
Abstract
Background:
Routine family planning data in South Africa are managed using a routine health information system, which facilitates data collection, storage, processing, presentation and dissemination. Healthcare providers generate data daily as they carry out their duties. The information generated should be used for planning and evaluating health program performance and policy development.
Objective:
To explore the use of family planning information by primary healthcare (PHC) clinic managers in South Africa.
Method:
A qualitative descriptive exploratory study was carried out in 11 PHC clinics in Tshwane District. Individual semi-structured interviews were conducted with 11 clinic managers. The data were analysed using a thematic analysis approach.
Results:
Managers used the information to disseminate performance and feedback, monitor the program’s performance and make decisions to improve the family planning service. However, they experienced challenges that hampered the effective use of the information.
Conclusion:
The use of family planning information is critical for improving the performance of the program. The clinics need sufficient skilled healthcare providers who are able to provide comprehensive family planning and generate accurate and reliable information that can be used to improve the service. Collaboration between the private and public sectors is critical in monitoring the program’s performance.
Keywords
Introduction
Access and use of family planning methods are crucial in preventing maternal mortality caused by pregnancy-related risks. One of the Sustainable Development Goals for 2030 is to ensure “universal access to sexual and reproductive healthcare services, including family planning” (Starbird et al., 2016; United Nations, 2018). To measure access and utilisation of family planning, the proportion of women aged 15–49 who use family planning methods is assessed (United Nations, 2018). Measuring the utilisation requires a health information system (HIS) that can generate valuable information for decision-making.
Numerous Asian and African countries, including South Africa, use the routine health information system (RHIS) to collect, analyse and present data needed to measure and track family planning’s performance (Anwar et al., 2015; Seitio-Kgokgwe et al., 2016; Wright et al., 2017). The RHIS is a primary monitoring system used at the institutional level to collect data regularly to meet anticipated information requirements (Afe et al., 2018). Its fundamental function is to produce high-quality, relevant and trustworthy data that can be transformed into information necessary for evidence-based decision-making regarding health system interventions, program implementation and monitoring and policy formulation (Afe et al., 2018; National Department of Health Republic of South Africa, 2011).
Several studies have reported low utilisation of information, despite its importance. Low utilisation was attributed to poor quality data in Ethiopia (Tilahun et al., 2021). In Palestine, Ethiopia, Kenya and South Africa, health institutions primarily used information for reporting to the district level, providing feedback to staff, monitoring program output and displaying information. The information was not used for planning and decision making (Cheburet and Odhiambo-Otieno, 2016; Mimi, 2015; Nicol et al., 2017; Wude et al., 2020).
In contrast, other studies in Botswana, Ethiopia and Nigeria discovered that routine health information was used for planning health services, managing supplies, budgeting and developing policies. However, most of the studies were conducted at the district, provincial and national levels, with only a few focusing on family planning (Afe et al., 2017; Dagnew et al., 2018; Ohiri et al., 2016; Seitio-Kgokgwe et al., 2016).
In South Africa, data are collected and aggregated by healthcare providers, captured into the district health information system (DHIS) software, the National Department of Health data management software by data captures and transmitted to the district level (Department of Health South Africa, 2012). At the district level, the data are analysed to produce information about the family planning program’s performance using the couple-year protection rate (CYPR) indicator. The CYPR indicator is used to estimate the proportion of women protected from pregnancy over 1 year by using family planning methods (Massyn et al., 2020). The district provides feedback to clinics and reports to the province, which reports to the national health department (Department of Health South Africa, 2012).
Considering the significance of family planning in reducing maternal mortality, it is vital that the information generated is utilised from the point of care and continues throughout other levels of care. Clinics should utilise these data for daily facility management, decision making and improving reproductive health program’s. Clinic managers have a responsibility to manage data, implement remedial actions and enhance the performance of family planning program’s (Department of Health South Africa, 2012). As such, it is critical to understand how managers use family planning information and the challenges they face. This study aimed to explore how primary healthcare (PHC) clinic managers in South Africa utilise family planning information.
Method
Study site
A study was conducted across all 12 PHC clinics in Region Three in the City of Tshwane Metropolitan Municipality. The clinics were selected for their proximity to the central business district, suburbs and townships in the western area of Pretoria. They generate substantial family planning information, because the youth and adult populations largely reside in the area for employment prospects (Gauteng Department of Health, 2017).
Study design
An exploratory research design was used to collect data from managers. The design allowed the researchers to explore and understand the use of family planning information for decision making by PHC clinic managers.
Participants and sampling
The study population was made up of clinic managers (12), each representing a clinic. A total population sampling approach was used to select all 12 clinic managers responsible for data management and decision making within their respective clinics. However, only 11 were interviewed due to data saturation, the point at which no new information was provided. Contact information for the clinic managers in Region Three of the Tshwane Metropolitan Municipality was obtained from the Human Resource Office, Department of Health, Tshwane District. Managers were contacted by telephone and then sent study-related emails. Those who were included had all consented to take part in the study.
Data collection
The first author (SMM) scheduled appointments for data collection with participating managers, who were provided with consent forms that explained the circumstance of study participation. The researcher explained the nature of the research, procedures, potential risks and benefits, the reason for the study and how the collected information would be used. In-depth face-to-face, semi-structured interviews were conducted from March to June 2019 in the respective clinics where the managers worked. Semi-structured interviews were appropriate for this study because they enabled the researchers to be sure that the specific set of questions about the use of family planning information was answered (Polit and Beck, 2021). The overarching questions were: (i) how is family planning information used for decision making? and (ii) what is your role in using family planning information to make evidence-based decisions? Interviews lasted between 45 and 60 minutes. The researchers took field notes during the interviews, and with the managers’ permission, all interviews were audio recorded. Data collection continued until saturation was achieved, which was determined by concurrent data analysis. The data were stored in adherence to local rules and policies regarding the confidentiality and data security.
Data analysis
Thematic analysis was carried out manually through coding and categorisation. The researchers first transcribed each audio recording verbatim, then listened to the audio recordings and reviewed the transcriptions multiple times to gain a deeper understanding of the data. The data in the transcripts were divided into different meaningful units using coding. The codes were developed based on the differences, similarities and meanings that emerged from the categories. The researchers labelled the categories according to the information obtained and combined them to create relevant subthemes. The subthemes were merged into themes (Nieuwenhuis, 2017; Polgar and Thomas, 2020).
Ethics approval
Ethical clearance was obtained from the University of South Africa (UNISA) Research Ethics Committee, the Department of Health Studies (HSHDC/719/2017), and the Tshwane District Research Committee granted permission to conduct the study. During data collection, confidentiality was maintained by avoiding the use of actual clinic and manager identifiers. Managers were given a unique numerical code according to the sequence of interviews. Transcripts were de-identified by removing names during the transcription of the interviews.
Results
Demographic characteristics
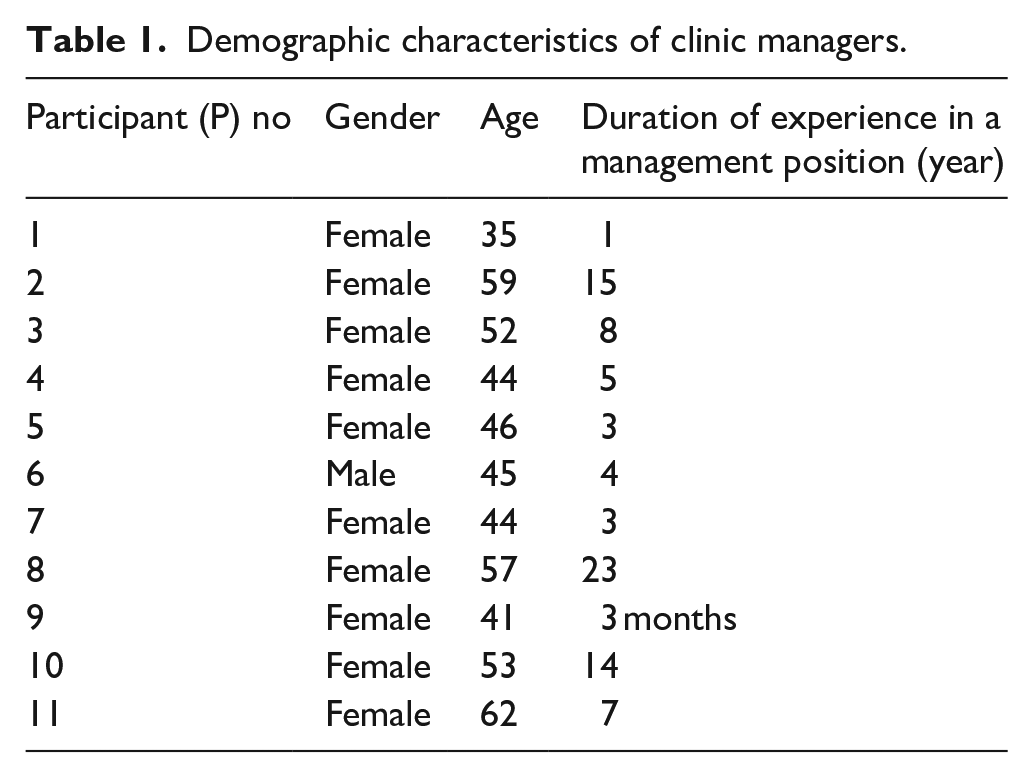
Eleven clinic managers were interviewed for this study. All clinic managers were registered nurses. Most participants were females (10 of 11) with a mean age of 48.9 years. Their experience in clinic management ranged from 3 months to 23 years (See Table 1).
Demographic characteristics of clinic managers.
Themes
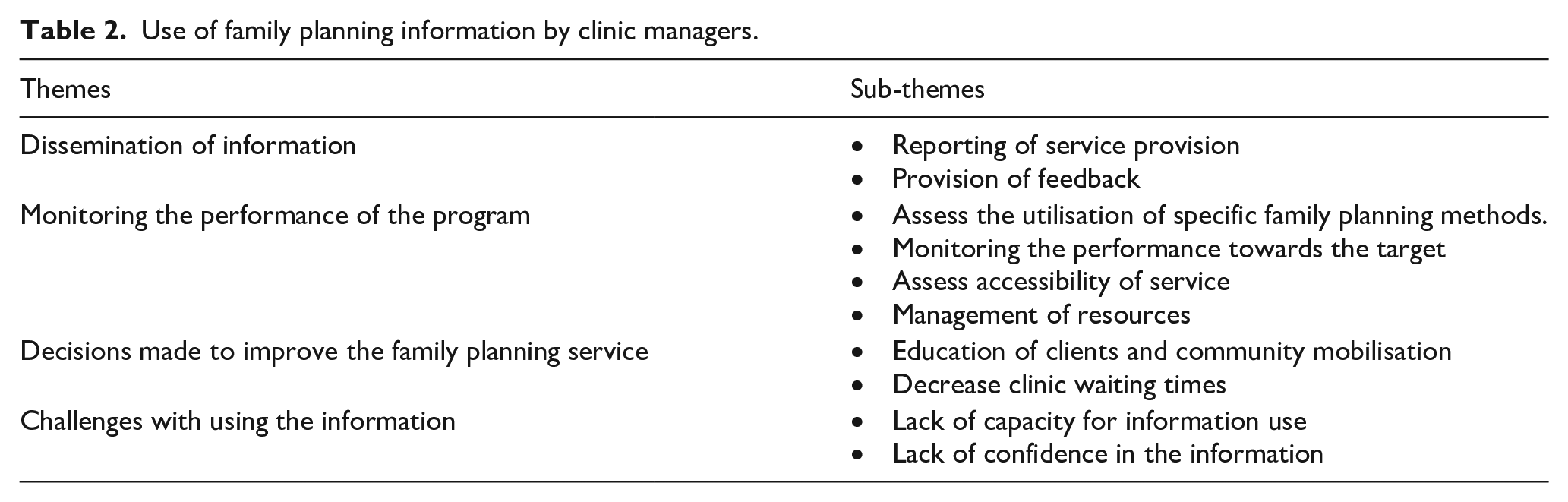
Themes and subthemes concerning the use of family planning information by clinic managers are outlined in Table 2.
Use of family planning information by clinic managers.
Information dissemination
Reporting of service provision
Most clinic managers explained that once the data have been collected by the healthcare providers while providing the family planning service, they are entered into the computer, validated and used to generate a monthly report. The report is compiled in a standard Microsoft Excel spreadsheet and sent to the next managerial level, the district health information office.
After the data has been entered into the computer and validated, the system generates a summary spreadsheet report. This is the form we use to report monthly services to the district office, including family planning. (P2)
Provision of feedback
Clinic managers stated that they use the family planning information to provide performance feedback to the healthcare providers. Performance is based on the number of family planning methods provided for the specific month. Feedback is provided at weekly meetings held in the clinics. In addition, managers attend quarterly review meetings with health information managers, where they review the quality of data and performance of the family planning program. Upon their return from the review meeting, they share the feedback from the review with staff.
I count the number of family planning methods we have distributed at the end of every month. Afterwards, I will update the staff during our weekly meetings. (P6) Following the quarterly review meeting, we hold our weekly meeting to provide feedback. We discuss the feedback to ensure that it is understood, as well as the implications of data quality in terms of service performance. (P11)
Monitoring the performance of the program
Assess utilisation of specific family planning methods
Managers mentioned that they use family planning information to assess the utilisation of family planning methods among women of childbearing age in their catchment areas. Short-acting hormonal methods, such as oral pills and injectables, were used more often when compared to long-term methods, such as the intrauterine device (IUD) and subdermal implant. Long-term methods were the least preferred due to their side effects: We are gathering information on family planning methods and comparing it with the population of women of childbearing age in a catchment area. Then we can determine the most preferred methods. (P1) Many clients are currently using short-acting methods such as injections and pills, and we are currently attempting to encourage them to switch to long-acting reversible contraception (LARC) methods such as IUDs. (P6) Clients say that the loop (intrauterine device) and the implant causes heavy menstruation. (P10)
Monitoring the performance towards the target
Every year, the managers set a family planning service performance target using the previous year’s performance as a benchmark. Each clinic establishes quarterly and annual targets, which are reflected in the operational plan. Managers will then use the generated information to compare the actual performance with the target.
Data are used to determine whether or not the family planning target is met. Quarterly, we review the program’s performance indicators in relation to the established target. Then, we can determine whether we have performed well or poorly. (P2) The operational plan will indicate the coverage for last year. The coverage is used as a baseline for this year and set quarterly and annual targets. I will compare the quarterly performance against the set targets. (P5)
Assess accessibility of service
Some managers reported using the family planning information to assess the accessibility of family planning services and to identify potential gaps in the program. This can be accomplished by comparing the rates of unintended pregnancy and abortions to the target population covered by the methods. High rates of unplanned pregnancy and low coverage of the target population would indicate that the service was not accessible to the community.
When clinic staff members report complications following illegal abortions, we realise that some women who do not want kids, get pregnant. We first ask whether our services are sufficiently accessible. Are we adequately protecting them against unintended pregnancies? (P1) The high rate of teenage pregnancy shows that there is a challenge with the accessibility of the service, and women are not using the methods. (P3)
Management of resources
Managers stated that generated information was used to allocate the clinics’ resources. The service utilisation rate influences the decisions, and the greater utilisation of the service indicates increased interest. Resources would be redirected to the family planning service in response to this information.
I utilise the data to assign human resources to specific programs. I can see from the data, for instance, that this clinic has many people using family planning services and fewer clients using other services. I will assign more nurses to the family planning service. (P9)
Some managers revealed that they use the information to budget for family planning methods based on usage, thereby preventing the incidences of expired and shortage of stock.
We allocate the budget to family planning methods. My responsibility is to ensure that budget is done according to the utilisation, preventing the occurrences of shortage of methods or overstock, which can result in the expiry of methods. (P8)
Decisions made to enhance family planning service
Education of clients and community mobilisation
Managers recognised that women prefer short-acting hormonal methods as compared to long-term reversible methods due to unfamiliarity, side effects, and lack of awareness regarding the benefit of long-term reversible methods. To improve the utilisation of the long-term methods, clients were educated about these methods, and community outreach program’s used to increase awareness of these methods in the schools and communities.
If, for a week, we do not have any clients for an implant, I will start urging nurses to hold educational sessions at the front desk so that clients can decide to insert the implant. (P4) We request that health promoters, who visit the community and schools to educate the community about long-acting reversible methods. (P10)
Decrease clinic waiting times
Managers acknowledged that time spent in the clinics affected the utilisation of the service, especially among school-going teenagers. They commented that decreasing the length of time clients spent in the clinics for family planning purposes could encourage and inspire clients to make better use of the service. Thus, all clients requiring family planning services were attended to promptly, and clients who visited the clinics for other services and also needed family planning services were seen at a single service point: We ensure that even school-aged children do not have to wait in a long line. We attend them first so they can attend school and continue using our services. Those seeking treatment for a chronic illness are also given their methods in the same room, even though family planning is typically handled in the maternal and child unit. We prevent long waiting times. (P5)
Challenges with using the information
Lack of capacity for information use
Although family information was available, managers could not use it effectively to improve the services due to a shortage of human resources. They understood that the clinics were not meeting the target but there were insufficient staff to provide the full service. Furthermore, some staff did not have the skills to perform some family planning interventions, mainly the insertion of the implant and the IUD.
Yes, you can see that the clinic needs to do better on family planning, but we cannot correct the situation because our nurses are not competent in providing other methods like implants and IUDs. (P1) We do not have enough staff to serve the increasing population. Most of the staff are overwhelmed by the workload. Some take vacation and sick leaves, leaving the remaining ones under pressure and unable to offer the services as planned. (P7)
Lack of confidence in the information
The managers mentioned that they sometimes question the accuracy of the data generated, that the information generated might not be a true reflection of their clinic’s performance. According to the managers, there is a lot of migration in and out of the city, with many private providers in the city offering the service. Therefore, people could choose to access family planning services elsewhere and their data then not included in the clinic performance data. The managers also acknowledged the role of staff attitudes towards data accuracy. Some staff did not record data correctly, which impacted negatively on data accuracy, leading to a lack of confidence and inefficient use of the information.
People in the city often move around and use clinics close to them, including private doctors and hospitals. I do not think the private providers report their services to the district office. I think this is one of the reasons we are seen not performing well. I sometimes become discouraged in using the information because it does not accurately reflect our clinic’s performance in terms of population coverage. (P1) Staff attitude. Even though I provide performance feedback to staff regarding data quality and coverage, some staff do not use the feedback to improve due to negative attitudes. They continue committing the same data collection errors. We end up questioning the accuracy of the information. (P5)
Discussion
This study explored the clinic managers’ perspectives on using family planning information in the Tshwane district. The family planning information was used to report monthly performance to the district and to provide feedback to the healthcare providers. Similarly, several studies in Ethiopia and Palestine revealed that most health institutions used routine health data to report the services to the next management level (Abera et al., 2016; Asemahagn, 2017; Mimi, 2015; Wude et al., 2020). The reporting of information is critical in ensuring the information is available to stakeholders involved in managing data and using information. The managers in this study complied with the Department of Health (DoH) guidelines, which necessitate the reporting of monthly data to the district (Department of Health South Africa, 2012).
Information sharing through feedback on data quality and family planning performance was constant in this study, when compared to findings in Kenya and Ethiopia, where some healthcare providers did not receive such feedback (Cheburet and Odhiambo-Otieno, 2016; Dagnew et al., 2018; Wude et al., 2020). The feedback meetings were frequent compared to the situation in Kenya, where some health institutions did not have any meetings at all, and others had annual or quarterly meetings, and only a few had monthly gatherings (Cheburet and Odhiambo-Otieno, 2016). Department of Health PEPFAR USAID & MEASURE Evaluation SIFSA (2016) stated that information generated should be shared within the clinic to allow healthcare providers and the manager to decide how best to render services based on information that is readily available locally. Timely feedback encourages information utilisation because it enables healthcare providers to discuss and understand how the program’s performance is reflected in the data (Afe et al., 2018; Shiferaw et al., 2017). This is essential for quality improvement practices because it can generate constructive suggestions that will motivate healthcare providers to perform well (Kumwenda et al., 2017; Shiferaw et al., 2017), whereas a lack of feedback from managers can be seen as a hindrance to information utilisation at the clinic level (Afe et al., 2018).
Similar to findings in Ethiopia, managers in the current study used the information to measure trends regarding the use of specific methods and to determine the acceptance of various methods (Afe et al., 2017). They discovered that short-acting hormonal methods were preferred over long-acting methods due to clients’ unfamiliarity with long-acting reversible contraception. These findings are similar to earlier studies conducted in Ethiopia, where many women used methods that only lasted for 3 months or less, such as injectables and oral methods.(Amentie, 2015; Endriyas et al., 2017). In contrast, the study conducted in Erzurum discovered that the most commonly used method was the long-acting method, the IUD, followed by the oral pills (Çalikoğlu et al., 2018).
The family planning information was further used to measure the performance of the clinics towards the set target as reflected in the operational plans. The CYPR is an indicator used to measure the performance of the family planning program (Moloko, 2021). It reflects the percentage of women between the ages of 15 and 49 who use contraceptive methods to prevent pregnancy (Massyn et al., 2019). Good performance will be demonstrated by meeting the quarterly and annual targets as reflected in the operational plan. The study findings are consistent with the recommendations by PEPFAR, USAID, and MEASURE Evaluation (2014), indicating that operational plans should reflect the targets and activities required to meet the targets. However, the current findings contradict a comparable study undertaken in Rwanda, which revealed that operational plans of health centres were not based on available information. No health institutions had a quarterly plan, and the baselines were not based on evidence from the HIS (Innocent et al., 2016).
As a basis for measuring the accessibility of services, managers used the information to compare the occurrences of unintended pregnancy and the use of family planning methods (Moloko, 2021). They argued that the high rates of unintended pregnancies indicate a lack of accessibility to service, which results in low utilisation of the methods. Similarly, a South African study found that many South African women do not use contraceptives, leading to unintended pregnancies and abortions (Chola et al., 2015). Some abortions were performed in unlicensed institutions, putting women’s health at risk. It is, therefore, essential to recognise that induced abortions caused by unintended pregnancies can be prevented by using family planning methods (Vlassoff et al., 2016). For this reason, using the information to monitor the accessibility and utilisation of family planning methods and improve the service is critical in reducing maternal mortality; consequently, improving maternal and child health (Chola et al., 2015).
The study shows the importance of information in resource management. The managers used the information to reassign and redistribute staff members to various services based on evidence of utilisation from the generated information. Increased demand and utilisation of the service, mainly family planning, necessitated the addition of more healthcare providers providing the service. Consistent with these findings, a similar study in South Africa found that health information was utilised to distribute resources based on the need for the services (Nicol et al., 2017). Correspondingly, studies in Ethiopia and Rwanda found that health information was utilised to distribute resources, such as hiring more staff to enhance services (Dagnew et al., 2018; Innocent et al., 2016; Moloko, 2021).
In addition, managers used family planning data to develop budget for family planning methods. The information seemed useful for controlling the supply chain of the clinics and preventing overstocking and the expiry of stock. Findings from previous studies concur that information should be utilised to evaluate the usage of medical supplies for a specific program, to estimate stock requirements to prevent stock-outs, and to purchase medication (Dagnew et al., 2018; Innocent et al., 2016; Kumwenda et al., 2017; Ohiri et al., 2016; Seitio-Kgokgwe et al., 2016). Managers require data to calculate indicators that provide a picture of the required resources for their service areas (USAID and MEASURE Evaluation, 2015).
Managers were able to make decisions to improve family planning services based on the generated information. After they identified the need to enhance the utilisation of the long-acting methods to improve the performance of the service, the managers decided to plan awareness activities about the availability and advantages of long-acting family planning methods. The activities included educating clients in the clinics and doing outreach sessions. The decision to use the information was appropriate to the context of trained community health workers who could provide factual information and dispel negative rumours about the methods. Thus, community mobilisation increased the demand and utilisation of contraceptive methods in low-demand and low-utilisation communities (Ho and Wheeler, 2018). Undoubtedly, information is essential for planning community mobilisation strategies and exchanging data with other health institutions (Dagnew et al., 2018; Moloko, 2021).
The other decision was to improve the utilisation of the service by reducing the time the client spends in the clinics. The managers designated the family service as a “fast queue,” meaning that all clients who visited the clinics solely for family planning were offered quick service in a single consultation room. The practice indicates that clinics make action-oriented decisions based on available information. This is consistent with Shiferaw et al.’s. (2017) perspective that information must first be utilised where it was generated. The National DoH recommends that when clients come to the clinic for acute or chronic care, they should be attended to and given a family planning method in the same consultation room (Moloko, 2021). On subsequent visits, clients will be expedited to the family planning service at the maternal and child division. At the same time, adolescents and young adults will be seen after school (National Department of Health, 2015).
Although the managers used the information to manage the family planning service, they also encountered some challenges. One of the main challenges faced was a shortage of staff to provide family planning services to a large population. This led to an increasing workload and pressure among the existing staff. Additionally, the available staff lacked the necessary skills to offer long-acting methods such as IUDs. For this reason, managers could not satisfactorily improve the family planning service’s performance. In contrast to the current study, healthcare institutions in Bangladesh, the Democratic Republic of Congo, and Malawi were able to increase the performance of the family planning program because there were sufficient staff competent in inserting the IUD (Haider et al., 2019; Ho and Wheeler, 2018; Lemani et al., 2018).
The second challenge was the lack of confidence in the information generated because of the uncertainty regarding the accuracy of the data reported to the district office. The coverage data were considered not to accurately represent the clinics’ performance because some women use private practitioners whose data are believed not to be reported at the district level. Consequently, the clinics are not performing because women in their catchment population are seen elsewhere. Indeed, it was discovered that about one-third of women use private practitioners for family planning, even those residing close to public health institutions (Fruhauf et al., 2018). This is mainly due to shorter waiting times (Young, 2016). It is evident that the family planning data from private practitioners are not reported to the district. Massyn et al. (2019) confirmed that the CYPR reported for South Africa only reflects the services offered by public clinics.
Incorrect data recordings due to staff attitudes affected data accuracy, a challenge not unique to this study. Similar studies in Malawi, Pakistan and South Africa found that data errors affect the accuracy of the information, and consequently, the program’s performance, which led to a lack of confidence in the generated information. As a result, the information was not used optimally (Kumwenda et al., 2017; Nicol et al., 2017). Negative attitudes could also suggest a lack of understanding of the importance of information in improving client care and managing the healthcare program and the service in general (Kasambara et al., 2017; Kumwenda et al., 2017; Moloko, 2021; Muhindo and Joloba, 2016). Underutilisation of family planning information can significantly hinder the improvement of the program, consequently affecting the country’s performance towards the reduction of the maternal mortality ratio (Starbird et al., 2016; United Nations, 2018)
Limitations
As this was a qualitative study with a small sample from one district in Gauteng Province, the results are not generalisable to other populations or clinics; however, the findings of the study might prove useful for other districts in the province with similar contexts. The qualitative approach provides rich information on the use of family planning information and the challenges encountered at the clinic level.
Conclusion
The study showed that the clinic managers used the family planning for improving the service. The managers disseminated family planning information to the staff and the district, enabling them to make informed decisions and devise measures to enhance the performance of the family planning program. Regrettably, despite their best efforts, they faced challenges with staff and lack of collaboration between the public and private healthcare sectors. The findings thus suggest that an increase in the number of healthcare providers and a capacity-building of the available staff to offer comprehensive family planning services, are required. It also proposes the collaboration between private providers and public health institutions in data management and reporting. To improve the accuracy and reliability of the information in measuring the performance of the family planning program, both stakeholders should ensure that all services are reported at a commonplace. Therefore, the National DoH should design a system incorporating data from the private and public sectors. This might improve the use of information in monitoring and evaluating the performance of the health sector.
Footnotes
Acknowledgements
The authors wish to acknowledge Sefako Makgatho Health Sciences University for the research grant which enabled them to carry out the research study, the University of South Africa for approval, the Tshwane Research Committee for permission, as well as the selected PHC clinic managers for participating in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Sefako Makgatho Health Sciences University Research Development Grant.
ORCID iDs
Research data availability
The data that support the findings of this study are available from the corresponding author, upon request.