
Abstract
Purpose:
To assess the health-related quality of life and radiographic outcomes of surgically treated adolescent Scheuermann’s kyphosis patients after minimum of 2-year follow-up and to compare the health-related quality of life with age- and sex-matched healthy controls.
Methods:
Twenty-two consecutive adolescents (mean age = 16.7 years) undergoing posterior spinal fusion for Scheuermann’s kyphosis were included and matched by age and sex with two healthy controls. The health-related quality of life was evaluated using the Scoliosis Research Society-24 questionnaire. Radiographic parameters were measured for comparison preoperatively and at 6 months and 2-year follow-ups. The health-related quality of life parameters were compared with healthy controls at 2 years of follow-up.
Results:
The mean maximal thoracic kyphosis improved from 79° (range = 75°–90°) to 55° (range = 45°–75°) (p < 0.001), and the mean lumbar lordosis was reduced from 71° (range = 51°–107°) to 52° (range = 34°–68°) (p < 0.001) after 2 years postoperatively. Incidence of proximal junctional kyphosis (PJK) was 18%. The scores of the Scoliosis Research Society-24 improved, with statistical significance observed in pain and self-image domains from preoperative to 2-year follow-up (p = 0.002 in both domains). The self-image and function were significantly lower in the operated patients at their 2-year follow-up visit compared to controls (p = 0.023 for self-image and p < 0.001 for function).
Conclusion:
Instrumented posterior spinal fusion improves the health-related quality of life of Scheuermann’s kyphosis patients during the 2-year follow-up. The greatest improvement is observed in pain and self-image domains. The health-related quality of life in pain and activity domains reaches the level of healthy individuals, while function and self-image remain at a statistically lower level.
Keywords
Introduction
Scheuermann’s kyphosis (SK) is the most common cause of severe thoracic kyphosis, with an estimated prevalence of 1%–8% in the general population.1,2 It is defined as thoracic kyphosis greater than 45° with greater than 5° of anterior wedging in three consecutive vertebrae. Clinically, the SK patients present with a rigid hyperkyphosis in the mid-thoracic or lower-thoracic spine with a compensatory hyperlordosis of the cervical and/or lumbar spine. SK is typically present during the late juvenile and adolescent period. Neurological findings are rare, but the condition is sometimes painful. 3
Patients with thoracic kyphosis greater than 75° and progressive curve despite non-operative methods (i.e. exercise, bracing), refractory pain, respiratory problems, and/or neurologic deficit may indicate surgical correction of the deformity.4,5 Surgery for the correction of SK aims to lengthen the anterior vertebral column while shortening the posterior column. This is achieved by multi-segmental posterior closing-wedge osteotomies across the apical levels to prevent stretching of the cord. It typically gives good and stable functional and radiological results. The correction of kyphosis with instrumentation can be performed using posterior-only or combined anterior–posterior procedures. 6 The posterior-only fusion using hybrid instrumentation, closing-wedge osteotomies, and autologous bone grafting gives excellent results and has low complication rates.7,8
Health-related quality of life (HRQOL) of patients in adolescent idiopathic scoliosis (AIS) has been studied extensively.9–11 Conversely, the studies assessing HRQOL of SK patients is relatively limited. Like AIS, SK can affect the quality of life. Increasing sagittal plane deformity has a significant impact on HRQOL with increased pain, lower self-image, and decreased function and activity.12,13 Previous studies which have assessed the HRQOL of surgically treated SK patients have compared the results with AIS patients or with non-operated SK patients.14,15 To our knowledge, there are no studies which compare the effect of operative treatment to HRQOL on SK patients with age- and sex-matched healthy controls.
In this study, we aimed to investigate whether the HRQOL improves in adolescent who underwent operative treatment for SK using posterior spinal fusion with pedicle screw instrumentation during a postoperative follow-up of 2 years. Furthermore, we compared the HRQOL scores of these patients with age- and sex-matched healthy individuals. We hypothesized that surgical treatment would result in improved health-related quality of life and that it would reach the level of healthy control group.
Materials and methods
Patients
Twenty-two consecutive patients aged between 13 and 19 years with operatively treated SK were prospectively enrolled from May 2009 to March 2020 in this study. The patients were selected based on diagnosis of operatively treated SK and were without congenital spinal anomaly or previous spinal surgery. All patients underwent posterior spinal fusion using segmental pedicle screw instrumentation. The indication for surgery was a thoracic kyphosis with a curve greater than 75°. All patients were operated by a single consultant orthopedic spine surgeon and had a minimum of 2-year follow-up.
Healthy control group
Two controls were matched with each SK patient for age (±2 years) and sex in the last follow-up (2:1). The controls were derived from our previously published population-based study, carried out between January 2012 and December 2015. 16 In this study, 272 healthy controls were selected from a population register to complete the Scoliosis Research Society-22r (SRS-22r) questionnaire, 17 which is a modified version of the Scoliosis Research Society-24 (SRS-24) questionnaire. 18
Surgical technique
All patients underwent posterior-only approach. Segmental pedicle screw instrumentation was inserted from sagittal stable vertebra using the posterior sacral vertical line (typically L2) to upper thoracic spine (typically T2 or T3) using free hand technique. 19 Apical posterior column osteotomies were performed in all patients to facilitate deformity correction. 20 The number of posterior column osteotomies was based on the flexibility of kyphosis intraoperatively. The correction of kyphosis was performed using double rod cantilever maneuver (proximal to distal) and with additional apical compression closing the apical posterior column osteotomies. Local bone from facetectomies with bone graft extenders was used for posterolateral spinal fusion. Intraoperative spinal cord monitoring (motor evoked potentials, somatosensory potentials, lumbar nerve root electroneuromyography) was used in all patients. Screw placement was verified using postoperative computed tomography (CT) scans.
Outcome parameters
Perioperative data were recorded, as well as radiographic outcomes and SRS-24 scores preoperatively, and at 6 months, and 2-year follow-ups. Perioperative data included fusion levels, number of osteotomy levels, blood loss, operative time, perioperative complications, and used bone substitutes. For radiographic measurements, standing anterior–posterior and lateral radiographs were collected. Of the lateral radiographs, thoracic kyphosis (T2–T12), maximal thoracic kyphosis, lumbar lordosis (T12-S1), sagittal vertical axis (SVA), pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS) angles were measured. Of the anterior radiographs, scoliosis angle and central sacral vertical line (CSVL) were measured at all time points. The proximal junctional kyphosis (PJK) was defined by two criteria: a proximal junctional sagittal Cobb angle ≥10° and at least 10° greater than the preoperative measurement. 21 PJK was measured postoperatively at 6 months and at 2 year follow-ups. The status of the instrumentation was evaluated for signs of loosening or screw/rod damage. Radiographic measurements were made by an independent observer.
Health-related quality of life
The health-related quality of life of the SK patients was assessed preoperatively and postoperatively using disease-specific Scoliosis Research Society-24 (SRS-24) questionnaire. 18 SRS-24 is a 24-item questionnaire, in which each item is scored on a 5-point Likert-type scale from one to five and the maximum score is 120. The higher score indicates better patient outcome. The questionnaire has seven domains: pain, general self-image, general function, general activity level, postoperative self-image, postoperative function, and patient satisfaction. The questions number 16–24 concern the treatment and are filled out only postoperatively.
In this study, the healthy control group filled out the SRS-22r questionnaire, which is an improved version of the original SRS-24.17,18 The first 15 questions of the SRS-24 are exactly the same as or close to questions in the SRS-22r. The questions number 1–15 of SRS-24 correspond with the questions 1, 2, 4, 5, 6, 8, 9, 11, 12, 14, 15, and 17–20 of the SRS-22r. These questions were used as a basis for four domains. They were forms as follows: pain (SRS-24: 1, 2, 3, 6, 8, and 11; SRS-22r: 1, 2, 4, 8, 11, and 14), general self-image (SRS-24: 5, 14, and 15; SRS-22r: 6, 19, and 20), general function (SRS-24: 7, 12, and 13; SRS-22r: 9, 15, and 18), and general activity (SRS-24: 4, 9, and 10; SRS-22r: 5, 12, and 17). 22 In addition, the scores of the eight questions that are the same in both SRS-24 and SRS-22r questionnaires were compared between patients and controls (questions one through eight in the SRS-24 and 1, 2, 4, 5, 6, 8, 9, and 11 in the SRS-22r).
Statistical analyses
The normal distribution assumption of the data was verified visually with QQ-plot and with the Shapiro–Wilk test. Descriptive statistics were presented in absolute numbers and percentages or in mean value with standard deviations (SDs). Statistical comparison of radiographic outcome data was performed with paired t-test. The comparison of preoperative or 6 months follow-up domain scores with 2 year follow-up scores were carried out with paired t-test. We applied the two-sample t-test assuming equal variances on the HRQOL domain scores to compare patients with healthy controls. For all analyses were conducted in JMP® for Macintosh, Version 16.1 (SAS Institute Inc., Cary, NC, USA, 1989–2021). p-values < 0.05 were considered statistically significant.
Ethical committee approval
The study received approval from the local ethical boards. Written informed consent was acquired from the patients and normative population and if needed from their guardians.
Results
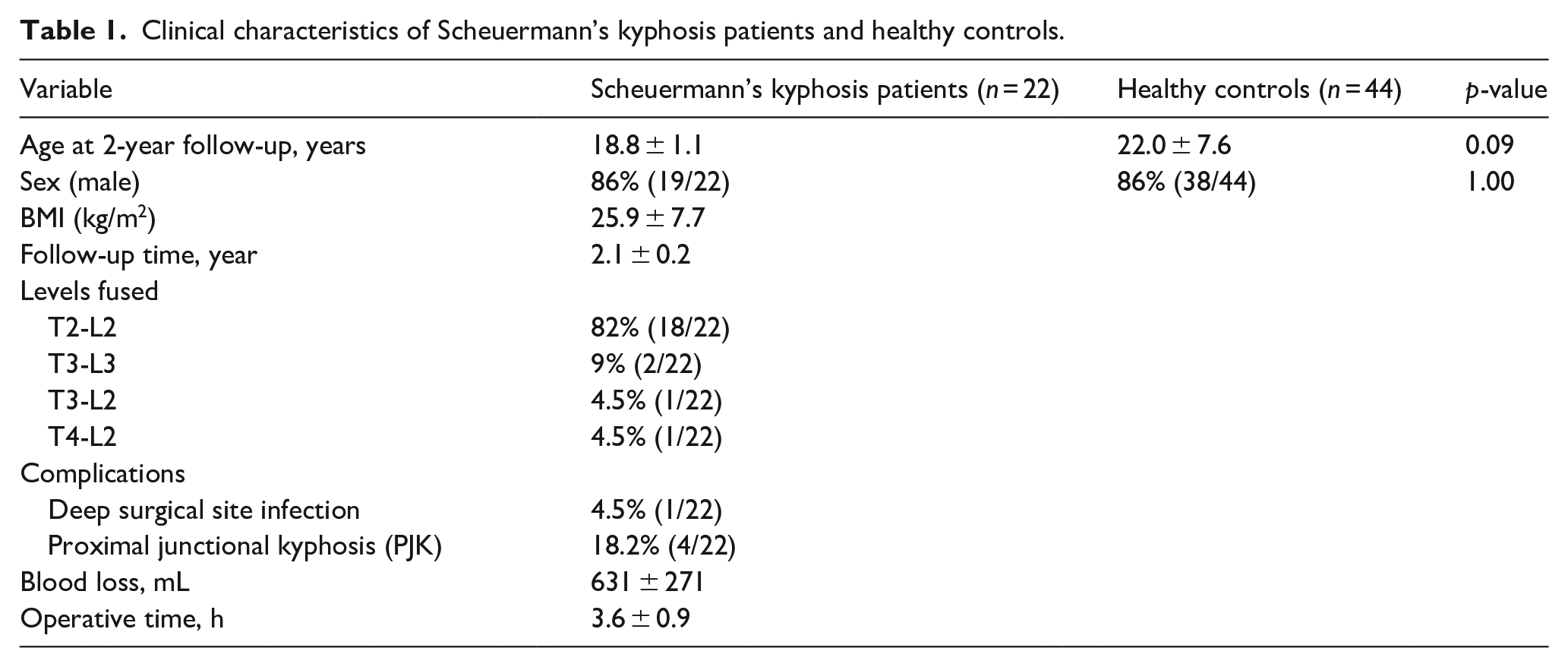
Twenty-two consecutive adolescents (mean age (SD) at the time of the surgery 16.7 years (1.3)), who were treated operatively for SK were included in this study. The mean body mass index was 25.9 (range = 16–40) preoperatively. The majority (82%) of fusion levels included T2-L2 (Table 1). The average length of surgery was 3.6 h (range = 2.75–7 h) and the average blood loss during the operation was 631 mL (range = 300–1450 mL). Median number of posterior column osteotomies was 4 (range = 2–7). In one patient, one pedicle screw was removed intraoperatively for a motor-evoked potetial (MEP) change in the spinal cord monitoring without neurologic deficit postoperatively. One patient underwent revision surgery for an acute deep surgical site infection.
Clinical characteristics of Scheuermann’s kyphosis patients and healthy controls.
Radiographic outcome
The mean maximal thoracic kyphosis improved from 79° (range = 75°–90°) to 55° (range = 45°–75°) (p < 0.001). The mean lumbar lordosis was reduced from 71° (range = 51°–107°) to 52° (range = 34°–68°) (p < 0.001) after 2 years of follow-up (Table 2). Kyphosis measured between T2 and T12 levels improved from 76° (range = 63°–88°) to 52° (range = 42°–68°) (p < 0.001). The mean PT changed from 7° to 9°, SS from 38° to 30°, and SVA from 13to 10 mm, during the 2 years of follow-up. These changes were not statistically significant. PI averaged 49° preoperatively and 44° at 2-year follow-up. There were no patients with significant PI—lumbar lordosis mismatch (>10°) at the end of the follow-up (Table 2).
Radiographic parameters of the Scheuermann’s kyphosis patients.
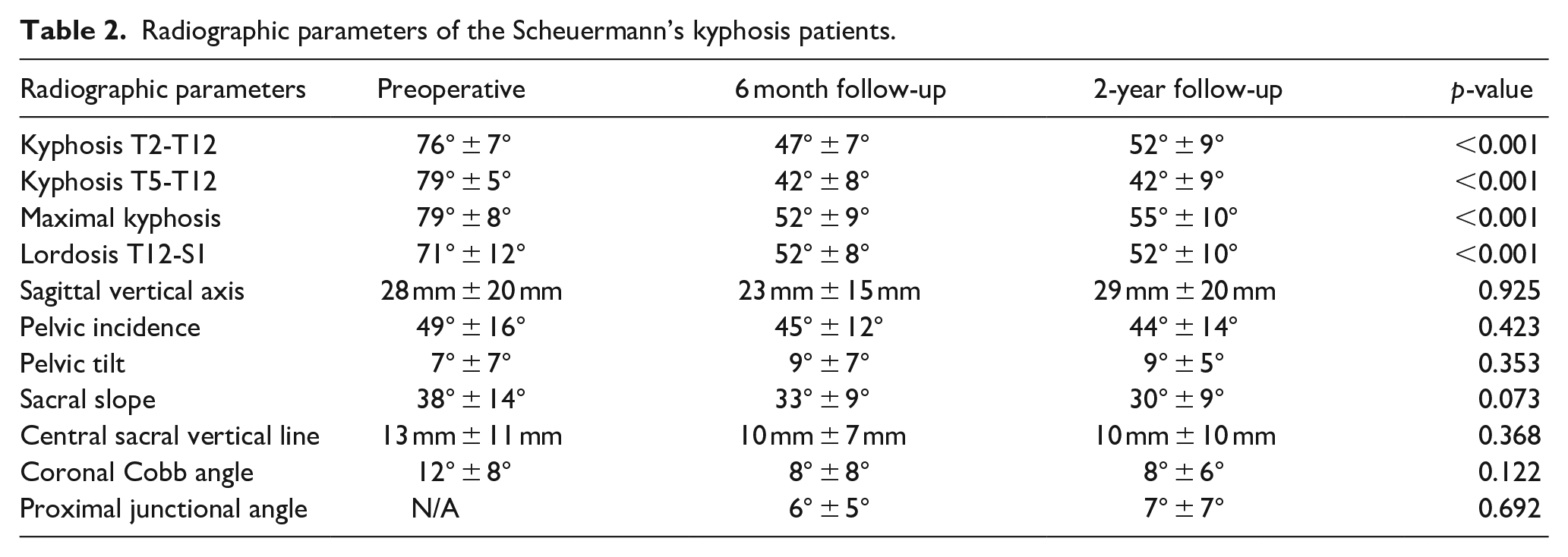
The mean coronal Cobb angle as measured from anteroposterior radiographs was 12° preoperatively and 8° at 2 years of follow-up. The CSVL was 13 mm preoperatively, and 10 mm postoperatively. These changes were not statistically significant. PJK incidence was 18% (4/22) after 2 years of follow-up and these patients were treated with observation only. The mean PJK change from 6 months to 2 years of follow-up was not statistically significant. PJK has remained asymptomatic in all patients and has been therefore addressed with continued radiographic follow-up only.
Health-related quality of life and comparison with healthy controls
Twenty-one (95%) patients completed the SRS-24 questionnaire preoperatively and twenty (91%) patients filled the same questionnaire at 2 years postoperatively. The scores of all domains of the SRS-24 questionnaire were higher after the 2-year follow-up (Table 3). The improvement was statistically significant in SRS-24 pain and self-image domains from preoperative to 2 year follow-up (p = 0.002 in both domains). The postoperative self-image, function and satisfaction domains improved from 6 months follow-up to 2 year follow-up. However, these changes were not statistically significant. The HRQOL of patients who had PJK did not differ significantly from other patients in any of the SRS domains at 2 years postoperatively. The radiographic correction of the deformity did not show any statistical correlations between the SRS questionnaire domains.
The changes in SRS-24 outcome questionnaire during the follow-up.
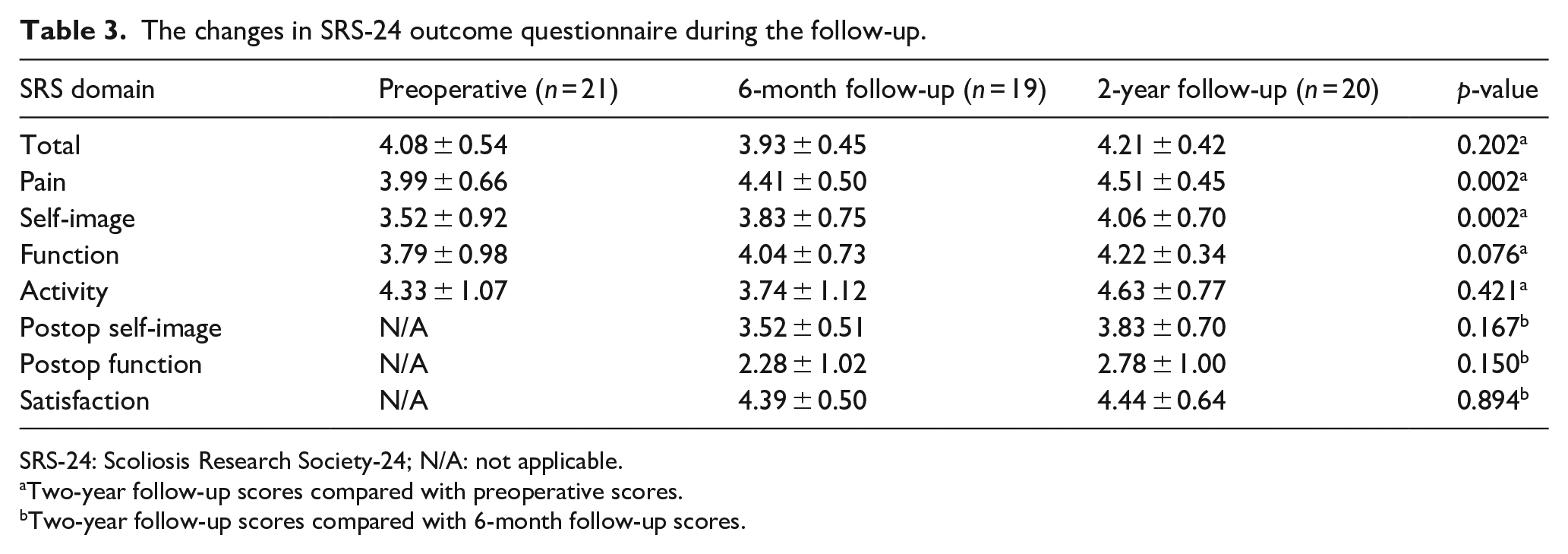
SRS-24: Scoliosis Research Society-24; N/A: not applicable.
Two-year follow-up scores compared with preoperative scores.
Two-year follow-up scores compared with 6-month follow-up scores.
Scores are mean values and SD.There was no statistically significant difference in the age between SK patients and controls (p = 0.09). The SK patients reached the controls in all SRS domains, except in self-image and function during the 2-year follow-up time (Table 4). The SRS scores for self-image and function remained significantly lower in the operated patients at their 2-year follow-up as compared with the age- and sex-matched controls (p = 0.023 for self-image and p < 0.001 for function).
Comparison of SRS outcomes between surgically treated patients and age- and sex-matched controls.
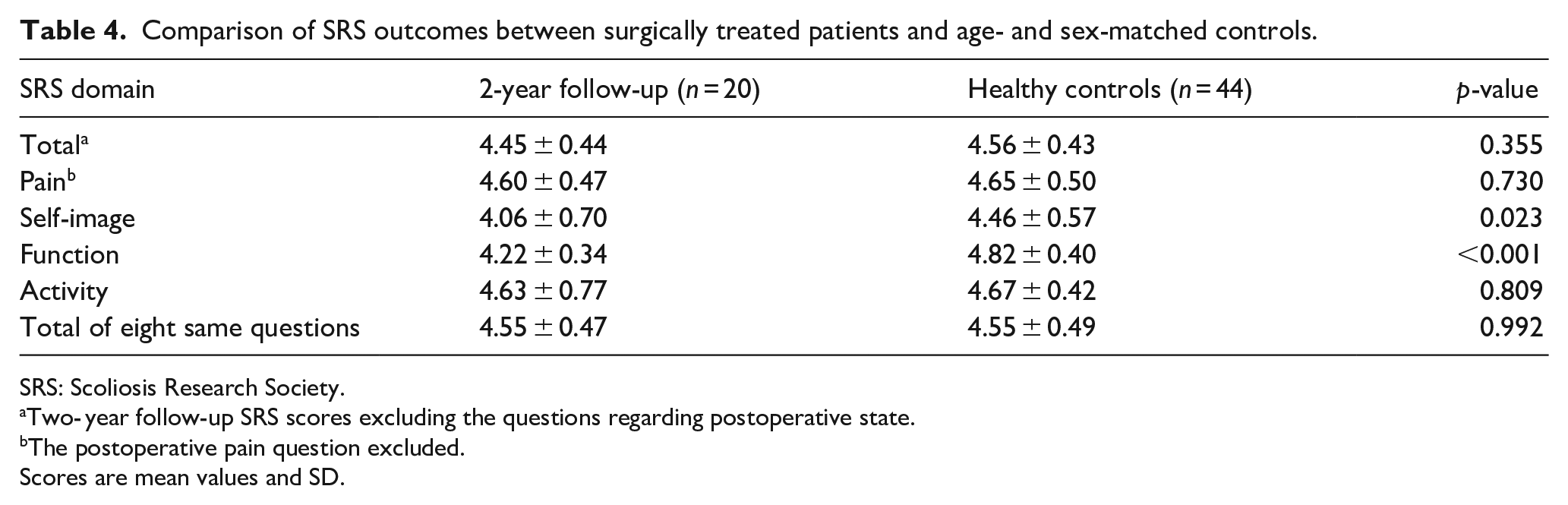
SRS: Scoliosis Research Society.
Two- year follow-up SRS scores excluding the questions regarding postoperative state.
The postoperative pain question excluded.
Scores are mean values and SD.
Discussion
To our knowledge, this is the first prospective study comparing the HRQOL of the operatively treated SK patients with age- and sex-matched healthy controls. This study shows that surgical treatment of SK significantly improves the HRQOL in pain and self-image domains in the 2-year follow-up, as measured with SRS-24 questionnaire. Pain and activity scores in patients with SK treated with posterior spinal fusion were comparable to those in healthy controls.
A significant improvement of thoracic kyphosis and lumbar lordosis was achieved in the surgical operation in this study. Variation in the operative time from 7 to 3 h represents the development of surgical practice and learning curve. Posterior-based instrumentation without vertebral column resection may not always provide satisfactory radiographic correction as shown by one patient with residual curve of 75 degrees. Despite the generally more limited radiographic correction of SK as compared with AIS, the patient reported satisfaction was on a relatively high level.
Our surgical technique has remained similar during this study period. Based on our earlier experience using either combined approach and/or vertebral column resection with even higher risk of PJK, longer operative time and neurologic risks of surgery, we believe that posterior pedicle screw instrumentation with apical osteotomies is good enough. This often results into satisfactory outcomes according to patient reported measures even if larger than normal radiographic kyphosis remains.
HRQOL data were missing from two patients at 2 years postoperatively. In these patients, the maximal kyphosis correction was from 77° to 55° and from 87° to 58°. The correction of lumbar lordosis was from 60° to 45° and from 61° to 39°, respectively. No complications occurred. Based on these results, we assume that the missing HRQOL data did not skew our results.
Previous results of operative SK treatment show similar improvement of radiographic parameters.8,12,14 PJK is the major instrumentation-related complication after the surgical correction of kyphotic deformities and its prevalence in operated SK patients is up to 30%.23,24 The prevalence of PJK was 18% in this study. All these four patients were treated conservatively and remained asymptomatic.
Patients with SK appear to have significantly lower preoperative scores in domains of the SRS-22 than patients with AIS or normal population. 12 Furthermore, Murray et al. 25 reached a conclusion that dissatisfaction with one’s appearance is greater in SK patients than in a control group of healthy subjects. Based on the previous research, surgical treatment of SK in the adolescent population results in significant improvements in HRQOL when measured using the SRS-22 outcome score.12,14,15
In 2018, Toombs et al. 14 studied the HRQOL in 82 surgically treated SK patients. The SRS-22 scores improved after surgery in all domains with the greatest change observed (2.8–4.4) in the self-image domain. In their study, a comparison of HRQOL data was made with surgically treated AIS patients. SK patients had significantly worse preoperative SRS-22 scores compared to the AIS group. At 2 years postoperatively, the HRQOL of SK patients improved to reach equivalent values to the AIS scores. Green et al. 15 compared 2-year radiographic and the SRS-22 results of 45 patients who self-selected either conservative or surgical treatment. At 2-year follow-up, surgical patients experienced a significant change on all parameters. exhibiting smaller Cobb angles, less pain, and greater satisfaction with their outcomes.
The minimal clinically important difference (MCID) for SRS-22r pain domain scores in adolescents has been reported at 0.20 and for activity domain scores at 0.08. 26 Data regarding the minimal clinically important values for the SRS-24 are lacking. In this study, the SRS-24 pain domain scores improved by 0.54 (95% confidence interval (CI) from 0.24 to 0.85) and activity scores by 0.16 (95% CI from −0.25 to 0.56) in the SK patients.
Limitations and strengths
Some limitations in this study need to be recognized. The SK is a relatively rare disease, and thus, the number of operated patients was relatively small. We did not compare our results with randomized controls for conservative treatment or natural history. One limitation of this study was the somewhat different questionnaires used (the SRS-24 and SRS-22r). We chose to keep the SRS-24 questionnaire in the surgical treatment group to provide data from preoperative to 2 years postoperatively. We used the 15 most similar preoperative questions from the SRS-24 and SRS-22r to provide comparable questionnaires, including eight questions that were the same. The results of SRS-24 and SRS-22r similar method have been compared previously in the similar manner.22,27 This study has several strengths. It is a prospective, single-center cohort study with consecutively enrolled patients. We used age- and sex-matched healthy controls. Same senior surgeon operated all the patients with an identical surgical technique (posterior spinal fusion with pedicle screws). The minimum follow-up time was 2 years. We assessed the HRQOL with widely used, validated, and standardized questionnaires.
Conclusion
In conclusion, the health-related quality of life and radiological measurements of SK patients improved after the surgery during 2-year follow-up time. The greatest improvement was observed in pain and self-image as measured with SRS-24 questionnaire. The scores in pain and activity reached the level of healthy control group, whereas the self-image and function remained significantly lower.
Research Data
sj-pdf-1-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-1-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-2-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-2-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-3-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-3-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-4-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-4-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-5-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-5-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-6-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-6-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Research Data
sj-pdf-7-cho-10.1177_18632521221106384 – Supplemental material for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls
Supplemental material, sj-pdf-7-cho-10.1177_18632521221106384 for Health-related quality of life outcomes in adolescent Scheuermann’s kyphosis patients treated with posterior spinal fusion: A comparison with age- and sex-matched controls by Eetu N Suominen, Antti J Saarinen, Johanna Syvänen, Elias Diarbakerli, Linda Helenius, Paul Gerdhem and Ilkka Helenius in Journal of Children’s Orthopaedics
Footnotes
Author contributions
All authors conceived and designed the study and participated in the acquisition of the data. E.S. analyzed the data and is the main author of the article. I.H. operated the patients. All authors contributed to critical article revisions. All authors approved the final version of the article and agree to be held accountable for the content therein.
Compliance with ethical standards
Ethical committee approval was obtained from Turku University hospital. Participants provided signed consent according to the Declaration of Helsinki. The article does not contain any studies with animals performed by any of the authors.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: I.H. has received institutional funding from Medtronic International, Stryker, and NuVasive. E.N.S. and A.J.S have received a research grant from Clinical Research institute HUCH. For the remaining authors, none were declared.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Medtronic International (grant no. ERP-2018-11372) and Stryker (Clinical Research Institute HUCH, project no. 20631).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.