
Abstract
Purpose
Open fractures are considered an orthopaedic emergency and are generally an indication for operative debridement. Recent studies have questioned this approach for the management of Gustilo-Anderson Type I open fractures in the paediatric population. This meta-analysis studies the non-operative management of Type I open paediatric forearm fractures.
Methods
An Ovid MEDLINE and PubMed database literature search was performed for studies that involved a quantified number of Gustilo-Anderson Type I open forearm fractures in the paediatric population, which were treated without operative intervention. A fixed-effect meta-analysis, weighting each study based on the number of patients, and a pooled estimate of infection risk (with 95% confidence interval (CI)) was performed.
Results
The search results yielded five studies that were eligible for inclusion. No included patients had operative debridement and all were treated with antibiotics. The number of patients in each study ranged from 3 to 45, with a total of 127 paediatric patients in the meta-analysis. The infection rate was 0% for all patients included. The meta-analysis estimated a pooled infection risk of 0% (95% CI 0 to 2.9).
Conclusions
The five included studies had a total of 127 patients with no cases of infection after non-operative management of Type I open paediatric forearm fractures. The infection rate of Type I fractures among operatively managed patients is 1.9%. The trend in literature towards non-operative treatment of paediatric Type I open fractures holds true in this meta-analysis.
Introduction
Open fractures are considered an orthopaedic emergency due to the potential for infection.1–5 Open fractures only comprise 2% of paediatric fractures.6,7 The standard of care for open fractures generally includes antibiotics and formal debridement in the operating room.8,9 This management decreases the risk of infection by decreasing the bacterial burden and removing devitalised tissue.3,4 The infection rate of Type I fractures among operatively managed patients is 1.9%. 10 It is generally accepted that open paediatric fractures have better outcomes than adults, but there is a call for high quality studies to explore this further.3,8,9,11,12 However, the management of Gustilo-Anderson Type I fractures in the paediatric population is controversial, with recent studies questioning the utility and cost-effectiveness of this approach. 3 The theory behind this approach lies in the fact that while there may be some soft-tissue damage associated with all Gustilo-Anderson Type I open fractures, these fractures generally have preserved blood supply to the injured area resulting in less soft-tissue ischemia, oedema and necrosis that could promote infections. 10 Operative intervention is associated with the risks of anaesthesia, damage to neurovascular structures and increased cost associated with surgery.3,9,10,13,14
Several recent articles have published data on the non-operative treatment of open paediatric forearm fractures.3,9,10,15,16 The published results demonstrate a nearly universal degree of success in achieving low infection rates with non-operative management. The treatment protocols proposed vary, but each includes non-operative debridement and irrigation in the emergency department and antibiotics. These fractures are typically closed reduced, immobilised and discharged for outpatient follow-up.
For this meta-analysis, we have examined available data regarding Gustilo-Anderson Type I fractures of the forearm in paediatric patients managed non-operatively. 5 To our knowledge, this study provides the largest collection of data on this topic.
Methods
The Gustilo-Anderson classification of open fractures characterises the soft-tissue injury based upon the size of the skin defect and the extent of soft-tissue damage. Specifically, Type I injuries have a 1 cm or less skin defect and are typically lower energy injuries.
A literature search was performed using the Ovid MEDLINE and PubMed databases. The search terms ‘open fracture’, ‘pediatric’, ‘forearm’ and ‘treatment’ were used. Articles were limited to English-language published peer-reviewed articles without date limitations. Only randomised controlled trails, cohort studies and case-control studies were included in the meta-analysis. Inclusion criteria were set to include studies that investigated outcomes after non-operative treatment of Type I open fractures of the forearm in the paediatric population. Once results were gathered based on search terms, studies were first reviewed based on title, abstract and results. The studies were further narrowed to a subset that authors deemed to fit inclusion criteria for full text review. Following evaluation, the citations of eligible studies were also reviewed for additional studies that might fit inclusion criteria.
The authors reviewed the full text of the included studies and extracted and recorded relevant data into a spreadsheet, including study identification (e.g. authors, journal, publication date), total number of patients included in the study, total number of forearm fractures included in the study, mean age, age range, gender, IV antibiotic use, oral antibiotic use, infection rate and complication rate.
For each study, the number of paediatric patients with non-operative treatment of a Type I open forearm fracture were counted, and the percentage of those patients with a post-operative infection was calculated, including the 95% confidence interval (CI) of that percentage based on an exact binomial distribution. The authors then performed a fixed-effect meta-analysis, weighting each study based on the number of patients, and a pooled estimate of infection risk (with a 95% CI) was calculated.
Results
The search results yielded 1148 publications. These results were reviewed based on title and abstract to yield 17 publications, which fit the study criteria. The full text of these 17 publications were reviewed and five of the papers were deemed eligible for inclusion (Fig. 1).3,9,10,15,16 These five studies included four retrospective cohort studies as well as one prospective cohort study; all five studies investigated outcomes after non-operative treatment of Type I open fractures of the forearm in the paediatric population. The excluded publications included studies in which all study participants received operative treatment of their open fractures, as well as review articles that were not independent studies. The included studies ranged in size from three to 45 patients and collectively included 127 paediatric patients with a Type I open forearm fracture. All included patients were treated with antibiotics (i.v. or oral) without formal open debridement and irrigation in the operating room.
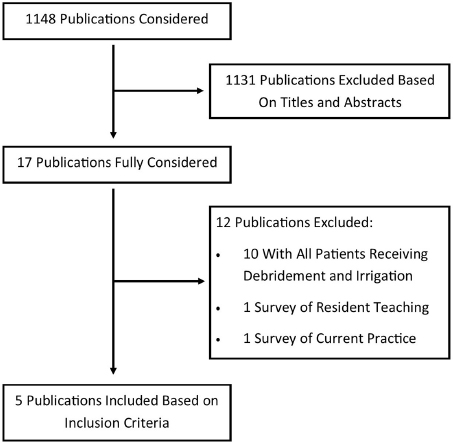
Flow diagram representing literature search and study inclusion.
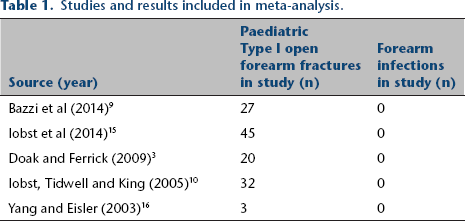
There were no cases of infection after non-operative treatment of the forearm fractures in the five studies examined, giving all individual studies an infection rate of 0% (Table 1). Three patients did undergo an operative treatment for loss of reduction of the forearm fracture, but did not experience infections after the initial non-operative treatment. There were two cases of infection after non-operative treatment of Type I open tibia fractures in these studies, but these results were not included in the meta-analysis calculation. Results of the meta-analysis estimate a pooled infection risk of 0% (95% CI0 to 2.9) and are shown in Figure 2.
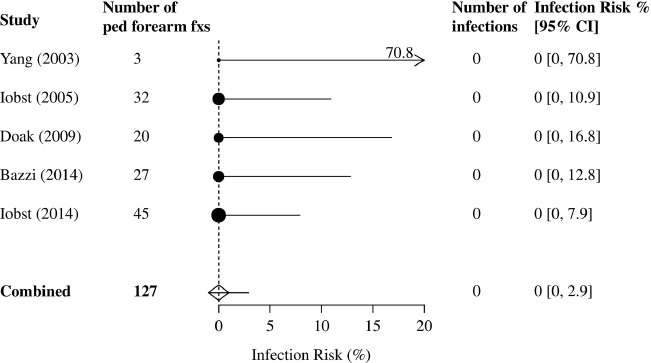
Forest plot of included studies.
Studies and results included in meta-analysis.
Discussion
To our knowledge, this meta-analysis is the first such review to analyse non-operative treatment of open paediatric forearm fractures and, to our knowledge, provides the largest collection of data on the topic. With a total of five included studies and a patient pool of 127 paediatric patients, there is no difference in the risk of infection for non-operative management of open paediatric forearm fractures compared with operative management. The infection rate of Type I fractures among operatively managed patients is 1.9%. 10 The trend in the literature towards non-operatively treatment of paediatric Type I open fractures holds true in this meta-analysis.
There are unique characteristics of Type I forearm fractures and paediatric populations that enable non-operative treatment. Compared with more severe grades of Gustilo Anderson open fractures, Type I fractures have small defects with minimal contamination. A common mechanism for this skin defect is an ‘inside-out’ puncture wound caused by a fragment of bone. 9 While all open fractures, including Gustilo-Anderson Type I open fractures, are associated with some degree of soft-tissue injury, Type I open fractures are more likely to have preserved blood supply to the injured area. 10 Since devitalised soft tissue can be a nidus for infection, the lack of soft-tissue damage may factor into a lower rate of infection. Some authors also point out differences in apparent infection risk based on the location of the Type I open fracture. Some of these authors report high risk of infection in lower extremity fractures.3,10,13 This could be the result of less soft tissue overlying the tibial shaft and ankle translating into a higher risk of infection. Finally, the thick, richly vascularised periosteum of paediatric patients allows for enhanced immune response, perfusion and antibiotic delivery to the fracture site. These factors provide an ideal environment for rapid healing and decreased risk of infections, giving paediatric patients a more favourable outlook for non-operative treatment of fractures.
In performing our analysis, we acknowledge several limitations. Our review focuses on Gustilo-Anderson Type I injuries, those typically involving low-energy trauma with limited fracture site contamination. Our results are not applicable to high-energy or grossly contaminated injuries classically treated with emergent operative debridement and irrigation. Our analysis is further limited to paediatric forearm fractures and we note that the studies analysed included two cases of infected tibial fractures. We acknowledge that there may be a greater risk of infection in fractures at body sites other than the forearm, potentially related to differences in soft-tissue coverage or to mechanisms of impact. Our literature and database search was thorough and used our best efforts to locate applicable studies; however, a meta-analysis has the possibility of publication bias. Similarly, the accuracy of a meta-analysis is dependent on that of the individual studies analysed; we did not observe apparent bias in the studies discussed here, but cannot exclude the possibility of error on an individual basis. The sample size of the included studies was limited, ranging from three patients to 45 patients. Finally, we note that in each of the studies analysed here, it was impossible to blind the patients and physicians to the treatment utilised.
Future research will be valuable in the area of non-operative treatment of open fractures. A randomised controlled trial is needed to further elucidate the treatment; such a trial is already underway. 17 Obtaining and analysing a larger patient pool may provide a compelling conclusion regarding appropriate treatment and would also begin to elucidate other potential factors for infection or complication of Type I fractures.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding was received for this study.
MS reports he is a paid consultant for Orthopaediatrics. All other authors have no conflicts of interest to declare.