
Abstract
Purpose
Little is known about the natural history of spinal deformities in Coffin-Lowry syndrome (CLS). Our goal was to evaluate the spinal deformity progression and clinical impact.
Methods
In this institutional review board-approved study, we performed a multinational retrospective review of six male CLS patients, aged 13 to 22 years at final follow-up, for a mean of 7.25 years (3 to 13).
Results
All showed delayed skeletal maturity. Three had calcifications of their lower cervical ligamentum flavum, all experienced neural axis abnormalities, including lower extremity weakness, numbness and tingling and in one, quadriparesis. Only two were ambulatory at final follow-up.
All had significant spinal abnormalities, including severe progressive thoracic lordosis, thoracolumbar kyphosis and scoliosis. All had undergone spinal fusion or were being evaluated for surgery.
Conclusion
CLS is a rare X-linked mutation in the RSK2 gene, affecting between 1/50 000 to 100 000 people. There are two reports in the literature of patients with calcifications of their ligamentum flavum. Both had neural axis abnormalities and one had acute onset quadriplegia. Analysis of their ligamentum flavum found abundant central calcifications. Despite our small cohort we found 50% had calcifications and 100% had neurologic consequences associated with those calcifications. There was a 100% rate of deformity progression.
They all exhibited delay in skeletal maturity, which mandates longer follow-up and has implications for surgical planning.
From our cohort and literature review, the natural history of CLS supports frequent patient evaluation and a lower threshold for correction of spinal deformities. Aiming to avoid spinal cord compression and improve or avoid neurological deterioration.
Level of Evidence
IV - retrospective study
Introduction
Coffin-Lowry syndrome (CLS) is a rare X-linked mutation in the RSK2 gene that affects between 1/50 000 to 100 000 people. The condition was first described in 1966 by Coffin 1 and in 1971 by Lowry 2 . The gene itself was identified in the mid-1990s and since then over 75 mutations have been identified in around 250 CLS patients. Male patients are more severely affected and carrier females are often only mildly affected due to X inactivation. 3 While it is an X-linked disorder, in 70% to 80% of cases it is due to a new mutation. 4 It is associated with severe developmental disability, characteristic facies, hypotonia, premature dental eruption, short stature, delayed bone age, hyperextensile doughy tapered fingers, pectus carinatum, pes planus and multiple spinal abnormalities.5,6
The aetiology by which the RSK2 mutation affects the musculoskeletal system is still unknown. This is due to the significant variability in RSK2 mutations which result in differing amounts of protein truncation and severity of phenotypic outcomes. Despite this uncertainty, progress is being made. RSK2 knockout mice have been found to have abnormal gliogenesis and neurogenesis, suggesting that the hypotonia may be due to the lack of differentiation of neural precursors.5,6 Furthermore, the osseous and collagenous abnormalities likely stem, at least in part, from RSK2's lack of phosphorylation and activation of ATF4 and CREB. ATF4 is a transcription factor which is an important component of osteoblast differentiation and gene expression. It is also an important component in the regulation of type-1 collagen synthesis and mutations in ATF4 are associated with delayed bone age. CREB ultimately results in the transcription of c-Fos, 5 which contributes to the differentiation of osteoclasts. C-Fos deficient mice closely resemble those with CLS. 6
Approximately 80% of male patients with the RSK2 mutations will have a spinal abnormality. Potential abnormalities include, but are not limited to, thoracic lordosis, scoliosis, kyphosis, degenerative disc disease and thoracolumbar kyphosis. The literature has reported that up to 47% of patients develop some degree of kyphoscoliosis. 7 In his review article on CLS, Hanauer proposed that the osseous changes in association with the ligamentous laxity may contribute to the progression of both the kyphosis and the kyphoscoliosis. 8 In 1990, Padley et al 9 described the radiographic findings associated with CLS. These included coarctation of the foramen magnum, narrowing of the intervertebral spaces, irregular endplates and anterior wedging. 10 These spinal abnormalities fall along a broad spectrum, but can be very severe. There are several case reports of rapidly progressive kyphosis and acute paralysis. This presents a significant problem and may dramatically shorten the life span of a CLS patient. Current literature reports life expectancy as a mean of 20.5 years. Cardiopulmonary compromise is a frequent cause of death and would be significantly affected by their progressive kyphosis.4,11
Unfortunately, little is known about the natural history or frequency of some of their spinal manifestations. Herrera-Soto et al's article in 2007 12 discussed their experience with ten CLS patients with spinal abnormalities, seven of which had kyphosis or kyphoscoliosis. Of these seven patients, four required surgical intervention. In other studies, both Hunter et al 4 and Miyazaki et al 13 had patients that developed significant calcifications of ligamentum flavum. Furthermore, Hunter's patient developed acute onset quadriplegia that had a waxing and waning course. His patient was 20 years old at the time of presentation and was found to have multilevel compression secondary to calcifications and hypertrophy of his ligamentum flavum as well as kyphoscoliosis. 4 Miyazaki's patient was 22 years old when he developed increasing difficulty ambulating, as well as evidence of cord compression. 13 He was subsequently found to have calcifications of the ligamentum flavum of his cervical and lumbar spine, though upon further review of his earlier imaging studies these were found to have been present on imaging studies since he was 14 years old. He subsequently underwent decompression and fusion and a sample of his ligamentum flavum was obtained. The sample was compared with those from an adolescent idiopathic scoliosis (AIS) patient and a CLS patient whose ligamentum flavum was not calcified. In addition to calcifications, Hunter et al 4 found an eight-fold and five-fold increase in the hexuronate content compared with the peripheral area of the CLS patient and the AIS patient with normal ligamentum flavum. Morino et al 7 analyzed ligamentum flavum removed at decompression in CLS patients and confirmed calcification (with calcium pyrophosphate and tricalcium phosphate crystals identified). This is quite concerning because, while it is not uncommon to develop calcifications, secondary to chondrocyte hypertrophys and shrinkage of the elastic fibres in the ligamentum flavum, this is primarily seen in the elderly, 13 tends to be more peripherally located and is thus less likely to cause cord compression.
Cases of calcification in the ligamentum flavum have been described with Mwaka et al 10 reporting on 28 non-hereditary cases; all had good results from laminoplasty. In CLS itself the calcifications are more localized – stretching from C2 to the upper thoracic levels – and more central. There has been no direct evidence to date that this calcification is due to genetic factors.
Materials and methods
This study was approved by the institutional review board of Shriners Hospital, Portland, Oregon. We performed a multinational retrospective chart review of six male CLS patients, aged 13 to 22 years at final follow-up, for a mean of 7.25 years (3 to 13). Information regarding the study was placed on the CLS Foundation website (http://clsf.info/) and participants’ parents contacted the corresponding author directly regarding participation in the study. Eight families elected to participate in the study, two were excluded due to incomplete records. Both of these excluded patients had scoliosis and had undergone surgical intervention. One of the two had developed central cord syndrome after a minor injury due to cervical stenosis. Both had moved home and were unable to provide their previous medical records or recall where the care had been provided. All families were provided detailed information regarding the study, and subsequently signed the appropriate consent forms and releases of medical records. The remaining six patients’ medical records and imaging studies were obtained, de-identified and were then reviewed; the patient's clinical outcomes, including surgical intervention, functional losses and motor or sensory losses were considered. Reviewers included a senior level orthopaedic resident (SF) and an orthopaedic spine consultant (MW). Both were blinded to clinical outcomes of the patients.
All patients had spinal abnormalities, including severe progressive thoracic lordosis, thoracolumbar kyphosis and scoliosis. All patients had either undergone posterior spinal instrumentation (four posterior instrumented fusions, one insertion of MAGEC rods (MAGnetic Expansion Control, Nuvasive, San Diego, California)) or were being evaluated for fusion at the time of final follow-up. Three patients had been braced without any evidence of improvement or slowing of the progression of their deformity.
Results
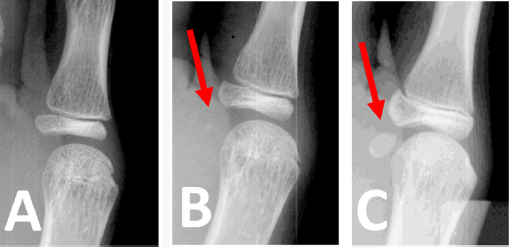
Delayed skeletal maturity and puberty was the rule, with only one patient achieving skeletal maturity at final follow-up. Three patients showed calcifications of their lower cervical ligamentum flavum (Fig. 1). These three patients were each experiencing neural axis abnormalities, including lower extremity weakness, numbness and tingling and, in the most profound example, acute quadriparesis. Two of the remaining patients had a significantly hypertrophied cervical ligamentum flavum, which could be considered a precursor to the calcifications. Four patients were ambulatory at final follow-up, two minimally so. Again, this highlights the importance of frequent clinical and radiological assessment in the setting of these spine findings. All patients also experienced varying levels of hypotonia.

Cervical spine axial CT scan demonstrating centrally located calcifications of the ligamentum flavum.
See Table 1 for a summary of the clinical, radiographic and surgical outcomes and Table 2 for a summary of the radiographic parameters at final follow-up.
Radiographic measures at final follow-up
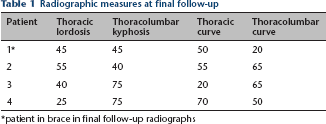
patient in brace in final follow-up radiographs
Summary of results
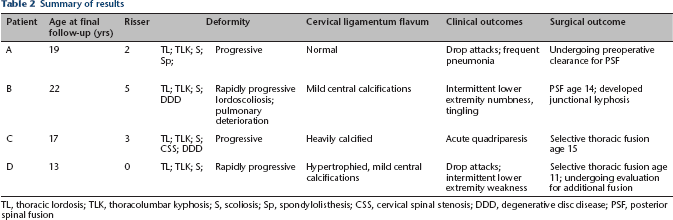
TL, thoracic lordosis; TLK, thoracolumbar kyphosis; S, scoliosis; Sp, spondylolisthesis; CSS, cervical spinal stenosis; DDD, degenerative disc disease; PSF, posterior spinal fusion
Discussion
Up to 80% of male patients with CLS will develop a spinal deformity. A significant number of these deformities will be severe and progressive. The deformity can worsen pre-existing cardiac and pulmonary compromise. It may cause neural axis abnormalities and in the most severely affected cases paralysis. Morino et al 7 reported an improvement in neurological function after early laminoplasty at just two weeks and long-term continued ambulation. Therefore, it appears that the detection and early treatment of these abnormalities is imperative. What remains to be determined is the time frame necessary for these interventions, especially considering the significantly higher morbidity and mortality associated with the treatment of spinal deformities in CLS.
Patients with CLS have significantly shortened lifespans. This is particularly true of male patients, who have a reported average lifespan of only 20.5 years. The vast majority of these patients’ causes of death will be secondary to either cardiovascular or respiratory complications. All patients with documented cases of cardiovascular causes of death were also suffering from panacinar emphysema.4,14
All of our patients had severe thoracic lordosis, thoracolumbar kyphosis and five patients had severe scoliosis (Figs 2 and 3). In our patient cohort, all deformities were progressive and 50% exhibited rapid progression. The progression of their thoracic lordosis alone may have a significant impact on both their quality of life and their lifespan, in terms of its effect on cardiac and respiratory function. Winter et al 15 found that thoracic lordosis in patients with AIS significantly impacted their pulmonary function. Multiple recent studies7,10,13 have shed light on the effect of these deformities on pulmonary and cardiac function. Bronchial torsion occurs as a result of thoracic kyphoscoliosis, 10 airway compression will occur with thoracic scoliosis, 7 and lordoscoliosis has been associated with both intrathoracic airway compression 13 and extrinsic bronchial obstruction. 7 Given the progressive nature of these deformities, more aggressive treatment earlier may lessen the pulmonary complications, improving life span and quality of life.
Anteroposterior and traction lateral radiograph of 11-year-old patient with severe thoracolordosis, thoracolumbar kyphosis and scoliosis.
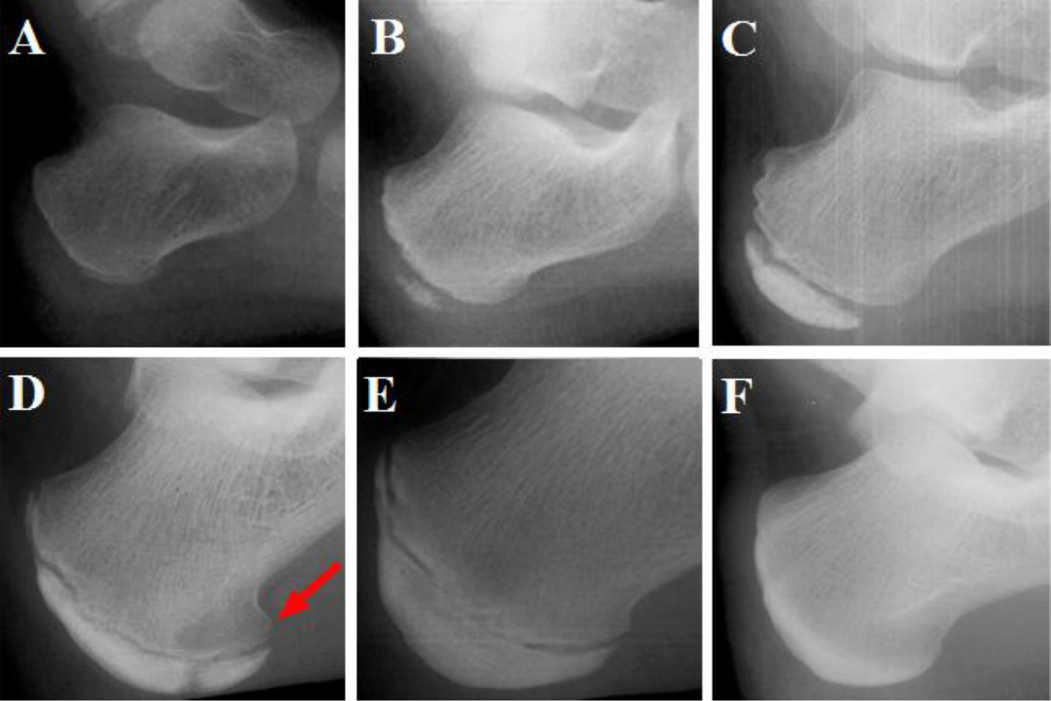
Lateral radiograph of 11-year-old patient with severe thoracic lordosis, thoracolumbar kyphosis and scoliosis six months after selective thoracolumbar fusion.
Prior to our study there were only two reports of patients 13 with calcifications of their ligamentum flavum. Both had neural axis abnormalities and one had acute onset quadriplegia with a waxing and waning course; 13 analysis of their ligamentum flavum found abundant centrally located calcifications. In our study we found that four (50%) of our patients had marked calcifications of the cervical ligamentum flavum (Fig. 1) and a further two patients (33%) had marked hypertrophy of the cervical ligamentum flavum. Interestingly these calcifications were visible on CT scans many years prior to the development of neural axis abnormalities. This could offer a useful indicator for closer follow-up and potentially earlier intervention. We found a 100% incidence of neural axis abnormalities in our patients with calcifications of the ligamentum flavum. The youngest had begun to experience marked lower extremity weakness and the oldest experienced acute onset quadriparesis; a devastating outcome for a CLS patient and for their families.
Lastly, another consideration in spinal surgery timing and in length of follow-up is their delayed skeletal maturity. This delay is the rule rather than the exception for CLS patients, with curves often progressing at older-than-anticipated ages, thereby mandating careful follow-up until skeletal maturity, which may be in the mid- to late-20s. Growth-sparing constructs may also be considered. Discussion with endocrine colleagues may be useful in defining skeletal maturity and planning surgical intervention.
Thus, the natural history of CLS is frequently one of spinal deformity progression and neurological compromise. Therefore, earlier and more aggressive correction of spinal deformities and decompression - especially when ligamentum flavum calcifications are identified - should be recommended. The aim is to avoid deterioration in cardiac and pulmonary function in the more severe spinal deformities and to reduce neural axis abnormalities and, in the worst cases, quadriplegia. This will serve to both improve quality of life and life expectancy in CLS patients.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Acknowledgments
We would also like to acknowledge the information obtained from the Coffin-Lowry Syndrome Foundation who provide excellent information and support to families and medical professionals alike.