
Abstract
Purpose:
Pediatric forearm fractures are a common presentation to Accident and Emergency departments. Standard treatment for the majority of these is manipulation under sedation within the department, followed by cast application. Concerns have been raised about the acceptability of such interventions, and reluctance to perform these procedures has led to increased admissions and manipulations performed under general anesthetic.
Methods:
A prospective case series of all pediatric patients with forearm fractures who underwent a manipulation under sedation in the Accident and Emergency department was collected over 12 months. All parents were invited to complete an acceptability questionnaire, adapted from the Swedish Pyramid Questionnaire for Treatment, based on their experiences.
Results:
A total of 77 patients were included and their parents were asked to complete a Swedish Pyramid Questionnaire of Treatment. Forty-four parents (55%) agreed to fill out the questionnaire. Patient demographics and fracture characteristics were compared between the group that responded and those that did not, with no significant differences. Average level of satisfaction was 9.4/10 (range = 7–10). 98% of respondents were satisfied with the level of analgesia provided, but only 86% with the timeliness of administration.
Conclusion:
This parent-focused evaluation of treatment confirms high levels of parental satisfaction with the management of pediatric forearm fractures in Accident and Emergency, with regard to care, analgesia, and information. It provides insights about parental concern relating to the injury and their anxiety as information useful to further improving care, a template for assessing quality improvement and should be considered as part of further studies in this field.
Level of evidence:
Level IV case series.
Purpose
Fractures are common among pediatric patients. Approximately 20%–30% of all children will attend Accident and Emergency (A&E) in the United Kingdom each year, do so with an injury.1,2 Approximately 9% of these attendances will be associated with a fracture,3,4 an estimated 300,000 individuals. The majority of these fractures occur in the upper limb, 5 with the majority occurring in the distal radius (approximately 25%) 6 and forearm mid-shaft (9%). 7
Closed reduction and immobilization in a cast is accepted as the standard treatment for a proportion of these cases.8,9 The majority of children requiring manipulation in recent times were admitted to hospital for this management. There was evidence of varied practice in that some hospitals were admitting less and manipulating some fractures in A&E in the previous decade.10,11 This has culminated in manipulation of suitable fractures in A&E becoming an established standard of care with guidance published as a Standard for Trauma care in the United Kingdom by the British Orthopaedic Association in conjunction with the Royal College of Emergency Physicians in 2020. 12
Fractures in children can be treated differently to equivalent injuries in adults due to their high potential for remodeling. This means that displacement and/or deformity considered unacceptable in an adult patient is potentially acceptable in a pediatric one. 8 Remodeling potential decreases with age, and so degree of displacement becomes more adult orientated as a child ages.8,9,13,14
Adequate analgesia is essential prior to manipulation of such fractures, and centers differ in their protocols. 15 Opiate analgesia, procedural sedation, hematoma or Bier’s blocks have all been advocated,10,11,15–18 but evidence behind the choice is limited. BOA Standards for Trauma and Orthopaedics (BOAST) guidelines recommend: “procedural analgesia and sedation,” allowing units to produce local protocols that suit their requirements and the skillset of the hospital.
A study of pediatric fractures in a hospital in the United Kingdom recorded an average waiting time for formal admission is often greater than 8 h, and average time from admission to discharge is over 21 h. 19 Successful reduction of such fractures in A&E results in comparable clinical outcomes, far more quickly and represents greater convenience for patients and parents as well as potential cost-savings to the hospital.20,21 The average cost of a pediatric patient undergoing manipulation and casting in theater is £554, compared to £56 for the same treatment and discharge from A&E, a near 10-fold increase. 22
We aimed to assess the acceptability of pediatric forearm manipulation in the A&E in a district general hospital, using a parental-related satisfaction tool, which is the first review of this type for this patient group, as far as we are aware. Although patient satisfaction is an accepted indicator of quality of care, this is difficult to assess in younger pediatric populations, and we therefore used parental satisfaction as a surrogate measure, based on experience from other pediatric interventions. 23
Methods
Ethical approval was sought from our local Research and Development department. All patients between the ages of 4 and 16 years who presented to the Emergency Department over a 12-month period from 2019 and 2020 with an injury of the forearm were initially included. Only patients with an isolated, closed injury of one or both forearm bones who went on to have a manipulation with casting in the A&E were included in this study.
Exclusions were patients with polytrauma, physiological instability, and of whom concerns regarding non-accidental injury had been raised were excluded. Patients with undisplaced fractures, segmental fractures, open fractures, or fractures associated with dislocations (Galleazzi and Monteggia variants), patients whose parents did not consent to manipulation, and lack of an appropriate A&E doctor to provide analgesia or sedation in the Emergency Department were also excluded.
The management of the patients in the study group was as follows: once patients were clinically assessed, and had orthogonal radiographs of the affected limb. Pre-reduction fracture characteristics including position of fracture and angle of deformity in the sagittal and coronal plane were recorded. The decision to manipulate was made by the on-call Trauma and Orthopedic Registrar based on patients age, fracture characteristics, and with consent from patient, parents, and A&E staff.
The choice of analgesia and/or sedation was made by the A&E team, and the manipulation and casting was undertaken by the Trauma and Orthopedic team. Six different registrars performed the manipulation and casting procedure over the data collection period. Parents were invited to be present during the procedure, but were fully informed about what to expect. Several declined, and waited in a waiting room until the reduction procedure had been completed. Analgesia and sedation varied between patients, but included strong opiates generally fentanyl or diamorphine; entonox; hematoma blocks and ketamine sedation, the choice of which was dependant on the A&E clinician.
Post-reduction orthogonal radiographs were taken and fracture characteristics were recorded for comparison. A reduction was considered “successful” if the patient did not require further manipulation.
The parents of all identified, included patients who had a manipulation and casting in A&E were invited to complete a Swedish Pyramid Questionnaire of Treatment (SPQT) and provided with a stamped return envelope. The questionnaire had no patient-identifiable information, and was collated into a spreadsheet using unique identifiable numbers. Consent was sought from all respondents. The SPQT has been adapted for the parents of pediatric patients undergoing treatments including surgical interventions and medical procedures such as lumbar punctures and day case infusions. It has been found to have high reliability and validity. 24 The SPQT includes a total of 45 questions which covers a wide range of parents’ perceptions of their child’s health status at time of presentation, parental anxiety levels as well as covering topics of information relating to the patients’ presenting condition, hospital routines, accessibility to healthcare, the medical treatment, the caring process, staff attitudes, participation in the health process, staff work environment, and overall satisfaction. As far as we are aware, it has never been used to assess the management of fractures in A&E.
Results
Demographics and fracture types
A total of 77 patients met the inclusion criteria and parents were invited to complete the SPQT. A total of 42 responses were received, a 55% response rate and forms the principle study cohort.
Of the parents who responded, the average age of their child was 10 years (range = 3–16) and 31 (73%) of the patients were male. Regarding fracture characteristics, 24 (57%) had both bone forearm fracture, 13 (31%) patients had isolated radius fracture, and 5 patients had an isolated ulna fracture (12%). Four (10%) patients had distal radius Salter–Harris type fractures of the radius. Twenty-seven patients (64%) had fractures in the distal part of the forearm, and 15 (38%) had mid-shaft fractures, and 11 (26%) patients had off-ended fractures. There were no significant differences in the patient demographics or the fracture characteristics between the respondent and non-respondent groups. Of those patients who did not receive initial manipulation and casting in the A&E department, 24 patients (60%) met the inclusion criteria according to the BOAST Guidelines for this treatment, but did not receive it due to non-medical reasons.
The methods used for analgesia and sedation are summarized in Table 1. Simple analgesia such as paracetamol and ibuprofen was given as baseline, usually soon after initial triage.
Analgesia and sedation used in 45 A&E pediatric forearm closed manipulations.

Choice of analgesia and sedation was administered at the discretion of the A&E team with input from the Trauma and Orthopedic team. There was no specific protocol in place. In combination, 35 patients (83%) received paracetamol, 29 (69%) received ibuprofen, 22 (52%) were administered diamorphine, 10 patients (24%) had oramorph, and 31 (74%) patients were given entonox. Three patients (7%) were given ketamine sedation, and three patients (7%) had a hematoma block with 2% lidocaine.
A&E manipulation outcomes
Thirty-four patients (80%) of the respondents’ children had a satisfactory reduction without the need for further surgery, compared to 30 (85%) in the non-respondent group.
Key survey results
On presentation, 9% (n = 4) of parents considered their child’s health status to be “seriously ill,” 43% (n = 18) “somewhat ill,” 43% (n = 18) “not seriously ill,” and 5% (n = 2) “not ill at all.”
With regard to parental anxiety about the patient’s wellbeing at time of presentation, 14% (n = 6) of parents “Were, to a great degree,” 62% (n = 26) “Were, to a certain degree,” 14% (n = 6) “Were not especially,” and 10% (n = 4) “Were not at all.” In terms of medical treatment, 98% fully or mostly agreed that their child received adequate analgesia, although this dropped to 86% agreeing or mostly agreeing this was delivered in a timely fashion. There was 100% confidence in staff skills and 96% satisfaction for the caring metrics.
When asked “On a scale of 1–10 with 10 being completely satisfied, how satisfied were you with your experience of the manipulation of your child’s fracture in A&E,” the mean satisfaction rating was 9.4 (range = 7–10). The number of responses to all of the questions on the SPQT can be found in Table 2.
Responses to the SPQT.
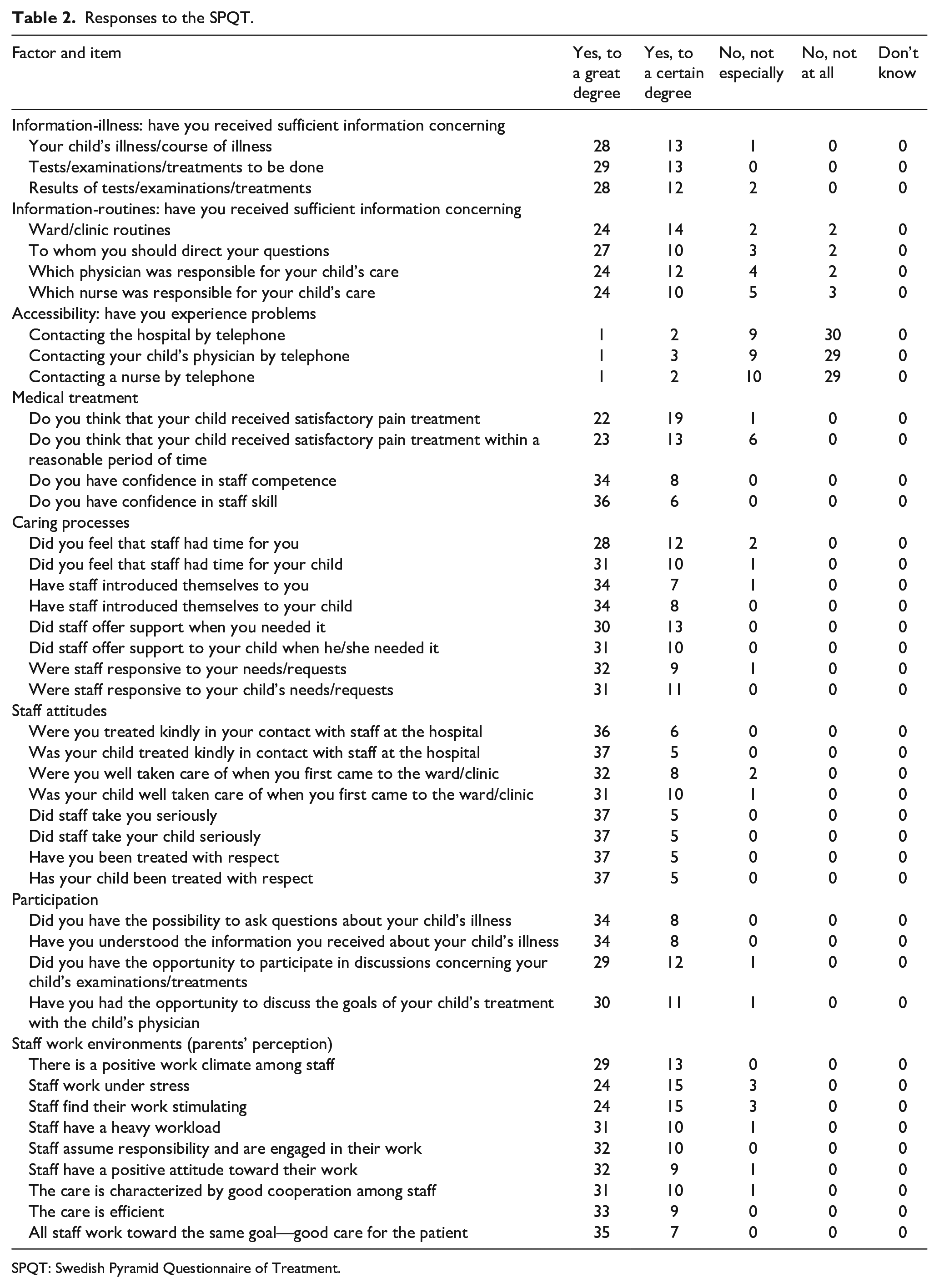
SPQT: Swedish Pyramid Questionnaire of Treatment.
Discussion
We achieved a response rate comparable with other studies that utilized mail questionnaires24,25 with additional repeat reminders and opportunities to participate at follow-ups also used.
It is interesting to observe the distribution of parental recognition of their child’s illness as well as their anxiety levels, as these produce the widest disparities of all of the response stems. It shows that while the vast majority of parents recognized that their child had an injury, with 95% considering their child to be seriously, somewhat, or not seriously ill, 5% felt their child not ill at all. The wording of this question may have been slightly misleading such that some parents may have considered “illness” and “injury” were different things, and answered the question more literally. In future questionnaires, adapting this language may be beneficial. There was a similar degree of variation with regard to parental concern, although with the largest group being the 62% concerned to some degree, with smaller proportions being very concerned and again 5% having no concerns at all.
The treatment and care sections showed far greater consensus, and with particular relevance to an A&E procedure was that 52% of respondents strongly agreed that their child had adequate pain relief and a further 45% of parents agreed to a certain degree. This was despite the variety of analgesia and sedation used in A&E during the study period. While ideally 100% of respondents would have strongly agreed that their child had adequate pain relief, this study suggests that regardless of the choice of analgesia and sedation used to manipulate these fractures, the majority of parents felt that it was adequate. We can infer that this was because the choice of method was tailored to suit the patients’ needs, whereby more analgesia and sedation were used for those who required it.
There was more variation in the perception of timeliness with regard to pain relief delivery, which provided the most variation in responses after illness severity and parental anxiety. Although the majority of patients’ parents (85%) felt that the patient received satisfactory pain relief within a reasonable period of time, 15% of respondents did not. There is some ambiguity in the question, and it is assumed that parents will regard this question being in relation to the time from presentation at hospital to receiving analgesia. It is possible that this finding represents increased operational pressures in A&E and worsened over the study period, but which is an important finding for targeting future improvements in the care of this patient group.
Encouragingly, all parents agreed that they had confidence in both staff competence and skill. With regard to perception of staff work environments, all parents felt that there was a positive work climate among staff and that staff assume responsibility and are engaged in their work. All parents felt that the care was efficient, and that all staff worked toward the same goal—good care for the patient. Of some concern, 93% of respondents felt that staff worked under stress, and 98% felt that staff had a heavy workload. This is another important finding from this study.
The key strength of this study is the utilization of a comprehensive parent completed validated questionnaire for the management of pediatric fractures at a time where there is concern and some degree of controversy as to which patients are best treated in an A&E setting, how they are best treated in terms of analgesia and/or sedation, and the patient related early outcomes of these types of treatment. We were able to achieve similar response rates of a consecutive series of patients, with no differences in demography or outcomes noted between parents who responded and those who did not. In addition, keeping the questionnaire anonymous encouraged parents to give an honest assessment of their experiences within A&E. This can be an issue when a participant is concerned about being treated unfavorably based on a critical response. The limitation of this is that we were not able to analyze for any patterns in differences in responses, with injury or analgesia factors. The proportion of non-responders clearly leaves some element of doubt that there were differences in satisfaction between those who completed the questionnaire and those parents who did not. Other weaknesses are that we were unable to define within the exclusion groups, the precise numbers of patients whose parents refused treatment or times when the department was too busy to undertake manipulation. These weaknesses and the small nature of this project could clearly be addressed by undertaking it for a similar amount of time as a multi-center prospective study.
In conclusion, this parent-focused evaluation of treatment confirms high levels of parental satisfaction with the management of pediatric forearm fractures in A&E, with high levels of satisfaction relating to treatment, care and information provided as well as providing insights into parent’s observations of how busy the service is. It provides insights about parental concern relating to the injury and their anxiety as information useful to further improving care, a template for assessing quality improvement and should be considered as part of further such studies in this field.
Footnotes
Author contributions
J.K. contributed the design, data collection, analysis, and first draft of the paper. S.D. provided the supervision, guidance, and revision drafts of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All patients returned informed consent as part of the questionnaire process.
Institutional review board
This study is registered with institutional R&D department.
Research involving human participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. No concerns identified regarding this study.