
Abstract
Aim
Pulled elbow or nursemaid's elbow is a radial head subluxation caused by a sudden pull on the extended pronated forearm. Children with pulled elbow usually respond dramatically for reduction, yet others show delayed improvement with no clear pathologic explanation. The aim of our study is to propose an explanation for the varying clinical response after the reduction of pulled elbow aided by ultrasound classification of the underlying pathology and its impact on management.
Patients and methods
Fifty children with a mean age of 3.8 ± 1.1 (standard deviation [SD]) years with pulled elbow were scanned by static and dynamic ultrasound utilizing the other elbow as the standard. The radial annular ligament (RAL) was examined for integrity and interposition, with measurement of the radiocapitellar distance. Reduction was performed following the hyperpronation technique, and postreduction splinting was guided by ultrasound findings. Postreduction scans and 1-year follow up were performed.
Results
Of the 50 included children, 39 (78%) had intact, yet interposed annular ligament (classified as type I) and 11 (22%) had torn annular ligament (classified as type II). The latter underwent splinting for 7 days. Three out of the 50 children had recurrent subluxation and constituted false-negative cases for the detection of torn ligament and represented the reoccurrence rate of 6%. The sensitivity, specificity, and accuracy for the ultrasound diagnosis of torn RAL were 76.9, 92.3, and 92%, respectively.
Conclusion
Pulled elbow is classified as follows: type I, with an interposed RAL, and type II, with torn ligament.
Introduction
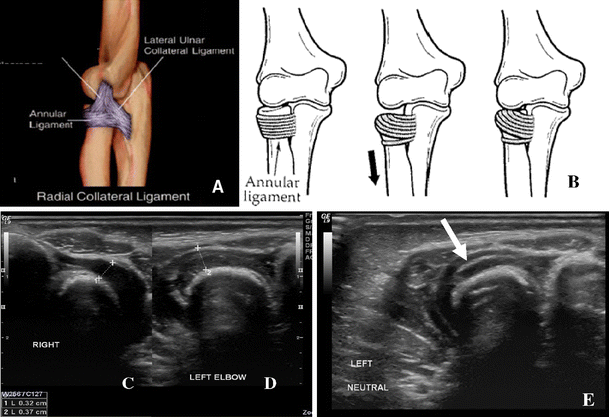
Pulled elbow, also known as nursemaid's elbow or radial head subluxation, commonly affects children under 5 years of age. Occasionally, it occurs bilaterally. Pulled elbow is usually caused by a traction injury when force is applied longitudinally to a pronated extended elbow. Examples include situations in which children are abruptly picked up from the floor by their hands or when children are suddenly pulled back by their hand as they are falling down [1].
The elbow of the child differs from the adult elbow in many ways. One important difference is that the annular ligament attachments are thicker and, therefore, stronger in adults than in children. The radial head is ovoid and about 30% larger in diameter than the radial shaft. Because of the ovoid shape, the profile of the radial head becomes smaller when the forearm is pronated [2].
Pulled elbow is a benign condition that usually passes uncomplicated. However, some patients experience recurrence. The exact pathology of pulled elbow is still to be defined.
Salter and Zaltz [3] described the condition as annular ligament tear, while Choung and Heinrich [1] stated that the cause was radial head subluxation. Macias et al. [4] presented multiple theories and Kaplan and Lillis [5] named the condition annular ligament displacement. The reason for delayed recovery after reduction and the likelihood of recurrence have yet to be determined. The role of ultrasound in the diagnosis of pulled elbow has been evaluated by previous studies [6, 7], but the role of dynamic imaging has never been studied, neither has any ultrasound-based classification.
The aim of our study is to propose an explanation for the varying clinical response after reduction of pulled elbow aided by ultrasound classification of the underlying pathology and its impact on management.
Patients and methods
Fifty children, 33 females and 17 males, were included in the study between April 2008 and April 2010. They were diagnosed as pulled elbow based on their history and physical examination. Their ages ranged between 2 and 5 years, with a mean of 3.8 ± 1.1 (standard deviation [SD]) years. All children were referred to the radiology department for standard radiograph and ultrasound of the elbow. The inclusion criteria included: definitive history of pull injury and a negative standard radiograph. The exclusion criteria included bilateral conditions and children with history of pulled elbow of either side.
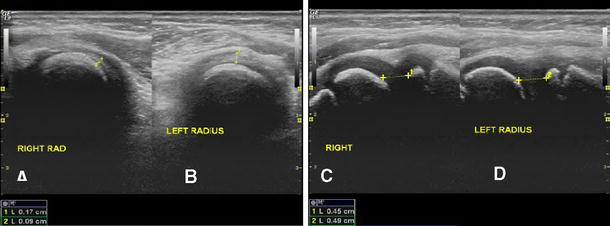
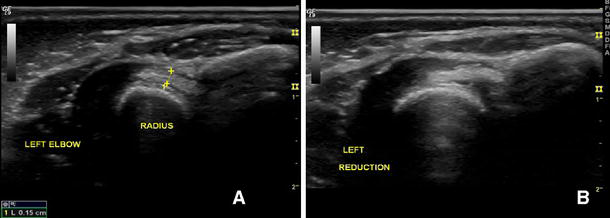
Ultrasonography was performed using a high-resolution 14-MHz linear probe on a GE Logiq 9 Ultrasound Machine (GE Healthcare, Milwaukee, WI, USA). The child was seated opposite to the radiologist or held on his/her parent's lap. The elbow was extended; the head and neck of the radius were scanned from the dorsal aspect. Static images and dynamic mini-video clips in supination and pronation were obtained of the injured and normal elbows and saved on a PACS for reporting and later reviewing. The diagnostic criteria for annular ligament interposition and radial head subluxation were: (1) widened joint space, (2) increased radiocapitellar distance, (3) increased joint space echogenicity in comparison to the other elbow (which is anechoic), and (4) limitation in the range of movement in pronation and supination during dynamic scanning (Figs. 1 and 2). Annular ligament tear was diagnosed when the ligament is seen as a thick hyper-echoic linear structure in the joint space having a free edge (Fig. 3), in addition to the other ultrasound signs. After reduction, the intact annular ligament is seen as a triangular echogenic structure at the joint periphery (Fig. 4).
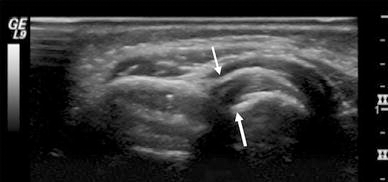
The right elbow showing normal appearance of the radial collateral ligament as an echogenic triangular structure with a peripheral wide base seen in between the white arrows
Reduction was attempted in the ultrasound department. We followed the hyperpronation technique in all children. In this maneuver, one grasps the hand of the patient's affected arm as if to shake it. The other hand is placed under the affected elbow. The patient's forearm is then simultaneously pronated and the elbow is extended. The elbow is then flexed with the forearm maintained in pronation to complete the maneuver [4, 8] (Fig. 5). Immobilization followed Kaplan and Lillis’ regimen of immobilization [5], initially designed for recurrent conditions, in which the elbow is splinted at 90° flexion with as much supination of the forearm as comfort will allow. The splint is applied for 7 days for children with ligament tear.

Demonstrates reduction by pronation: simultaneous pronation of the wrist and extension of the elbow (
A postreduction dynamic study was repeated illustrating the full range of movement. Children were followed up for 1 year to record recurrence. Dynamic ultrasound was repeated for recurrent conditions and in all cases at final follow up. Statistical analysis was performed through calculation of the sensitivity, specificity, accuracy, negative, and positive predictive values of the radiological signs in the diagnosis of torn radial annular ligament (RAL).
Results
The study included 50 children; 39 (78%) had type I pulled elbow, interposed RAL, and subluxated radial head, while 11(22%) had type II pulled elbow with torn RAL and subluxated radial head. All patients in this study had successful reduction of the subluxated radial head after manipulative reduction. The radiocapitellar distance of the pulled elbows was significantly greater than the normal elbows, measuring 6.4 mm ± 0.8 SD to 4.3 mm ± 0.6 SD, respectively, with a P-value < 0.0001.
Thirty-six of 39 (92%) children had interposed RAL with subluxated radial head; they were followed up for 1 year with no reoccurrence. Three of 39 (8%) children experienced recurrence. Ultrasound scan performed at the time of recurrence revealed the free echogenic edge of the torn annular ligament and they constituted the false-negative results for torn annular ligament. They had a splint for 7 days and none had a third episode. Eleven of 50 (22%) children had a torn annular ligament. Ten of 11 (90%) children were confirmed for ligament tear on postreduction scan, none had recurrence, and they constituted the true-positive results. One of 11 (10%) children was found not to have a torn ligament on postreduction scan and constituted the false-positive result.
The sensitivity, specificity, accuracy, positive, and negative predictive values for the individual ultrasound signs in the diagnosis of type I and type II pulled elbow are demonstrated in Table 1. Widened joint space and increased radiocapitellar distance during dynamic scanning have the highest sensitivity (97.3%) in the diagnosis of type I pulled elbow. The echogenic edge of the torn annular ligament has the highest specificity (97.9%) and positive predictive value (96.9%) in the diagnosis of pulled elbow.
The statistical data of the ultrasound signs in the diagnosis of pulled elbow
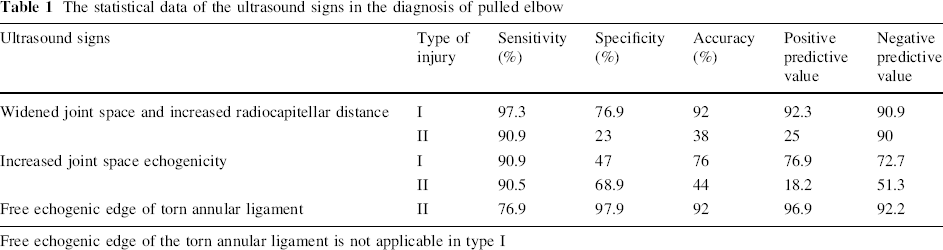
Free echogenic edge of the torn annular ligament is not applicable in type I
Discussion
Pulled elbow is a benign condition that usually affects children under 5 years of age. The condition is usually caused by a traction injury when force is applied longitudinally to a pronated extended elbow. The terminology includes nursemaid's elbow, radial head subluxation, radial head dislocation, annular ligament tear, and annular ligament displacement. The synonyms of nursemaid's elbow reflect a once obscure understanding of its pathology [2, 4]. Among initial reports from the 1800s, the focus was on determining whether the injury occurred at the wrist or the elbow [9]. Some suggested a tug on the pronated forearm as a mechanism of injury, thereby, pulling the radius through the annular ligament, which may partially tear and become entrapped between the radial head and the capitellum [10]. Subsequent studies did not provide a comprehensive clue for the actual pathology. In this study, we agree with other authors [2, 4, 11] that the radial head, under axial traction with the forearm pronated, is subluxated and becomes trapped distal to the annular ligament, which is interposed, with widened radiocapitellar distance, either in ultrasound [7] or on standard radiograph [1], causing pain with movement. This is in contrast to Bretland [12] and Lee et al. [13], who stated that the radiographic findings in this condition are normal.
The conflict extended from understanding the pathology to the technique of reduction. Two maneuvers are commonly used when attempting to reduce pulled elbow: supination or pronation (sometimes termed hyperpronation) [4, 8]. We implied the pronation maneuver for all children included in this study.
Dynamic ultrasound showed limited radial head rotation during pronation and supination, which was never discussed in the previously published literature, and the regain of the full range of movement following reduction was demonstrated in mini-video clips. The torn subluxated annular ligament explains the absence of reduction click and the failure of immediate improvement in some children following reduction. We concluded that the conflict in understanding the pathology of pulled elbow is the result of trying to unify the pathological events in one group. Correlation between ultrasound findings and clinical response indicates that pathological events in pulled elbow are not uniform.
A new ultrasound-based classification for the pathological events is proposed in which pulled elbow is classified into two types: type I with radial head subluxation, annular ligament interposition and type II with radial head subluxation, annular ligament tear.
The clinical impact of this classification concerns immobilization. Taha [14] recommended casting for 2 weeks for all children to decrease recurrence, while Kaplan and Lillis [5] recommended immobilization for 10–14 days in cases of recurrent pulled elbow. According to our classification, type I pulled elbow did not follow any regimen of immobilization, while in type II, the elbow was splinted for 7 days, which corresponded to the inflammatory and early reparative phases of ligament healing [15] and, yet, does not reduce the connective tissue mechanical properties values concerning load and stiffness [16].
This classification is thought to be valuable in the management of pulled elbow. Proper understanding of the real pathology and classification of the condition should resolve the question that arises when the child shows neither reduction pop nor prompt clinical improvement after manipulative reduction. In such clinical situations, and if dynamic ultrasound is not available for confirmation, the child would be treated as type II pulled elbow and splinted for 1 week.
Early studies report recurrence rates as low as 5% [17], whereas more recent studies reported recurrence rates between 26.7 and 39% [18, 19] and 32.9% [8]. In our study, the recurrence rate was 6% and is attributed to the failure to recognize torn ligaments during the initial ultrasound study because of limited experience in the early stage of the study. This was picked up in the follow up scans as the learning curve increased. The limitation of our study was mainly the small number of patients, especially of type II pulled elbow. A follow up randomized study for type II treatment without and with splinting is suggested.
The limited number of children with type II pathology in this study opens the door for larger scale anticipated studies. A randomized study concerning splinting and, moreover, the immobilization period will be of great value.
In conclusion, pulled elbow is a radial head subluxation that can be either with an interposed RAL (type I) or torn ligament (type II). Dynamic and static ultrasound imaging can help with the proper understanding of the pathology and represent a valuable tool in differentiating types when clinically uncertain.