
Abstract
Introduction
Clinical registries collect data about diseases, procedures, devices, drugs or healthcare resources, and are observational in nature (Australian Commission on Safety and Quality in Health Care, 2024b). Impactful clinical registries should employ the principles of effective governance, appropriate data collection, robust data management, implementation of quality assurance activities and outcomes reporting (Parker et al., 2023). For effective operation, key personnel at a clinical registry include a director with clinical expertise, a registry manager to oversee day-to-day operations, statistical support, data coordinators, collectors and processors and administrative support (Australian Commission on Safety and Quality in Health Care, 2014a).
There is increased demand for health information managers (HIMs) to work at clinical registries (Gjorgioski et al., 2023). This demand is attributed to the alignment of HIM professional competencies with the core operations of a clinical registry (Gjorgioski et al., 2023). In Australia, HIMs are university-degree qualified specialists in health information and data management (Wissmann et al., 2024). The core competencies of HIMs encompass the domains of health records management, healthcare classifications and terminologies (including clinical coding), research, health data analytics, health service organisation and delivery, health information law and ethics, and health informatics (Health Information Management Association of Australia, 2023).
HIMs are well-placed to work at clinical registries, with approximately one in five (17.8%) final-year health information management students (2012–2021) undertaking industry placements at a medical research/health or disease screening/registry during their degree (Robinson et al., 2025).
In this study, we explore and describe: (i) the roles, responsibilities and perceptions of HIMs working at Australian clinical registries and (ii) the reported HIM workforce within clinical registries.
Method
Study design and sample – Aim 1
A cross-sectional study design was utilised and reported based on the Survey Reporting Guideline (SURGE; Grimshaw et al., 2014). Eligible participants were qualified HIMs aged ⩾18 years, with current or recent (within 5 years) employment at an Australian clinical registry since obtaining their health information management qualification. The authors were not excluded from participating if they met the inclusion criteria. Participants were engaged through snowballing methods using personal email advertisement and flyers. Researchers circulated these advertisements via extensive professional networks, health information management degree course coordinators (La Trobe University, Queensland University of Technology, University of Tasmania), the Australian Clinical Trials Alliance Clinical Quality Registries Special Interest Group, members of the Australia and New Zealand Stroke Coding Working Group, conferences during the recruitment period (Australian Clinical Trials Alliance Clinical Trials and Registries Symposium) and industry newsletters (Health Information Management Association of Australia).
HIM survey instrument
The survey was developed by HIMs with research and registry experience and was based on prior HIM workforce profiling work conducted by Riley et al. (2020). The survey (Supplementary Box 1) comprised four parts: demographics, background, registry employment and roles and responsibilities. A mixture of open- and closed-ended questions were used to collect participant demographics (age, gender), and professional background (health information management qualification including the degree awarded, institution and year, and other qualifications obtained or in progress). Information about clinical registry employment was obtained through open-ended questions about the current/last position title, length of employment and a closed question to rate self-perceived level of competence (novice, advanced beginner, competent, proficient, expert; Dreyfus, 2004). Participants who indicated they have considered leaving their current role, or participants who no longer work at a clinical registry, were prompted to indicate reasons why. An open-ended question gave all participants the opportunity to provide in-depth responses about what factors would improve their job satisfaction at a clinical registry.
A mixed-methods approach was used to obtain information on roles and responsibilities of HIMs at clinical registries. Five-point Likert scales (e.g. never, rarely, sometimes, often, always) were used to estimate the typical proportion of time HIMs undertook tasks based on the domains of the HIM Professional Competency Standards (Health Information Management Association of Australia, 2023). These domains include health classification, health informatics, health data analysis and health information management. The proportions of time were defined as never 0% or not at all, rarely 1%–20% of the time, sometimes 21%–50% of the time, often 51%–80% of the time and always 81%–100% of the time or consistently. Open-ended questions were used to ascertain a description of a participants’ typical day in their role, and their perceptions about the type of roles HIMs can contribute to at a clinical registry.
Data collection
The survey was self-administered and completed online via the Research Electronic Data Capture tool hosted at Monash University (Harris et al., 2009, 2019). Data were collected from 20 November 2024 to 31 January 2025. Participation was voluntary and consent was implied by survey completion. Survey responses were anonymous, but participants were asked to disclose the name of the clinical registries they had worked at. Participants were offered the choice to enter a prize-draw to win one of five AU$50 supermarket gift vouchers. Personal details collected for the prize-draw were kept separate from survey responses.
Clinical registry data custodian survey – Aim 2
A second survey was developed for data custodians (or similar roles) within Australian clinical registries (Supplementary Box 2). This survey comprised six questions to ascertain whether the registry employed HIMs (including the number and total employment fraction), roles, responsibilities and skills of HIMs at the clinical registry, and an open-ended question about skill gaps in their workforce. This survey was emailed to the registry contact for 124 clinical registries listed on the Australian Register of Clinical Registries (Australian Commission on Safety and Quality in Health Care, 2024c), with one reminder email. Data were collected from 16 to 31 January 2025.
Data analysis
Descriptive statistics were used to summarise quantitative data from both surveys. Position titles were classified into six broad areas by mutual agreement between the researchers: clerk/administration, HIM, clinical coder, data manager, director/executive and other manager. The level of seniority was determined based on position title in conjunction with classifications used in applicable enterprise agreements and awards (Fair Work Commission, 2020, 2022). Clerk/administration roles were considered entry-level, director/executive and “senior HIM” roles were considered senior-level and all other roles were mid-level.
All free-text data were summarised using inductive thematic analysis (AS). Triangulation, by including the collection of quantitative and qualitative data, was used to evaluate the survey responses, in order to improve the understanding of results and gain insights into common themes (Carter et al., 2014). A pragmatic sample of ~25% of responses were dual coded by an independent reviewer (CB) to check interpretation against the data. Furthermore, ongoing discussions between the research team were used to ensure data were being interpreted and summarised to best reflect the intended meaning.
HIM survey responses with incomplete answers to demographic, background and registry employment were excluded from the final analysis. Data were analysed using Microsoft Excel and STATA/SE 18.0 (StataCorp., College Station, TX, USA). All data were de-identified to ensure that no individual nor clinical registry could be identified.
Ethics
Ethics approval for this study was obtained from Monash University Human Research Ethics Committee in Victoria, Australia (Project ID: 45658).
Results
Characteristics of HIM survey participants
Of 30 responses received, 16 were included in the analysis. Responses were excluded where they were incomplete (n = 7), the individual did not have a health information management qualification (n = 4) or did not have post-qualification employment at a clinical registry (n = 3; Supplementary Figure 1).
Majority of respondents were female (94%) and half were aged <40 years (50%). Nine respondents held Bachelor degrees (56%) in health information management, six Master degrees (38%) and one Associate Diploma (6%). Most respondents (69%) graduated from La Trobe University/Lincoln Institute of Health Sciences, Victoria. Almost half (44%) received their health information management qualification <5 years ago, with a median of 8 years since graduation (interquartile range [IQR] 4–28, range 1–40).
Seven respondents (44%) held qualifications prior to studying health information management, of which six were allied health or health-related degrees. Since qualifying as a HIM, three respondents (19%) have undertaken or are currently completing further study in the areas of public health, business administration, health promotion and information technology. Seven respondents (44%) indicated they had no intention of completing further study, while the remainder were unsure (56%, n = 9).
Employment of HIMs in clinical registries
The employment history of the 16 respondents spanned 17 national and state-based clinical registries. The most common job titles were HIM (25%, n = 4), data manager (25%, n = 4) and clerk or administration officer (19%, n = 3). Five (31%) position titles were “HIM” or “clinical coder.” One in four respondents (25%, n = 4) were in senior-level roles (e.g. senior HIM, executive/director), 56% in mid-level roles (e.g. HIM, other manager; n = 9) and 19% in entry-level roles (e.g. clerk, administration officer; n = 3).
Ten respondents (63%) were currently employed at a clinical registry and all reported being happy in their current role. Of these respondents, there was a median of 5 years (IQR 3–9) total experience at clinical registries and 3 years in their current role (IQR 1–4). Four (40%) respondents sometimes, often or always considered leaving their position due to lack of support (25%), too large a workload (50%) or to take a better position (50%). The main factor that would improve job satisfaction was better workplace conditions related to resources and funding. Specifically, respondents commented on a desire for greater access to training/education opportunities, employment of more HIMs at clinical registries, more secure employment contracts and increased funding to support clinical registry activities (e.g. “developing dashboards/data reports for the registry”). One respondent stated that they would be more satisfied if they were “able to use more of my health information management skills” in their role.
Of the six respondents who did not currently work at a clinical registry, all had worked at a clinical registry within the last 2 years. The reasons provided for leaving their clinical registry role were similar to those who consider leaving their current role, with the addition of employment contract expiry and the impacts of the COVID-19 pandemic on the workplace. Three respondents (50%) reported their role at the clinical registry was enjoyable; however, four indicated changes to general workplace conditions (e.g. management, communication, support for staff, employment type, funding) would be likely to improve their job satisfaction (e.g. “additional funding and resources to better support the use of the data would have been useful”).
Perceptions of utilisation of health information management skills and experience in clinical registries
Most respondents reported their level of competence in their role at a clinical registry as proficient (53%, n = 8) or expert (27%, n = 4). None identified as a novice.
Fifteen respondents outlined a typical work day at a clinical registry. Responses were diverse with a wide range of tasks listed by each respondent (median of seven tasks per respondent, IQR 5–8). Activities undertaken during a typical work day included data-related activities, including database management, data analysis, data cleaning, development of reports and research-related tasks. Other respondents described administrative activities including handling enquiries from participants and clinicians, coordinating mail outs for participant follow up, event coordination (conferences, workshops, meetings) and minute taking. Several respondents described management activities such as coordination of the registry, ethics and governance, staff management, overseeing budgets, managing contract and service agreements, policy development, leading key strategic projects and stakeholder engagement (e.g. government, industry). Other respondents were involved in activities related to health informatics, such as testing and implementing new databases and systems, developing dashboards, and being a “‘go-between’ for IT and end data users.” Two respondents reported that clinical coding was part of their role.
When asked what types of roles HIMs could fulfil at a clinical registry there were a variety of responses. Comments were categorised into 13 main themes. Majority of comments were related to roles in data and database management (n = 13), and data analysis and reporting (n = 13; Figure 1). Other common roles suggested were project management (n = 5) and research activities (n = 5). One respondent stated that “HIMs are well placed” to contribute to research activities as they bring a “unique knowledge of data/legislation/privacy aspects [that] are useful for managing ethics and data linkage applications and the HIM degree provides training in management of people and importance of record keeping.”
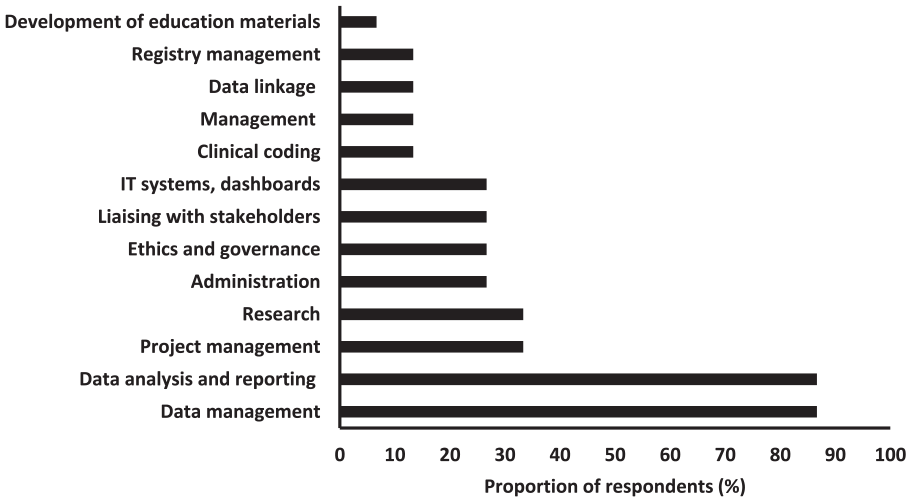
Roles and activities that health information managers can contribute to at a clinical registry (n = 15).
Of the 15 respondents to the final part of the survey (employment and roles and responsibilities), the proportion of time undertaking tasks across the four domains of health information management was varied. The most common activities undertaken by HIMs at a clinical registry related to health informatics, health data analysis and health information management, with ⩾50% of respondents performing tasks from these domains at least “sometimes.”
The responsibilities of database management (73%) and development of system documentation (53%) were frequently reported (often/always) tasks related to health informatics (Figure 2). The majority of tasks undertaken from the health data analysis domain were data integrity and governance (67%), routine or ad hoc data publications or requests (60%) and other data interrogation or visualisation (60%). Common tasks related to health information management were project management (60%) and clinical governance or quality management (53%).
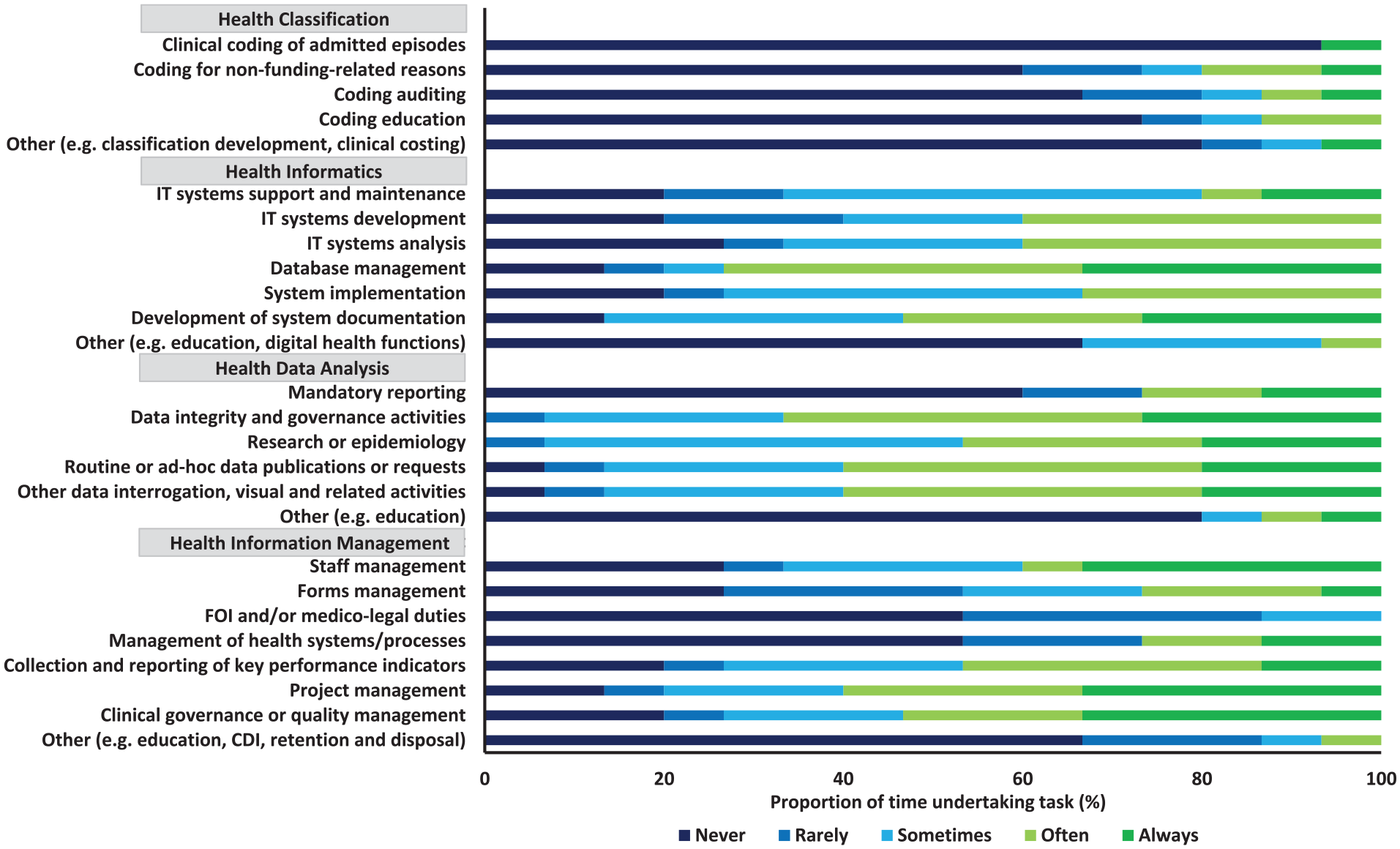
Proportion of time undertaking health information management task in a typical day at a clinical registry (n = 15).
Responsibilities related to health classification were least reported by HIMs at clinical registries, with seven respondents (47%) never undertaking tasks from this domain. The majority never performed clinical coding of admitted episodes (93%), coding for non-funding related reasons (60%), nor conducted coding auditing (67%) or coding education (73%).
Data custodian survey
There were 38 responses received from data custodians (or similar roles) at Australian clinical registries (31% response rate; n = 3 unable to be contacted). Of the 38 responses, eight were incomplete and excluded from the analysis. Three clinical registries provided duplicate responses (identified by registry name), and in these instances, the response with the most complete data was retained. In total, 27 responses were included in the analysis.
Overall, 12 (44%) of the clinical registries reported current or recent (within 5 years) employment of HIMs. A total of 23 HIMs were reported to be employed at these clinical registries (10 full-time, 11 part-time, 2 casual) with a median total employment fraction of 1.1 full-time equivalent (IQR 1.0–1.7). The primary roles and responsibilities of HIMs reported by clinical registry leadership were data collection and management (n = 11 registries, 92%) and quality assurance and compliance activities (n = 10, 83%). Eight (67%) of these clinical registries reported HIMs were responsible for data analysis and reporting, patient privacy and confidentiality, and other activities (e.g. data linkage, ethics and governance, finance, staff supervision, administration, project management, registry management).
Respondents commented that the critical skills HIMs contribute at clinical registries include data management (including collection and compliance; n = 10), project management (n = 7) and data analysis (n = 6). Respondents stated that HIMs have an understanding of ethics and governance (including relevant legislation; n = 5), and knowledge of clinical coding (n = 3). Other skills listed include understanding of the organisation and functions of the hospital system and medical records (n = 2), staff management (n = 2), stakeholder engagement (n = 2) and report writing (n = 1). Three respondents listed skills possessed by HIMs at their clinical registry which were outside the scope of a HIM (e.g. specimen collection, clinical work).
Sixteen of the clinical registries (59%) identified gaps in the skillset of their overall registry workforce (Figure 3). This included missing or limited expertise in statistical analysis/biostatistician (n = 7), database management and analysis (n = 4), dashboard development (n = 2), implementation science (n = 2) and epidemiology (n = 2). Other areas of expertise that were lacking in the overall registry workforce included clinical quality improvement, health economics, information technology, policy and legal, marketing and communications (all n = 1). Additional descriptive analysis showed that only the clinical registries that did not report employment of qualified HIMs experienced gaps in database management and analysis skills (n = 4).
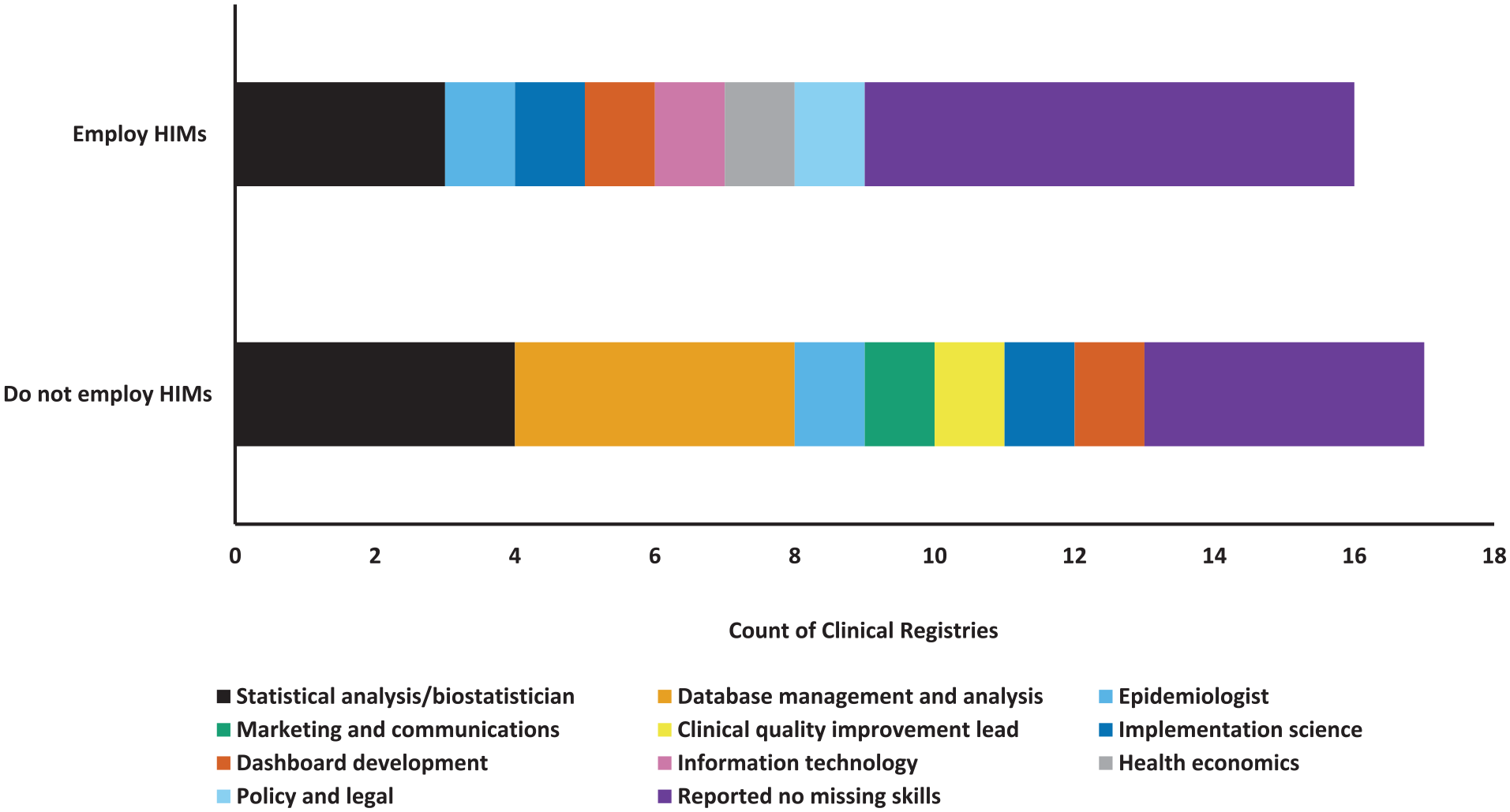
Missing skills identified at clinical registries (n = 27). Multiple answers were allowed from each clinical registry.
Discussion
We provide new evidence into the skills, roles and responsibilities of HIMs working at Australian clinical registries. The role of HIMs at clinical registries is varied and HIMs utilise many skills from the core domains of the profession explored in this study. However, some skills are underutilised at clinical registries, particularly those related to health classification and HIMs report a desire to use more of their skills within their role. Clinical registries that do not employ HIMs reported workforce skill gaps in areas which fall within the remit of HIMs.
Our study demonstrated that there is no standard “typical workday” for a HIM at a clinical registry. Roles and responsibilities are varied, and HIMs consistently utilise a range of their skills at clinical registries. Skills from the domains of health informatics, health data analysis and health information management were employed “sometimes or more” by the majority of respondents. This aligns with prior research where most HIM graduates were found to work in positions where they utilised three or four of these knowledge-skill domains (Gjorgioski et al., 2023; Riley et al., 2020). Despite being one of the core capabilities of HIMs, few respondents utilised skills in health classification (including clinical coding). As technology improves clinical coding is more likely to be automated, and codes are increasingly extracted from patient administration systems, which reduce the need for HIMs to code at clinical registries (Campbell and Giadresco, 2020; Nguyen et al., 2015). Other tasks that were infrequently undertaken by HIMs at clinical registries in our study include mandatory reporting and freedom of information requests. These tasks are typically conducted within hospital settings, and HIMs who choose to work in a clinical registry may do so because they do not want to focus on “traditional” components of health information management.
Historically, HIMs have predominantly worked in health information services within hospitals (Gjorgioski et al., 2023; Riley et al., 2020; Watson, 2008) with position titles such as HIM or clinical coder. Despite conducting this study in a non-traditional health information management environment, approximately one in three position titles at clinical registries were “HIM” or “clinical coder.” HIMs are part of the Australian health workforce (Australian Institute of Health and Welfare, 2024) and use of these traditional role titles may indicate that the knowledge and skills of HIMs are being recognised outside of hospital settings (Riley et al., 2020).
The 2021 Census of Population and Housing reported that 2000 HIMs work in Australia (Jobs and Skills Australia, 2024), but these estimates may be conservative given the diversity of HIM job titles. Based on the census data, our sample of 16 HIMs working at clinical registries represents ~1% of the Australian HIM workforce. While the total number of HIMs working in clinical registries is unknown due to limited data capture (i.e. those potentially missed in our study), our sample is lower than previous estimates. For example, the authors of an Australian survey of 130 health information management graduates (2017–2021) reported that 9.2% (n = 12) of HIMs work in research/cancer/screening or registry settings immediately after qualification (Gjorgioski et al., 2023). Based on these data, and given we only sampled one of these settings, we believe we received responses from most HIMs employed in clinical registries at the time of conducting this study (n = 16).
Our results have identified skill gaps at clinical registries which HIMs can competently fulfil. Four clinical registries reported lacking capability in database management and analysis, and all four of these registries did not employ HIMs at the time of this survey. These database skills are a component of health informatics which is a core capability of HIMs (Health Information Management Association of Australia, 2023). Two clinical registries reported a lack of skills in dashboard development. While complex computer programming may be considered an advanced level of competency, HIMs are skilled in data visualisation and informatics (Health Information Management Association of Australia, 2023). At most clinical registries where HIMs were employed, we observed a good alignment between the perceptions of senior leadership about the skills that HIMs contribute, with the professional competencies of HIMs. Clinical registries that employed HIMs reported fewer missing skills than those that did not employ HIMs, which may indicate that there is a broad contribution of HIMs at clinical registries.
HIMs have demonstrated that they can apply their skillset and diverse expertise along the broad spectrum of activities routinely undertaken at a clinical registry. Our results align with previous evidence related to the involvement of HIMs at clinical registries in establishing registry processes, data entry and analysis, reporting outcomes, quality improvement, stakeholder engagement, clinical informatics, research and staff management (Allison, 2014; Bhatt, 2021; Kilkenny, 2014; Ryan et al., 2024; Walker, 2010). The expertise of HIMs in health data integrity, interpretation of coded data, ethical practices and management of health record systems and policies is an asset to clinical registries (Robinson and Lee, 2021). These skills uniquely position HIMs to contribute to a range of agreed national priority areas for clinical registries such as timely access to and reporting of data, registry and data governance, national health data and terminology standards, interoperability with electronic medical records and patient privacy (Australian Government Department of Health, 2021).
Funding support was identified as a barrier to job satisfaction of HIMs at clinical registries. It is well established that Australian clinical registries require sustainable long-term funding (Ahern, 2023a; Parker et al., 2023). Despite the importance of clinical registries to monitor the quality of care and outcomes, very few are government funded, and the majority are funded by industry or not-for-profit organisations (Ahern, 2023b). Insufficient funding may restrict the activities of clinical registries to support only the essential tasks of data collection, management and reporting. Increased and sustainable funding may facilitate secure employment of HIMs at more clinical registries, and expansion of their roles and responsibilities beyond “core business” activities (e.g. research, system interoperability).
Our results confirm that the skillset of HIMs aligns well with the critical functions of clinical registries. However, not all clinical registries employ HIMs, nor are their professional skills utilised to their full potential. This finding is concordant with issues surrounding the professional identity of the health information management profession that has been investigated in previous studies. For example, research has highlighted that HIMs have difficulty describing their profession to others as “no one ever knows what we do” (Nexhip et al., 2024). HIMs report that they value being seen as an expert in their field (Nexhip et al., 2025), which may be difficult to achieve when the profession and core knowledge base of qualified HIMs is not well understood by potential and current employers. There is a workforce shortage of HIMs in Australia, and often other disciplines substitute into the role of HIMs without an equivalent understanding of health information management (Robinson and Lee, 2021). Ongoing advocacy is required to increase the awareness of the health information management profession, to increase the number and scope of practice of HIMs working at clinical registries.
Strengths and limitations
This is the first study into an area of the profession that has not been investigated previously in Australia. The strengths of this study included adapting a previously developed survey, which was informed by multiple health information management workforce experts. We also obtained multiple perspectives to understand the workforce, and roles and responsibilities of HIMs at Australian clinical registries.
This study is limited by a small sample size. The number of HIMs working at Australian clinical registries is estimated to be small, but cannot be quantified accurately. Therefore, it is unknown how generalisable these results are. Approximately one-third of clinical registries responded to our survey, and there may be a participation bias towards registries who employed HIMs. In this study, we did not include population-based screening services, which may be an important area for future studies.
The majority of respondents graduated from institutions in Victoria. This may be explained by the distribution of accredited HIMs courses in Australia, and that almost half of HIMs work in Victoria (Jobs and Skills Australia, 2024). We acknowledge that many clinical registries are affiliated with organisations based in Victoria; however, we cannot ascertain the exact geographical location of each registry as this information is not included in the Australian Register of Clinical Registries (Australian Commission on Safety and Quality in Health Care, 2024c).
Participation in both surveys relied on self-identification of HIMs working at clinical registries. In particular, data custodians were not asked to specify the qualifications of HIMs employed at their clinical registry. Clinical registry duties readily fulfilled by HIMs may be undertaken by other health information professionals (i.e. people without an accredited health information management qualification) working in similar roles. It is also noted that some respondents to the data custodian survey reported that HIMs at their clinical registry used skills which are outside the scope of a HIM (e.g. specimen collection, clinical work). These responses suggest a potential misidentification of HIMs at clinical registries. Regardless of whether the data custodians were referring to HIMs with a clinical background, clinical skills are not within scope and would not be used in a HIM role. These responses may limit the accuracy of the results of the data custodian survey.
Conclusion
HIMs fulfil a diverse range of roles and responsibilities at Australian clinical registries which extend across most domains of health information management professional competence. While the overall number of HIMs employed at clinical registries in Australia is likely to be low, their skills align well with the core operational requirements and future vision for clinical registries. Not all clinical registries employ HIMs, and some HIMs who work at clinical registries are underutilised in their roles. Ongoing advocacy is required to increase the understanding of the professional competencies of HIMs at clinical registries.
Supplemental Material
sj-docx-1-him-10.1177_18333583251344982 – Supplemental material for Exploration of the role of health information managers in the world of clinical registries
Supplemental material, sj-docx-1-him-10.1177_18333583251344982 for Exploration of the role of health information managers in the world of clinical registries by Catherine Burns, Ailie Sanders, Merilyn Riley, Olivia Ryan and Monique F Kilkenny in Health Information Management Journal
Footnotes
Acknowledgements
We would like to acknowledge Dr Lee Nedkoff and Miriam Lum On for their suggestion to survey senior leaders at clinical registries about their perspective of HIMs. We also thank Dr Tharshanah Thayabaranathan for proof-reading the manuscript.
Accepted for publication May 10, 2025.
Author contributions
CB was responsible for formal analysis, data validation and writing the original draft. AS was responsible for formal analysis and data validation. MFK was responsible for supervision. All authors contributed to the conceptualisation, methodology and were responsible for reviewing and editing the manuscript for intellectual content. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: MFK is a member of the Australian Stroke Clinical Registry Management Committee and an Associate Editor of the Health Information Management Journal Editorial Board. CB, MR and OR are members of the Health Information Management Journal Editorial Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: No specific funding was obtained for this study. MFK received fellowship support from the National Heart Foundation of Australia (#105737).
Ethical considerations
Ethics approval for this study was obtained from Monash University Human Research Ethics Committee in Victoria, Australia (Project ID: 45658).
Consent to participate
Details of the study, including the explanatory statement, were provided in the invitation email and within the REDCap survey, and consent was obtained from participants though their agreement to access and complete the online survey.
ORCID iDs
Data availability statement
The data that support the findings of this study are available from the corresponding author (MFK) upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.