
Abstract
Background:
Opioids are widely used in moderate-to-severe chronic pain which is non-responsive to standard analgesics. Prescriptions have increased in Europe in the last decade, although remain lower than in USA. This work projected the future utilization and costs of opioids in chronic osteoarthritis (OA) pain in the Spanish National Health System (NHS).
Methods:
An epidemiological model was populated with the opioid dispensing trends from 2010 to 2019 using Spanish Medicinal Agency rates of opioid utilization in subjects over 18 years of age and the real-world OPIOIDS study to estimate chronic-OA-pain patients receiving opioids. A best-fitted trend analysis model was applied estimating the likely number of DHD (defined daily dose/1000 inhabitants per day) to calculate projected opioid utilization and costs for the period 2020–2029.
Results:
In 2010, an estimated 5.67 DHD were dispensed for the equivalent of 217,076 chronic OA pain patients per day [1.99 DHD, 76,084 refractory to non-steroidal anti-inflammatory drugs (NSAIDs)]. From these trends and OA prevalence, the projected number of DHDs is expected to increase more than threefold to 17.98 DHDs by the year 2029 for the equivalent of 727,356 chronic OA pain patients per day (8.18 DHD, 330,720 refractory to NSAIDs); 41.8% on strong opioids. The estimated cost was €116.9m (€45.0m in NSAID-refractory OA) in 2010 rising by 222% to €376.1m (€199.7m refractory to NSAIDs) by 2029.
Conclusion:
Chronic-OA-pain-related opioid dispensing and costs to the NHS are set to increase more than threefold from 2010 to 2029 in Spain. Using opioids for OA pain is concerning given disease chronicity and other related costs not computed in these projections.
Plain language summary
• Opioids are widely used in chronic pain which is non-responsive to standard analgesics. Prescriptions have increased in Europe, although remain lower than in USA. Osteoarthritis (OA) is a degenerative joint disease usually accompanied by pain. Despite not recommended, opioids use in OA have been expanded because this health condition is increasing with ageing and, also, because physicians both primary and specialist boosted their use.
• This study aimed to quantify the current burden of opioids used for chronic moderate-to-severe OA pain by estimating the number of defined daily doses per 1000 inhabitants per day (DHD) and associated costs, and to forecast the likely burden on the National Health System (NHS) in Spain for the years 2020–2029.
• In 2010, an estimated 5.67 DHDs were dispensed for the equivalent of 217,076 chronic OA pain patients per day. From these trends, the projected number of DHDs is expected to increase more than threefold to 17.98 DHDs by the year 2029 for the equivalent of 727,356 chronic OA pain patients per day; 41.8% on strong opioids. The estimated cost was €116.9m in 2010 rising by 222% to €376.1m by 2029.
• Chronic OA-pain-related opioid dispensing and costs to the NHS are set to increase substantially (threefold to more than fourfold) from 2010 to 2029 in Spain. Thus, using opioids for OA pain is concerning given disease chronicity, aging population and other related costs not computed in these projections. Our findings can inform payors and clinicians about ongoing discussions on appropriate analgesic management for longer-term OA pain, including resource requirements at a national level. Clinicians who prescribe opioids for OA pain should consider the potential implications of side effects such as sedation, cognitive deterioration, incremental need of caregivers, particularly in older people, and carefully consider the risk–benefit balance.
Introduction
Pain is defined as an unpleasant sensory or emotional experience resulting from real or potential tissue damage. 1 It is a major health problem, with chronic pain, which lasts longer than 3 months, being one of the main causes of medical consultations.1,2 More than three-quarters of patients with chronic pain receive drug treatment to lessen the intensity of pain, and two-thirds of the pain population resort to medical visits as their main pain-management strategy.2,3 Osteoarthritis (OA) is a degenerative joint disease characterized by cartilage deterioration and inflammation of the synovial membrane in the joint, and it is accompanied most of the time by joint malfunction and chronic pain.4,5 Treatment of chronic pain in OA patients includes both pharmacological and non-pharmacological strategies.6,7 Among the pharmacological drugs are non-opioid analgesics, opioids and adjuvants. Opioid drugs are a group of drugs characterized by selective affinity for central and peripheral opioid receptors by inhibiting the transmission of nociceptive entry and pain perception.6,7 However, these drugs are not recommended to treat OA pain by Osteoarthritis Research Society International or the American College of Rheumatology, among other entities.8,9 Nonetheless, these medications are widely prescribed for the treatment of severe acute pain, and also in OA patients with chronic moderate to severe pain that does not respond to other treatments, despite mounting evidence questioning the benefits.10–12 Nowadays, OA prevalence is the highest among all rheumatological diseases.13,14 In Spain, OA affects up to 29.4% of people aged 40 or older, 15 with pain as a core symptom in many patients: up to 56.5% of OA patients suffered from moderate to severe pain according to the 2017 Spanish National Health Survey (SNHS). 16 This health condition can have a tremendous individual and socioeconomic burden.17–21 According to the landmark Global Burden of Disease study, OA is now the 13th leading cause of disability worldwide. 22 Using data from the 2017 SNHS, it has been estimated that chronic OA pain is a considerable source of burden to society and the health system; on average, patients with OA lost 35.6% of their life expectancy due to disability (Disability-Adjusted-Life-Expectancy loss of 3.5 years per patient). 23 Likewise, OA exerts a significant impact on healthcare systems, given the substantial costs associated with joint replacement surgery, specialist consultation and the use of prescription medicines, amongst other resources, to manage moderate to severe pain.19–21,24 In Spain, OA healthcare costs were on average €2274 per patient per year; projecting the actual prevalence of OA, 15 the actual national costs would be €11.2bn, or 0.96% of the 2017 Spanish gross domestic product. 24
On the other hand, there was a worldwide doubling in the use of opioids for pain relief between the years 2010 and 2019, with high levels of opioid use evident in developed Western countries.25–28 Opioids have the potential to cause harm, both short- and long-term, in all subjects but mainly in elderly OA patients who are taking multiple medicines and have an increased risk of accidents and fractures. 29 There is also a potential risk of dependence, overdose, and death. Despite limited evidence to support longer-term opioid use, they are habitually used to treat chronic pain associated with OA and non-cancer pain. In Spain, opioid use also doubled in the period between years 2010 and 2019, 30 with more than two-thirds being prescribed by primary care physicians for OA of any joint. 31
This study aimed to quantify the current burden of opioids used for chronic moderate-to-severe OA pain by estimating the number of defined daily doses per 1000 inhabitants per day and associated costs, and to forecast the likely burden on the National Health System (NHS) in Spain for the years 2020–2029.
Methods
Study design and reporting guidelines
An epidemiological longitudinal and prospective model was designed and populated with aggregate data available in the public domain only. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting guidelines were used to write this article. 32 Supplemental material online includes a completed CHEERS checklist reviewing the most critical steps carried out in the economic analysis.
Data sources
Data sources used to populate the epidemiological model included trends in opioids dispensing from the years 2010–2019 using Spanish Medicinal Agency (AEMPS) rates of opioid prescribing in people over the age of 18 years (see below); 30 the real-world OPIOIDS (Outcomes in Patients usIng Opioids In Painful Disorders in Spain) study to estimate moderate-to-severe chronic OA pain patients receiving opioids and patients with chronic OA pain which is refractory to non-steroidal anti-inflammatory drugs (NSAIDs);31,33 a study on the prevalence of rheumatic diseases conducted recently by the Spanish Association of Rheumatology, the EPISER study; 15 and the Spanish Drug-Catalogue for opioid drug costs (Table S1 in the Supplemental material). 34 AEMPS, as a state agency attached to the Spanish Ministry of Health, is responsible for guaranteeing to society, from a public service perspective, the quality, safety, efficacy and correct information regarding medicines and medical devices. To this end, it carries out a wide range of activities, including, but not limited to, the continuous monitoring of the safety and efficacy of medicines once marketed and quality control. Due to this, the AEMPS continuously monitors the use of opioids, among other drugs, in Spain by conducting drug utilization or pharmacoepidemiologic studies. The prescription billing information of the Spanish NHS managed by the General Directorate of Pharmacy and Sanitary Products (DGFPS, acronism in Spanish) is used for these studies. This database contains the number of packages provided in community pharmacy settings under the NHS and is populated by the data provided by all the different Autonomous Communities of Spain. Following the recommendations of the World Health Organization (WHO) on Drug Use Studies, 35 drug use has been expressed in defined daily doses (DDDs) per 1000 inhabitants per day (DHD). DDD is a technical unit of measurement that corresponds to the maintenance dose for the main indication, for a given route of administration, in adults. The DDDs of the active substances are established by the WHO and are published on the WHO Collaborating Centre for Drug Statistics Methodology website. 35 For those active substances whose DDD has not been defined, it is approximated using the recommended dose in the literature and in the corresponding data sheet of the medicinal product. Official population figures are obtained from the National Statistics Institute (data from the standard municipality and census projections) and are available for consultation. 36 The calculation of DHDs from the number of packs dispensed is carried out using the following formula: DHD = (UV × FF × C × 1000)/(DDD × Number of inhabitants × 365 days), where UV = packaging units sold, FF = number of pharmaceutical forms per packaging and C = amount of active substance in each pharmaceutical form. As an example, a use of 20 DHD in a given year can be interpreted as if on each day of that year an average of 20 out of every 1000 inhabitants received a DDD of the medicinal product.
Model development
Opioids were defined by the international Anatomical Therapeutic Chemical classification as ‘N02A’, including both weak and strong opioids, as recommended by the WHO collaborating centre for drug statistic methodology.28,35 Medications included in the analyses were those included in the prescription billing information of the Spanish NHS, managed by the DGFPS, listed in the ‘Nervous System-Analgesics-Opioids’ category and prescribed by a family medicine physician or a specialist exclusively in any of the available forms. The incidence of patients receiving opioid medications used in chronic OA pain, as recorded in the OPIOIDS study, was included in the analysis to project national opioid utilization, both in terms of type of opioid and the percentage distribution used.31,33 The total number of dispensed opioid DHDs within the NHS in Spain for any reason for each financial year from 2010 to 2019 (as reported by the AEMPS) was plotted in Microsoft Excel and a trend line of best fit was added for any opioid analysed individually. Lineal, logarithmic, power, exponential, quadratic and cubic trend line options were explored to choose the best fit using R 2 statistic. Projections were computed for a period similar to those of the fiscal years recorded (10 fiscal years), thus, projections were for the years 2020–2029 (inclusive). This approach has already been followed by other investigators previously. 28
To estimate OA opioid consumption projections, we first projected all opioid use for any reason and expressed it in DHDs from the data provided by the AEMPS in years 2010–2019 (Figure S1 and S2, Table S2, Supplemental material). 30 Then, we estimated the proportion of DHDs corresponding to OA patients with moderate-to-severe chronic pain from the OPIOIDS study for each individual opioid drug dispensed in that real-world study (Tables S3–S6, Supplemental material)31,33. As opioids share, in percentage, observed in the OPIOIDS study evolved from one year to the following, the opioid utilization share was projected to fiscal years 2020–2020 by using a trend line of best fit analysis using the opioid utilization share evolution observed in the OPIOIDS study. Table 1 shows the different equations fitted with a corresponding R2 statistic for each opioid drug. Then, total opioid DHDs were calculated. Once DHDs values was known, both observed and projected, the number of OA patients taking a DDD in each year was estimated by multiplying the census in the year by the DHD value. Reimbursed costs for dispensed opioid prescriptions were obtained from the Spanish Drug Catalogue (Table S7, Supplemental material). 34 DDD cost was estimated by summing the Public Selling Price (PSP) of each opioid weighted by its use in each year, both observed and projected. Cost data for the NHS by year was computed by multiplying the estimated annual projected population from the census in the year and the expected cost of each opioid DDD in that year using PSPs. Using the above data inputs, a final model was developed to forecast the likely number of dispensed opioid prescriptions for OA and associated costs to the NHS (reported as total costs) for 2020–2029. All costs are reported in 2019 euros.
Trend line of best-fitted equations by type of opioid used in model projections.
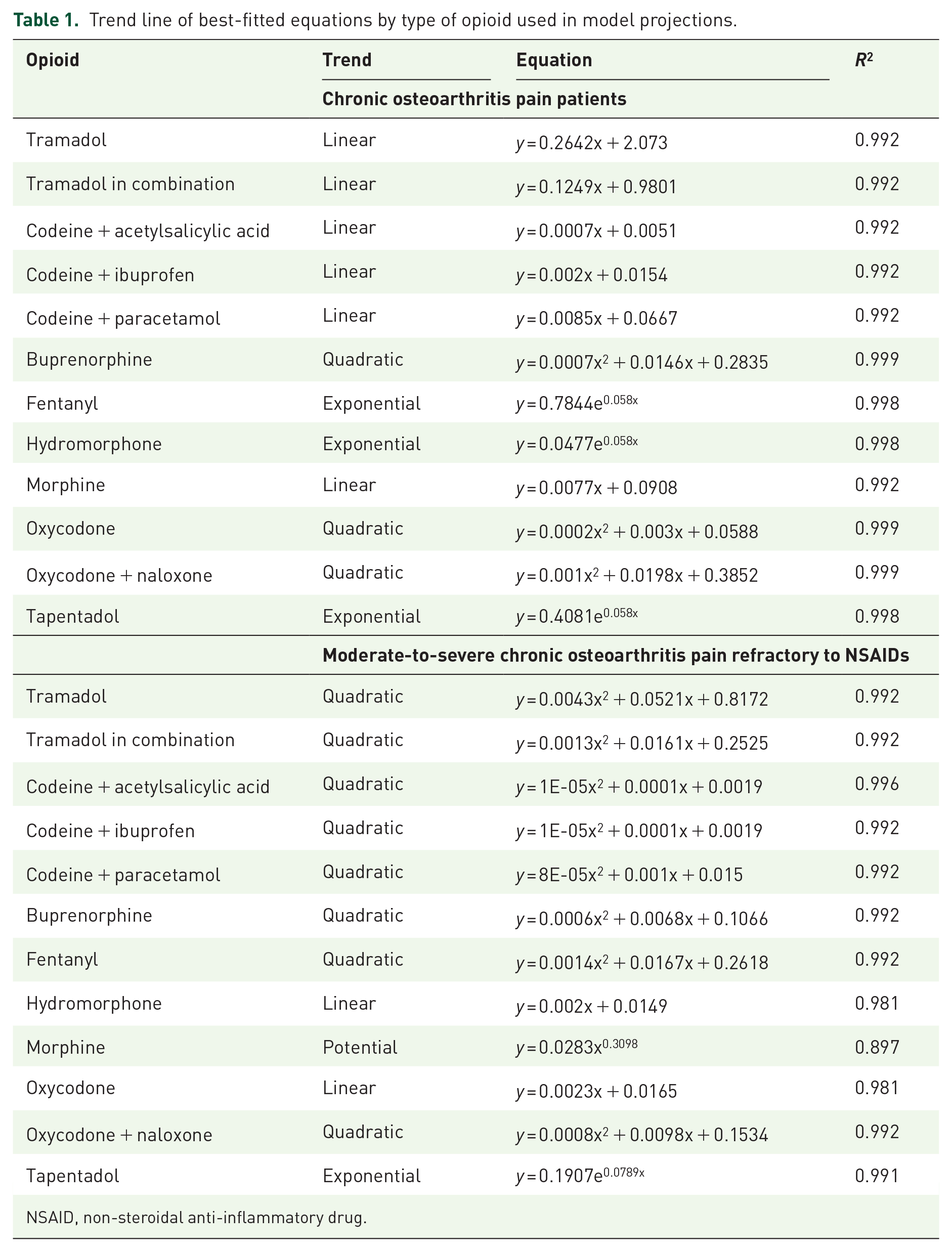
NSAID, non-steroidal anti-inflammatory drug.

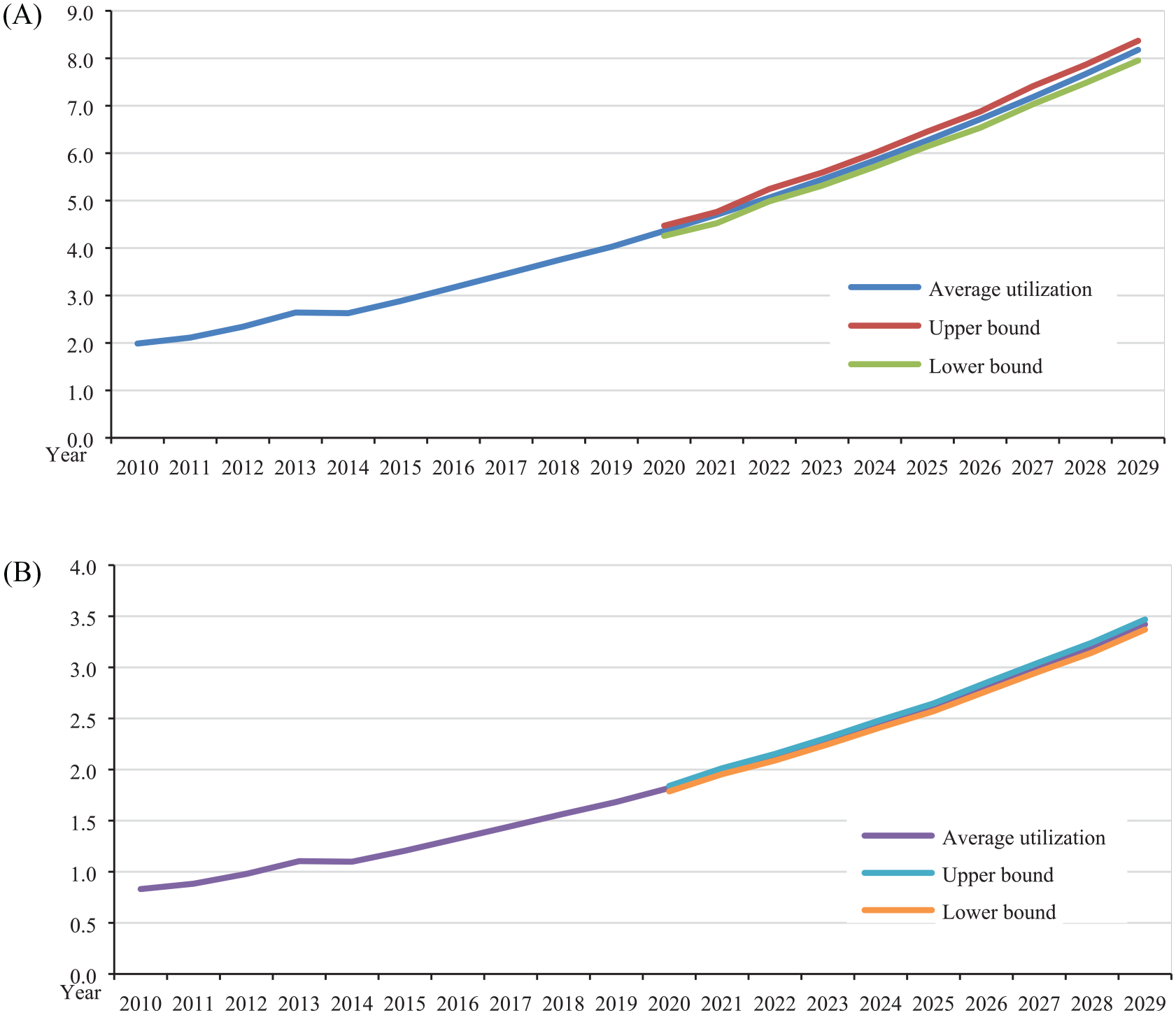
Annual DHD use of all opioids (A) and strong opioids (B) in Spain for the years 2010–2019 and projection years 2020–2029 in chronic osteoarthritis pain patients.
Sensitivity analysis
The uncertainty surrounding DHD projections in each year was managed by means of building a 95% probabilistic confidence interval of every annual DHD in the period 2020–2029. Probabilistic calculations were performed by means of a second order Monte Carlo simulation using the distribution utilization probability of each opioid drug for every projected year. Distribution probabilities in the model were allowed to be chosen at random each time for the 10,000 iterations carried out. The analyses ran 10,000 simulations for every year of the projections. Annual persons on opioid therapy and cost to the NHS were computed by multiplying the upper and lower bound of the 95% confidence interval by the estimated population in the year and the expected cost of each opioid DDD for future distribution use.
A sensitivity analysis was also undertaken to evaluate the potential variability around our opioid dispensing estimates given alternate scenarios. Alternative scenarios affecting the cost of opioids included using the ex-factory opioid price (Table S8, Supplemental material), 34 a maximum of 10% patient co-payment of the opioid PSP (this is because some opioids have a reduced patient co-payment), reducing the tapentadol price by either 40% or 60% of the base case as well, due to its expected loss of exclusivity during forthcoming years, including daily cost of concomitant non-narcotic analgesia as per the observed data in the OPIOIDS real-world study, using real-world opioid daily cost as observed in said OPIOIDS study,31,33 both at the public selling price and at the ex-factory price, and applying a 3% discount rate to the future cost, as per Spanish pharmacoeconomic guidelines. 37 The expected increase of OA prevalence in Spain due to an aging population was not included to avoid double counting, since future projections assumed that one of the reasons for the increment in opioid use could be due to incremental rates of OA prevalence. The sensitivity analysis also included subgroup analyses in OA patients. These included patients with chronic NSAID-refractory OA pain, 33 and both patients with chronic OA pain and those with pain which is refractory to NSAIDs and taking strong opioids only.
Confidentiality of information/ethical aspects
This study did not require an ethical board approval because the economic modelling included here used aggregate dated available in the public domain only, thus, no individual data from patients were obtained and, due to this, de-identification was guaranteed to prevent anyone’s personal identity from being revealed. Therefore, studies such as this one are exempt from Institutional Review Board review and from classification by the Spanish Agency of Medicines and Medical Devices according to current regulations for post-authorization observational studies (https://www.aemps.gob.es/investigacionClinica/medicamentos/estudiosPostautorizacion.htm#norEstatal).
Results
In 2010, an estimated 10.05 DHD of opioid prescriptions were dispensed in Spain for the equivalent of 384,764 pain patients/day, of which 5.67 DHD and 217,076 patients correspond to chronic OA pain patients (1.99 DHD and 76,084 refractory-to-NSAIDs; Tables 2 and 3, Figures 1 and 2 and Supplemental material Figure S1). These values increased by year 2019 to 10.82 DHD or the equivalent of 415,601 chronic OA pain patients/day (4.03 DHD and 154,710 refractory-to-NSAIDs). Strong opioid dispensing figures for the years 2010 and 2019 were, respectively, 84,225 and 141,134 for chronic OA patients (2.20 and 3.67 DHD) and 31,803 and 64,669 for patients with NSAID-refractory OA pain (0.83 and 1.68 DHD; Tables 2 and 3, Figures 1 and 2). Based on dispensing trends and OA prevalence, the projected number of dispensed opioid prescriptions is expected to more than triple to 17.98 DHD by 2029 (66.3% relative increment to 2019) or the equivalent of 727,356 chronic OA pain patients/day (8.18 DHD, 330,730 patients with chronic NSAID-refractory OA pain, 103.1% relative increment to 2019). For strong opioid utilization, the corresponding figures were 6.44 DHD by 2029 (75.2% relative increment) or the equivalent of 260,322 chronic OA pain patients/day (3.42 DHD, 138,353 patients refractory-to-NSAIDs, 103.3% relative increment).
Annual moderate-to-severe chronic osteoarthritis pain patients using a DDD per day of an opioid drug and cost to National Health System in Spain years 2010–2019 and projections years 2020–2029.
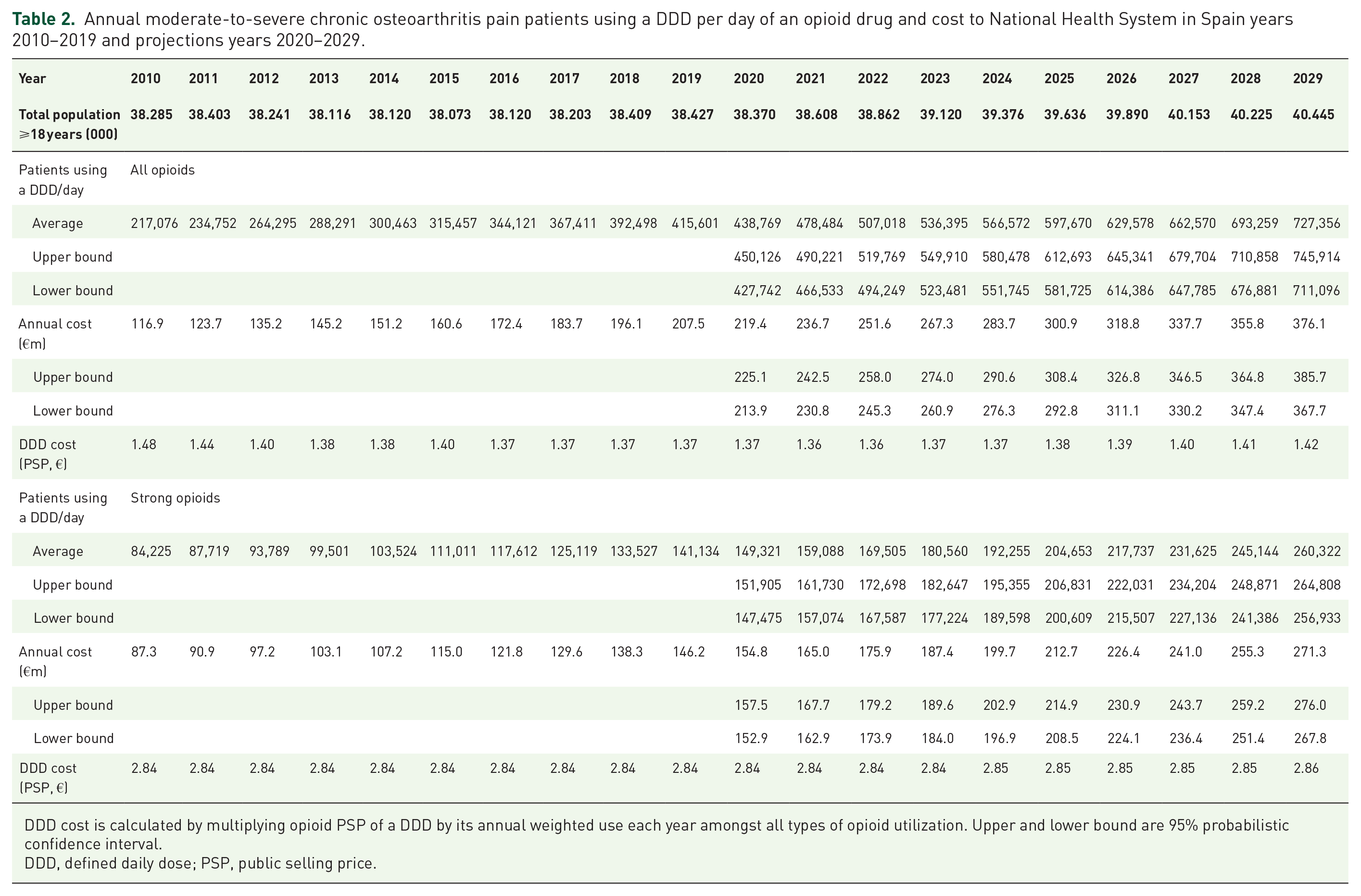
DDD cost is calculated by multiplying opioid PSP of a DDD by its annual weighted use each year amongst all types of opioid utilization. Upper and lower bound are 95% probabilistic confidence interval.
DDD, defined daily dose; PSP, public selling price.
Annual moderate-to-severe chronic osteoarthritis pain refractories to non-steroidal anti-inflammatory drugs using a DDD per day of an opioid drug and cost to National Health System in Spain years 2010–2019 and projections years 2020–2029.

DDD cost is calculated by multiplying opioid PSP of a DDD by its annual weighted use each year amongst all types of opioid utilization. Upper and lower bound are 95% probabilistic confidence interval.
DDD, defined daily dose; PSP, public selling price.
Annual DHD use of all opioids (A) and strong opioids (B) in Spain for the years 2010–2019 and projection years 2020–2029 in patients with moderate-to-severe chronic osteoarthritis pain which is refractory to non-steroidal anti-inflammatory drugs.
In accordance with the weighted opioid cost of a DDD in 2010 (€1.48 for chronic OA pain patients and €1.62 for refractory), the corresponding cost was €116.9m for chronic OA pain patients and €45.0m for patients with chronic NSAID-refractory OA pain (Tables 2 and 3). These values increased by ~76% and 98% to €207.5m and €91.5m, respectively, in 2019 despite the fact that the average DDD cost was decreased to €1.37 per day in chronic OA pain patients because of the incremental weight of tramadol and tramadol-in-combination in the mix of opioid use (Figures 3 and 4). Strong opioid dispensing costs for 2010 and 2019 were, respectively, €87.3m and €146.2m (~67% increase) for chronic OA patients (€2.84 per DDD) and €35.1m and €71.3m (~103% increase) for refractory-to-NSAIDs (€3.02 per DDD). Based on dispensing trends, the projected cost of opioids is expected to increase to €376.1 million (81.3% relative increment to 2019) in chronic OA pain patients (€1.42 per DDD), and to €199.7m (118.3% relative increment) for chronic NSAID-refractory OA pain by year 2029 (€1.65 per DDD). For strong opioid use, the corresponding figures were €271.3m (~86% increase related to 2019, €2.86 per DDD) for chronic OA pain patients and €156.6m (~120% increase, €3.10 per DDD) for NSAID-refractory patients (Tables 2 and 3).

Annual DHD use of weak (A) and strong (B) opioid-type individually in chronic osteoarthritis pain patients in Spain for the years 2010–2019 (solid line) and projection years 2020–2029 (dotted line).

Annual DHD use of weak (A) and strong (B) opioid type individually in patients with moderate-to-severe chronic osteoarthritis pain which is refractory to non-steroidal anti-inflammatory drugs in Spain for the years 2010–2019 (solid line) and projection years 2020–2029 (dotted line).
Probabilistic 95% confidence interval calculations were consistent with average estimations (Figures 1–4 and Tables 2 and 3). Under alternative projection scenarios for years 2020–2029 in the sensitivity analysis (Table 4), as expected, ex-factory price and 10% patient co-payment showed lower cost impact according to DDD cost reduction. The expected loss-of-exclusivity for tapentadol would cause a drop of from ~10% to 27% in the economic impact in opioid projections in 2029, both in DDD cost per day per patient and in total annual cost. However, including the cost of non-narcotic analgesia taken concomitantly with opioid drugs by chronic OA pain patients would show an increment of ~11% in the NHS drug expenditure for these analgesics: €415.9m in 2029 instead of €376.1m in the base case. This increment is more meaningful in the case of NSAID-refractory, chronic OA pain patients, who showed an increase in analgesia expenditure of approximately 28%: from €199.7m to €255.2m, always compared with year 2029. Findings in the analysis including strong opioids only showed results aligned with previous data (Table 4). On the other hand, including the real-word cost of a DDD as per the OPIOIDS study,31,33 future projections of economic impact will hit the NHS budget sharply by 2029, as compared with 2019, ranging from an increment of 81% to 119%, depending on the group and PSP, or ex-factory, prices taken into consideration (Table 4).
Sensitivity analysis: base case alternative scenarios.

DDD cost is calculated by multiplying opioid price of a DDD in each scenario by its annual weighted use each year amongst all types of opioid utilization. Range in parentheses: upper and lower bound 95% probabilistic confidence interval.
DDD, defined daily dose; LOE, loss-of-exclusivity; N/A, not applicable; NSAID, non-steroidal anti-inflammatory drug; OPIOIDS, Outcomes in Patients usIng Opioids In Painful Disorders in Spain; PSP, public selling price.
Discussion
This study is the first to provide estimates of the current burden of opioid use for OA-related pain in Spain, and to forecast the likely burden if opioid dispensing trends continue as shown by the drug utilization study conducted by the Spanish Medicinal Agency. 30 Our findings are like the ones found previously in other countries and in Australia most recently,25,27,28,38 which also showed a future growing trend in opioid dispensing in OA pain patients. The growing evolution observed in Spain consumed a significant portion of the NHS drug and healthcare expenditure in 2019: 1.01–1.88%. 39 Such figures would even triple or quadruple according to our forecast analysis of opioid utilization as assessed in terms of DHD (DDD/1000 patients per day) between 2010 and the projected 2029. A sizeable portion of the growing trend is caused by the current use and expected sharp increase in the use of tramadol and tramadol in combination: approximately 59% of total opioid dispensing. However, some strong opioids, particularly fentanyl, tapentadol and oxycodone plus naloxone, also showed robust increases, accounting for 27–30% of opioid use. Most of these prescriptions are signed by general practitioners or family medicine physicians in primary healthcare, as also reported previously.11,31,40 The economic implications of opioid use for OA warrant exploration, given the relatively high prevalence of this health condition and its expected growth due to an aging population.1,3,15,16 We estimated that 217,076 patients with chronic OA pain would consume a DDD of an opioid in 2010 and this figure would increase to 415,601 in 2019, scaling up to 727,356 in the projected year 2029, due partly to the expected increase in OA prevalence,15,41 but mainly to the incremental trend in opioid use recorded between 2010 and 2019. 30 These data mean that almost 10% of OA patients with chronic pain in Spain would be receiving an opioid daily at a DDD,15,31 which means that by 2029 nearly one million moderate-to-severe chronic OA patients (982,914) could be on an opioid therapy for OA pain if we take into account that the medication possession ratio (days that the patients have medicine in their hands) found in the OPIOIDS study was, on average, 74% each year. 31 Consequently, this is expected to have a clear financial impact on the healthcare system. Despite limited evidence to support long-term use, given its expected modest effectiveness in relation to OA pain, 42 anticipating using other analgesia concomitantly, the economic impact would be further increased due to the clinical consequences in the health of OA patients because of the potential collateral effects of opioid drugs. In the OPIOIDS study, after 3 years of follow-up and with a median duration of treatment with opioids of 203 days (interquartile range, 89–696), 3.3% more OA patients developed a cognitive deficit (as assessed with the MiniMental State Examination test) and 15.6% developed moderate-to-total dependence for basic activities of daily living according to the Barthel index, 31 both requiring costly specialized healthcare (residential nursing home care, carers, etc.). Other side-effects related to opioid use could add even more burden to the NHS.43,44 Particularly worrisome is the excess mortality associated with opioid use as described in the scientific literature,45–48 mainly with strong opioids, which has also been observed in Spanish OA patients receiving strong opioids in the OPIOIDS study.31,33
We used a real-world approach to project the future opioid burden for OA, based on recent opioid dispensing trends by the AEMPS, anticipated growth in the OA population and the opioid utilization rates observed in the real-world OPIOIDS study.30,31,33 By assuming no change in opioid prescribing practices, our study provides an important baseline for health decision makers and clinicians in Spain, in order to evaluate the potential impacts of future strategies that aim to address inappropriate opioid prescribing. We also performed a sensitivity analysis and an analysis in subgroups of patients with OA pain (NSAID-refractory and those taking strong opioids only), which showed that the growing trend in future opioid burden would remain unless international recommendations on opioid use are implemented, or newer therapeutic strategies based on drugs with a novel mechanism of action replace current drug-based analgesia of chronic OA pain.8,9 Nerve growth factor (NGF)-sequestering antibodies have exhibited the most promise in clinical trials, and they have shown potential to replace opioids and NSAIDs, which dominate the clinical landscape despite limited effectiveness and considerable side-effect profiles.49–53 Our findings in dispensing data show that, while the overall use (both in chronic OA pain patients and in NSAID-refractory patients) of some opioid subtypes is decreasing over time (for example, codeine/paracetamol and oral morphine preparations), the use of other opioid subtypes is increasing, and this is not only for weak opioids but also strong opioids such as tapentadol, fentanyl or oxycodone plus naloxone. There are clinical circumstances in which opioid use may be considered appropriate for patients with severe pain, such as when simple analgesics and/or anti-inflammatory medications are no longer effective, nor tolerated or inadequate, or while waiting for joint replacement surgery. 54 However, from a public health perspective, valid concerns have been raised about escalating opioid addiction and overdose issues and these harms undoubtedly contribute to the societal burden of opioid use. Notably, one should consider the high cost of treating chronic OA pain with strong opioids under real-world conditions of use, as shown in the OPIOIDS study.31,33 When included in our future projections, the financial impact in the 2029 NHS drug expenditure would grow between 118% and 344% relative to 2019 and 2010, respectively, as per the results of our sensitivity analysis. Our findings are not only aligned with recent Australian findings, 28 but also with data from the US study using Medicare claims, which revealed that tramadol use doubled from 5% of patients with knee OA in 2003 to 10% in 2009, and oxycodone prescriptions increased from 5% in 2003 to 8% in 2009. 25 Under alternative projection scenarios for the years 2020–2029 in the sensitivity analysis, as expected, ex-factory price and 10% patient co-payment showed lower cost impact according to DDD cost reduction. This information could nonetheless be of interest to some payors under certain circumstances of opioid reimbursement. Likewise, the expected loss-of-exclusivity for tapentadol would have an impact (of between 10% and 27%, depending on price reduction) on lowering the economic impact in opioid projections, both in DDD cost per day per patient and in total annual cost. However, including the cost of non-narcotic analgesia taken concomitantly with opioid drugs by chronic OA pain patients would show an increment of ~11% in NHS drug expenditure for these analgesics: €415.9m in year 2029 instead of €376.1m in the base case. This increment is more meaningful in the case of patients with NSAID-refractory chronic OA pain ,who showed an increase in analgesia expenditure of approximately 28%: from €199.7m to €255.2m, always compared with year 2029.
A key strength of our study is the use of national opioid use trends from the Spanish Medicinal Agency during a long period of time, comprising years 2010–2019, a large real-world opioid utilization study in patients with chronic pain, irrespective of prior analgesia used, and data from the most recent prevalence national study.15,30,31,33 Also, our results are in line with those already shown in other countries,25,27,28,38 thus supporting the plausibility of the findings presented in this research. Some novel elements include our subgroup analyses in patients with chronic NSAID-refractory OA pain or the strong opioid subgroup. Nonetheless, some limitations of our study should be raised. We restricted our modelling to opioids that are relevant to OA care (oral administration and patches) and did not include other forms that are largely limited to other clinical indications. Our projections are based on dispensed opioid prescriptions as these reflect the actual financial burden on the Spanish NHS only. For example, direct cost funded by the patients themselves or costs related to medication harm were not captured, nor was indirect cost due to lost labour productivity and, so, these costs could not be included in our analysis. On the other hand, our study did not include consumption by mutual funds, other insurers, hospital consumption, private prescriptions, or over-the-counter dispensing (basically self-medication), which could be interpreted as showing that our findings are, therefore, conservative. In this regard, there is expected to be a possible increment in opioid use of up to 20%, this year and in forthcoming years, due to the current impact of the COVID-19 pandemic on analgesia management and its related side-effects.55,56 Comparison of the results of this report with previous studies should be done with caution because the value of DDDs is not static and is subject to continuous review by the WHO Collaborating Centre for Statistics Methodology. These changes affect only some of the active substances. Similarly, the results are influenced by the population data chosen to perform the DHD calculations (pattern or census estimation). However, as mentioned above, our projections are in line with previous results shown in other countries. Finally, it should be noted that DDD is a technical unit of measurement and does not necessarily reflect the daily dose actually prescribed or used by the patient, although it should be an approximation of it. Discrepancies between DDD and the dose actually used by the population can cause the results expressed in DDD to overestimate or underestimate the actual use of the drug. In addition, the data handled do not reveal treatment compliance; dispensed units are expressed, but these may not be consumed by the patient. Therefore, the term ‘use’ (or ‘consumption’) is not used in a literal sense. This was the reason for running a sensitivity analysis using a daily cost of opioids, the ones observed in the real-world OPIOIDS study that, as far as we know, captured a more realistic picture of opioid use in real life, both considering its daily cost and patient adherence expressed in terms of percentage of days with medication possession. Finally, the potential costs of new opioids entering the market between 2020 and 2029 were not considered in these projections and we assumed that rates of opioid prescribing for OA would remain constant over time; nor was the possible commercialization of novel NGFs indicated in OA pain that could replace or diminish opioid use in the projected period of time. In general, as with any forecasting, the accuracy of estimating future outcomes based on currently available data (that is, projecting beyond the range of data used to build the model) is unknown. We recognize that many factors can influence these trends (impact of modifying prescribing practices as a consequence of new clinical practice and public health guidelines, more use of new analgesics or disease-modifying drugs, pricing considerations, current international debate around the use of opioids for chronic non-cancer pain, etc.).
In conclusion, and despite the possible limitations enumerated above, chronic OA-pain-related opioid dispensing and costs to the NHS are set to increase substantially (threefold to more than fourfold) from 2010 to 2029 in Spain. Thus, using opioids for OA pain is concerning given disease chronicity, aging population and other related costs not computed in these projections. Our findings can inform payors and clinicians about ongoing discussions on appropriate analgesic management for longer-term OA pain, including resource requirements at a national level. Clinicians who prescribe opioids for OA pain should consider the potential implications of side-effects such as sedation, cognitive deterioration and incremental need of caregivers, particularly in older people, and also carefully consider the risk–benefit balance.
Supplemental Material
sj-pdf-1-tab-10.1177_1759720X211010599 – Supplemental material for Future projections of opioid use and cost in patients with chronic osteoarthritis pain in Spain
Supplemental material, sj-pdf-1-tab-10.1177_1759720X211010599 for Future projections of opioid use and cost in patients with chronic osteoarthritis pain in Spain by Javier Rejas-Gutierrez, Antoni Sicras-Mainar and Josep Darbà in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
Preliminary findings were presented at the 2020 E-ISPOR annual meeting held on 14–18 November 2020 in Milan, Italy.
Author contributions
Each author agrees that the manuscript represents honest work. The data reported within the manuscript are not proprietary to any of the authors. Javier Rejas-Gutiérrez was responsible for the study concept and data analysis. Antoni Sicras-Mainar and Josep Darbà reviewed the analysis and participated in data interpretation. The manuscript was prepared jointly by all authors, and all of them had the right to review, comment on, and approve the manuscript prior to submission.
Availability of data and materials
All data generated or analysed during this investigation are included in this published article. Any additional information is available from the corresponding author upon reasonable request.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.