly pathologic CAHI of 74% when a HA > 22° was determined. In the literature, a CAHI < 75% 12 or < 77% 13 is associated with a loss of containment.
In general, surgical procedures are preferred in case of loss of containment. 31 A large prospective multicentre study showed better outcome after surgical treatment compared with conservative treatment in patients older than eight years at the time of onset with lateral pillar group B or border group B/C hip joints according to the Herring classification. However, operative treatment does not always lead to good clinical outcome, especially in Herring group C hips. 32 But until now, there has been no consensus or guideline with a favoured surgical procedure. 31 Proximal femoral (derotating) varus osteotomies as well as pelvic osteotomies or combined osteotomies are implemented successfully.33,34
In hip joints with an improvement of containment postoperatively, an aggravation of containment may appear again with the need for further operative treatment. In this context, follow-up sonography for containment assessment is uncomplicated and it is not disturbed by osteosynthesis material. This view is supported by the results of our follow-up examinations also including postoperative sonographic re-evaluation with implants.
One limitation of our study is the possible influence of joint effusion on the HA assessment in sonography. Joint effusion was found in 76% of all LCPD-affected hip joints. However, it is part of LCPD 35 and leads to pain as well as a restriction of range of movement of the hip joint. 21 Therefore, it should be treated first to relieve patients of these symptoms by the use of traction, partial weight-bearing and anti-inflammatory medication before addressing the problem of hip joint incongruence by conservative or operative treatment. 36 Furthermore, it has to be considered that performing musculoskeletal ultrasound correctly requires several months of practise, but it can be learned by frequent training. In contrast to performing the ultrasound, the measurement of the HA is quick to learn – for fellows, practising orthopaedic surgeons and residents equally. Additionally, sonographic containment assessment with HA measurement should always be accompanied by anamnesis, assessment of pain intensity and clinical examination concerning a restriction of movement.
Our results indicate that sonography seems to be an adjunct to the assessment of children with LCPD. Previous studies showed that sonography is useful in monitoring joint effusion, evaluating femoral head extrusion and recognizing the healing phase of the disease.12,15,21 Wirth and colleagues 37 published a chronological ultrasound staging in LCPD. We suggest the determination of the HA in sonography, after the diagnosis of LCPD based on the benchmark examination MRI and clinical examination. If a normal containment is determined in both findings (CAHI > 75% and HA < 22°), the HA alone can be measured in the course of containment assessment. In follow-up examinations, a steady normal HA would help to evaluate the effectivity, e.g. of conservative therapy. After surgical therapy, HA measurement would help evaluating if the resulting containment persists postoperatively. If the HA climbs above 22° over time, then a further exclusion of loss of containment should take place. According to the good correlation between CAHI and HA and the results from our follow-up examinations underlining the relationship between both containment parameters, frequent sonographic follow-up assessment in critical joints is an alternative if MRI is not available. It helps to detect a decrease in containment at an early stage.
Conclusion
Our study establishes the HA assessment in sonography as a useful tool for the evaluation of femoral head containment in LCPD, especially for clinical research. The HA correlated well with the CAHI as an established containment parameter. Further studies should routinely include the HA as a sonographic containment parameter in LCPD, because of its availability, absent side-effects and low cost. The predictive clinical value remains to be investigated in future studies comparing different methods of treatment.