
Abstract
Background:
Axial spondyloarthritis (axSpA) patients are known to have a higher prevalence of several comorbidities, including, among others, an increased risk of atherosclerosis, hypertension, dyslipidemia, and diabetes. The purpose of the present study was to determine whether the sum of traditional cardiovascular (CV) risk factors is related to disease characteristics, such as disease activity, in patients with axSpA.
Methods:
A cross-sectional study that encompassed 804 patients with axSpA was conducted. Patients were assessed for the presence of five traditional CV risk factors (diabetes mellitus, dyslipidemia, hypertension, obesity, and smoking status), and disease activity measurements. A multivariable regression analysis was performed to evaluate whether the number of classic CV risk factors was independently associated with specific features of the disease, to include disease activity.
Results:
A multivariable analysis showed that Ankylosing Spondylitis Disease Activity Score–C reactive protein (ASDAS-CRP) activity score was significantly higher in patients with 1 [beta coefficient 0.3 (95% confidence interval (CI) 0.1–0.5), p = 0.001] and ⩾2 [beta coefficient 0.5 (95% CI 0.3–0.7), p = 0.000] CV risk factors compared with those without CV risk factors. Similarly, patients with 1 [OR 2.00 (95%CI 0.99–4.02), p = 0.053] and ⩾2 [OR 3.39 (95%CI 1.82–6.31), p = 0.000] CV risk factors had a higher odds ratio for the presence of high disease activity compared with the zero CV category. The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) activity score was significantly associated with the number of CV risk factors, being higher in patients with more CV risk factors. These relationships showed a CV risk factor-dependent effect being beta coefficients and ORs higher for the effect of ⩾2 over 1 CV risk factor.
Conclusion:
Among patients with axSpA, as the number of traditional CV risk factors increased, disease activity similarly increases in an independent manner.
Introduction
The term axial spondyloarthritis (axSpA) refers to a family of disorders, including ankylosing spondylitis or radiographic axial spondyloarthritis. In addition, non-radiographic axial spondyloarthritis can be accompanied by psoriasis, inflammatory bowel diseases, and other conditions. The different forms of axSpA share a group of clinical features including inflammation of axial joints (especially the sacroiliac joints), asymmetric oligoarthritis (especially of the lower extremities), dactylitis, and enthesitis. Moreover, axSpA has been associated with co-morbidities that include, among others, cancer, infections, osteoporosis, and cardiovascular (CV) risk factors and established CV disease. 1 With respect to the latter, several studies have suggested an increased risk of hypertension, type 2 diabetes, obesity, and dyslipidemia in axSpA compared with healthy populations, as was observed with the ASAS-COMOSPA cohort.2,3 In addition, CV risk algorithms applied to the general population in order to calculate CV risk have been found to exhibit a poor discrimination ability in patients with axSpA.4,5
Despite non-modifiable CV risk factors that include age, gender, and family history of CV disease, there are five classic modifiable CV risk factors (hypertension, smoking, dyslipidemia, diabetes, and obesity) that are estimated to account for more than 50% of all CV deaths. 6 It is known that the absence of these major CV risk factors predicts a much lower risk of coronary heart disease. 7 It is also accepted that, after adjusting for age and sex, the odds of developing CV disease increases with the number of risk factors present [odds ratio (OR) 2.4, 4.2, 4.9, and 7.2 for 1, 2, 3, and 4 or more risk factors, respectively, compared with no risk factors]. 8 The co-occurrence of these traditional CV risk factors has been linked to pathways sharing common underlying mediators and mechanisms related to inflammation.9–11 This means that inflammatory processes are involved in not just a few select disorders like inflammatory arthritis, but also in others that include CV risk factors and, eventually, CV disease.
Although the presence of CV comorbidity in axSpA has been studied, the way in which CV risk factors correlate with disease-related data has not been explored before. In this study, we aimed to assess whether axSpA patients with a higher number of CV risk factors have higher disease activity, or if these number of CV risk factors is related to other disease characteristics.
Materials and methods
Study participants
This was a cross-sectional study that included 804 patients with axSpA. All of them were 18 years old or older. axSpA patients included in this study fulfilled the Assessment of Spondyloarthritis International Society (ASAS) classification criteria. 12 They were diagnosed by rheumatologists and periodically followed up at rheumatology outpatient clinics. For the purpose of inclusion in the present study, axSpA disease duration needed to be ⩾1 year. axSpA patients undergoing biologic therapy [anti-tumor necrosis factor (TNF) alpha therapies and others) were not excluded from the present study. Likewise, since glucocorticoids may be used in the management of axSpA, patients taking prednisone at an equivalent dose ⩽10 mg/day, were not excluded. Moreover, patients were excluded if they had a history of CV events, cancer or any other chronic disease, or evidence of active infection or a glomerular filtration rate <60 ml/min/1.73 m2. Therefore, none of the patients had a history of ischemic heart disease, cerebrovascular accidents, or peripheral arteriopathy. All of the axSpA patients came from a Spanish multicenter cohort study of atherosclerosis in axSpA involving 10 different Spanish hospitals. Patients were recruited consecutively from those centers between 2013 and 2018. The study protocol was approved by the Institutional Review Committee of each hospital, all of them in Spain (approval number 2016.052). Subjects provided informed written consent. Research carried out with human subjects was in compliance with the Declaration of Helsinki.
Data collection
Surveys of axSpA patients were performed to assess CV risk factors and medication. Subjects completed a questionnaire and underwent a physical examination to determine anthropometric measurements and blood pressure. Medical records were reviewed to ascertain specific diagnoses and medications. Five CV risk factors were defined at study onset: (1) Dyslipidemia was established if one of the following factors was present: total cholesterol >200 mg/dl, triglycerides >150 mg/dl, HDL-cholesterol <40 mg/dl in men or <50 mg/dl in women, or LDL-cholesterol >130 mg/dl; (2) hypertension was defined as a systolic or a diastolic blood pressure higher than, respectively, 140 and 90 mmHg; (3) obesity was defined as a body mass index equal or higher than 30 kg/m2; (4) smoking if currently active; and (5) diabetes mellitus if glycemia exceeded 126 mg/dl or patients were on glucose-lowering drugs or insulin therapy. The atherogenic index was calculated using the total cholesterol/HDL cholesterol ratio. Two clinical indexes of disease activity [Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Ankylosing Spondylitis Disease Activity Score (ASDAS)],13,14 a functional status index [Bath Ankylosing Spondylitis Functional Index (BASFI)], 15 a metrological index [Bath Ankylosing Spondylitis Metrology Index (BASMI)], 16 and an enthesitis index [Maastricht Ankylosing Spondylitis Enthesitis Score (MASES)] 17 were assessed in all patients at the time of their evaluation visit. Information on any history of hip involvement, synovitis, enthesitis, and extraarticular manifestations (anterior uveitis, psoriasis, and inflammatory bowel disease), HLA-B27 status and disease duration was also assessed. Structural damage was assessed by the modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS) 18 and the presence of syndesmophytes on spinal radiographs. The patients also underwent a standard anteroposterior plain radiograph of the pelvis to classify them as ankylosing spondylitis or nr-axSpA. Positive sacroiliitis in magnetic resonance imaging (MRI) was defined if active sacroiliitis or chronic changes were present. Furthermore, high-sensitivity C-reactive protein (CRP) was assessed, and standard techniques were used to measure serum lipids.
Statistical analysis
Demographic and clinical characteristics in patients with axSpA are expressed as the mean ± standard deviation (SD) or percentages for categorical variables. For non-normally distributed continuous variables, data are expressed as median and interquartile range (IQR). Univariate differences between patients with 0, 1, and 2 or more CV risk factors were assessed through an analysis of variance (ANOVA) or Kruskall–Wallis tests according to normal distribution or the number of subjects. The relationships between the number of CV risk factors and disease-related data, including disease scores, were assessed through multivariable logistic, linear, and multinomial regressions. These associations were adjusted for confounders with a p value less than 0.20 in the univariable analysis, using patients with zero CV risk factors as the reference category. Diagnostics for regression models were tested by studying the residuals plots of each model. All of the analyses used a 5% two-sided significance level and were performed using SPSS software, version 24 (IBM, Chicago, IL, USA). A p value < 0.05 was considered statistically significant.
Results
Demographic and disease-related data
A total of 804 axSpA patients with a mean ± SD age of 48 ± 12 years were included in this study. The frequency and percentages of the five CV risk factors, as well as the demographic and disease-related characteristics of the participants, are shown in Table 1. While 31% (n = 250) of the patients did not have CV risk factors, the presence of 1, 2, and 3 or more CV risk factors was observed in 35% (n = 285), 21% (n = 168), and 13% (n = 101) of patients, respectively.
Main demographics, cardiovascular risk factors, and disease-related data in spondyloarthritis patients.

Data represent means ± SD or median (IQR) when data were not normally distributed.
ASDAS-CRP categories were defined as: disease activity <1.3 inactivity; ⩾1.3 to <2.1 low disease activity; ⩾2.1 to <3.5 high disease activity; ⩾3.5 very high disease activity. ASDAS-CRP was not available in 213 patients.
ASDAS, Ankylosing Spondylitis Disease Activity Score; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; CRP, C-reactive protein; CV, cardiovascular; DMARD, disease-modifying antirheumatic drug; ESR, erythrocyte sedimentation rate; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; MASES, Maastricht Ankylosing Spondylitis Enthesitis Score; MRi, magnetic resonance imaging; mSASSS, Modified Stoke Ankylosing Spondylitis Spinal Score; NSAID, nonsteroidal anti-inflammatory drugs; Obesity, BMI > 30 kg/m2; TNF, tumor necrosis factor.
The median axSpA disease duration was 8 years (IQR 2–17). The ASDAS-CRP score was 2.3 ± 1.0, and 38% of the patients were in the high activity category. The BASDAI total score was 3.7 (IQR 1.8–5.5) and 44% of the patients had a BASDAI ⩾4. The BASFI and BASMI scores were, respectively, 3.5 ± 2.6 and 2.7 ± 2.0. The median CRP was 2.2 (IQR 0.6–6.2) mg/l and HLA-B27 was present in 70% of subjects. A total of 82% of the patients were taking nonsteroidal anti-inflammatory drugs (NSAIDs), 16% were on methotrexate, and 34% were receiving TNF-alpha inhibitors. Additional axSpA information regarding disease features is shown in Table 1.
Number of CV risk factors and association with disease-related data
Differences in demographics, CV risk factors, and disease-related data between the different number of CV risk factors in axSpA patients is shown in Table 2. As expected, most of the CV disease-related data increased as the number of CV risk factors also rose. In this sense, the frequency of male sex, age, lipid profiles (with the exception HDL-cholesterol), and the use of statins were higher in patients with 1 and ⩾2 CV risk factors compared with those without any. These differences remained, in general, statistically significant, even after adjusting for age and sex.
Differences in demographics, cardiovascular risk factors, and disease-related data vis-à-vis the number of CV risk factors in axSpA patient groups.

Data represent means ± SD or median (IQR) when data were not normally distributed.
Both logistic and linear regression analysis, adjusted for age and sex, were used to assess the effect of 1 CV and ⩾2 CV risk factors versus none. In this analysis, the number of CV risk factors is considered the independent variable.
Multivariable analysis was only performed for variables that showed differences in the univariable analysis with a p value < 0.20.
axSpA, axial spondyloarthritis; BMI, body mass index; CRP, C-reactive protein; CV, cardiovascular; DMARD, disease-modifying antirheumatic drug; ESR, erythrocyte sedimentation rate; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; MRi, magnetic resonance imaging; mSASSS, Modified Stoke Ankylosing Spondylitis Spinal Score; NSAID, nonsteroidal anti-inflammatory drugs; Obesity, BMI > 30 kg/m2; TNF, tumor necrosis factor.Significant p values are depicted in bold.
Regarding disease-related data, the presence of syndesmophytes, the use of anti-TNF inhibitors, and CRP at disease onset were higher in patients with ⩾2 CV risk factors compared with those with none. In addition, patients with one CV risk factor had a lower frequency of total extraarticular manifestations and uveitis when compared with those with no CV risk factors. All of the aforementioned differences were found after correcting for age and sex.
Relation of CV risk factors to disease-related scores, including disease activity
In general, the majority of disease-related scores associated with disease activity, functional and metrological features, and enthesitis proved higher, in the univariable analysis, as did the number of CV risk factors (Table 3).
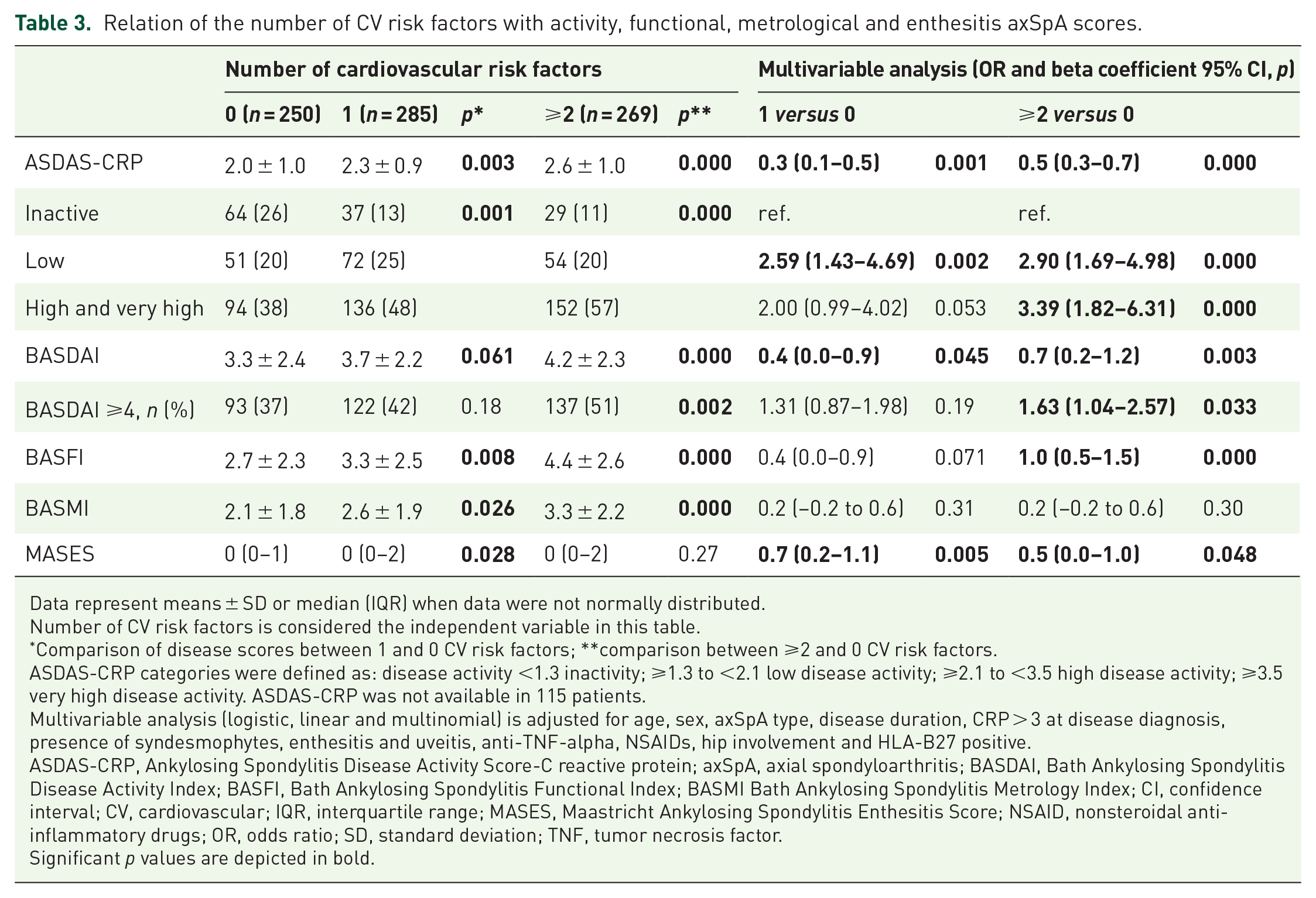
Relation of the number of CV risk factors with activity, functional, metrological and enthesitis axSpA scores.
Data represent means ± SD or median (IQR) when data were not normally distributed.
Number of CV risk factors is considered the independent variable in this table.
Comparison of disease scores between 1 and 0 CV risk factors; **comparison between ⩾2 and 0 CV risk factors.
ASDAS-CRP categories were defined as: disease activity <1.3 inactivity; ⩾1.3 to <2.1 low disease activity; ⩾2.1 to <3.5 high disease activity; ⩾3.5 very high disease activity. ASDAS-CRP was not available in 115 patients.
Multivariable analysis (logistic, linear and multinomial) is adjusted for age, sex, axSpA type, disease duration, CRP > 3 at disease diagnosis, presence of syndesmophytes, enthesitis and uveitis, anti-TNF-alpha, NSAIDs, hip involvement and HLA-B27 positive.
ASDAS-CRP, Ankylosing Spondylitis Disease Activity Score-C reactive protein; axSpA, axial spondyloarthritis; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI Bath Ankylosing Spondylitis Metrology Index; CI, confidence interval; CV, cardiovascular; IQR, interquartile range; MASES, Maastricht Ankylosing Spondylitis Enthesitis Score; NSAID, nonsteroidal anti-inflammatory drugs; OR, odds ratio; SD, standard deviation; TNF, tumor necrosis factor.Significant p values are depicted in bold.
The ASDAS-CRP activity score was significantly higher in patients with 1 [beta coefficient 0.3 (95% confidence interval (CI) 0.1–0.5, p = 0.001] and ⩾2 [beta coefficient 0.5 (95% CI 0.3–0.7), p = 0.000] CV risk factors compared with those without any CV risk factors. This relation was found using either ASDAS-CRP as a continuous or categorical variable. In this regard, patients with 1 [OR 2.00 (95% CI 0.99–4.02), p = 0.053] and ⩾2 [OR 3.39 (95% CI 1.82–6.31), p = 0.000] CV risk factors had a higher OR for the presence of high and very high disease activity compared with the zero CV category. These relations were found in the fully multivariable analysis, which included age, sex, axSpA type, disease duration, CRP at time of study, CRP >3 at disease diagnosis, the presence of syndesmophytes, enthesitis and uveitis, current use of TNF-alpha inhibitors and NSAIDs, history of hip involvement, and HLA-B27 status. Similarly, the BASDAI score, which also measures disease activity, was significantly associated with the number of CV risk factors, being higher in those patients who had more CV risk factors (Table 3). Interestingly, these relationships revealed a dose-dependent effect: beta coefficients and ORs were higher when the effect of ⩾2 CV risk factors, versus just 1, was studied.
Other relationships were observed in scores related to functional, metrological, and enthesitis. For example, the presence of ⩾2 CV risk factors was associated with a higher BASFI score, and MASES was found to be significantly higher in patients with 1 CV and 2 or more CV risk factors (Table 3).
Discussion
Low-grade chronic inflammation is now widely accepted to be associated with conventional CV risk factors in the general population. Moreover, a link between traditional CV risk factors, CV disease, and inflammation may also exist. According to our results, CV risk factors in patients with axSpA may correlate not only with CV disease, but also with features related to the disease, such as disease activity.
The prevalence of CV risk factors and CV disease itself represent a considerable burden in patients with axSpA. For example, several previously described analyses based on the ASAS-COMOSPA International Cohort revealed higher prevalences of hypertension, type 2 diabetes, ischemic heart disease, smoking, dyslipidemia, obesity, etc., in these patients.2,19 Our study, in which 69% of the patients had at least one CV risk factor, supports this notion. Moreover, an ancillary study of the same ASAS-COSMOPA project showed that the CV risk factor burden was largest in the peripheral axSpA group. 2 These findings were in keeping with our results, suggesting that disease characteristics and traditional CV risk factors may be interconnected.
Many studies have focused on the role of inflammation as a common mediator in several CV risk factors. For example, obesity and type 2 diabetes have been linked in this way. In fact, factors released by adipose tissue, such as adipokines, are known to stimulate inflammatory activity, which correlates with insulin resistance. 20 In addition, metabolic syndrome, a constellation of different CV risk factors, has been recognized as a proinflammatory, prothrombotic state, and is associated with elevated levels of CRP, interleukin-6, and plasminogen activator inhibitor-1.21,22 The contention that inflammation underlies CV risk factors is also supported by the fact that the anti-inflammatory properties of certain medications, including thiazolidinediones and statins, may contribute therapeutic benefits beyond their propensity to lower glucose and cholesterol levels, respectively. 23 Moreover, among patients with rheumatoid arthritis or psoriasis, the use of anti-inflammatory, disease-modifying antirheumatic drugs, such as TNF inhibitors and hydroxychloroquine, is associated with a lower incidence of diabetes than other agents. 24 Although we have not assessed the links between cytokines or adipokines and inflammation in this study, we believe our results are likely in agreement with all of the aforementioned concepts: CV risk factors through hitherto unknown mechanisms could exert inflammatory effects on a disease that is already inflammatory in itself. 25
In a previous work by our group, the number of CV risk factors was associated with disease activity in patients with psoriatic arthritis. 26 In this study, 305 patients were assessed for the presence of six traditional CV risk factors (diabetes mellitus, dyslipidemia, hypertension, obesity, chronic kidney disease, and smoking status). After multivariable analysis, psoriatic arthritis patients with a higher number of CV risk factors exhibited upregulated disease activity compared with those without them. This occurred independently of disease duration and other demographics factors. The fact that we have found similar results in axSpA patients reinforces the contention that CV risk factors most likely interact with features of the disease in a deleterious manner.
In our work we assessed various scores vis-à-vis different disease aspects related to activity, functionally, metrology, etc. Interestingly, the number of CV risk factors correlated with all of these aspects and not just one. Since these scores are constructed differently, we believe our findings supports the contention that this association does exist.
One limitation of our study was that we did not record the duration or severity of the CV factors, or whether they were present before or after diagnosis of the disease. We additionally could not determine how, or to what degree, certain combinations of CV risk factors interact in their effect on the disease. Moreover, the quantity of previous DMARDs or anti TNF-α treatments, as well as cumulative NSAID dosages, were not assessed in our study. We also understand that other comorbidities such as depression, impaired physical activity, family history of CV disease, lifestyle habits like alcohol and diet, etc., were not assessed in our study. For example, the subject of physical activity is of interest since patients with high disease activity may exercise less and have a more sedentary lifestyle due to pain, resulting in an accumulation of CV risk factors. Furthermore, we recognize that our study is cross-sectional in nature, which makes it difficult to determine the direction of causality. For this reason, our reported results require confirmation in future longitudinal studies.
In conclusion, the sum of traditional CV risk factors correlates with a higher disease activity in patients with axSpA. Our findings support the argument that control of CV risk factors may have beneficial effects not only on CV disease and/or CV events, but also on disease control, since they correlate with higher disease activity. Conversely, controlling disease activity could also have a positive effect in controlling CV risk factors. The network of interconnected effects between CV risk factors and inflammation warrants further research.
Footnotes
Acknowledgements
We thank the Sociedad Española de Reumatología for the English-language revision of this manuscript.
Conflict of interest statement
MAG-G and IF-A would like to acknowledge that they received grants/research supports from Abbott, MSD, Jansen, and Roche, as well as consultation fees from company-sponsored speakers bureaus associated with Abbott, Pfizer, Roche, Sanofi, Celgene, and MSD.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant to MAG-G from the Instituto de Salud Carlos III (ISCIII) (Fondo de Investigación Sanitaria grants PI06/0024, PI09/00748, PI12/00060, PI15/00525, PI18/00043) and the ISCIII RETICS programs (RD12/0009 and RD16/0012).
ORCID iDs
Data availability
The data underlying this article will be shared upon reasonable request to the corresponding authors.