
Abstract
Background:
The aim of this study was to assess the real-world effectiveness and safety of certolizumab pegol (CZP) in rheumatoid arthritis (RA) patients, and the impact on patients’ productivity, pain, and fatigue, in Canadian practice.
Methods:
FαsT-CAN, a 2-year prospective, observational study, evaluated CZP use in Canadian adults with moderate to severe, active RA. The primary objective was to assess the proportion of patients achieving 28-joint Disease Activity Scores (DAS28) <2.6 at Week 104. Secondary and additional endpoints assessed the improvements in Patients’ Assessment of Arthritis Pain (PtAAP), fatigue, Health Assessment Questionnaire-Disability Index (HAQ-DI), and the proportion of patients achieving minimal clinically important differences (MCID) in HAQ-DI. Validated arthritis-specific Work Productivity Surveys (WPS-RA) assessed the RA-associated impact on productivity. Incidence of CZP-related treatment-emergent adverse events (TEAEs) was reported for patients receiving ⩾1 dose of CZP (safety set).
Results:
The full analysis set (baseline DAS28 ⩾ 2.6, ⩾1 dose of CZP and ⩾1 valid post-baseline DAS28 measurement) included 451 of the 546 patients recruited into the study; a total of 229/451 (50.8%) patients completed Week 104. At Week 104, 90/451 (20.0%) patients achieved DAS28 < 2.6. Rapid improvements in disease activity, pain, and fatigue were observed. At Week 104, 66.2% of patients achieved HAQ-DI MCID. Patients employed at Week 104, reported reduced absenteeism, and improved productivity. CZP-related TEAEs were consistent with the known CZP safety profile.
Conclusions:
CZP was an effective RA treatment in Canadian practice, and no new CZP-related safety signals were identified. The improvements in household and workplace productivity are the first observations in a real-world Canadian setting.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by systemic inflammation and persistent synovitis, which causes pain, stiffness and swelling of joints leading to loss of physical function, work disability, and decreased quality of life.1,2
Certolizumab pegol (CZP) is an Fc-free, PEGylated anti-tumor necrosis factor (TNF) treatment, approved worldwide for several chronic inflammatory diseases. For RA, CZP is indicated in Canada for patients with moderate to severe, active disease, who do not respond adequately to methotrexate (MTX). 3 The Canadian Rheumatology Association guidelines indicate that patients should be considered for biologic disease modifying anti-rheumatic drugs (bDMARDs) if moderate to high disease activity [i.e. 28-joint disease activity score (DAS28) > 3.2] persists after 3 months, despite treatment with at least two prior synthetic DMARDs (sDMARDs), such as MTX. 4
Randomized clinical trials (RCTs), including the pivotal RAPID-1 (ClinicalTrials.gov identifier: NCT00152386) and RAPID-2 (ClinicalTrials.gov identifier: NCT00175877) studies, have demonstrated a fast, clinical response in CZP-treated RA patients.5,6 However, while RCTs provide important results regarding the efficacy and tolerability of a drug, the selective nature of their design and subsequent under-representation of particular patient demographics may not reflect clinical practice. 7
Several publications have reported on real-world effectiveness and safety of the first anti-TNFs approved for RA. The most recently approved anti-TNFs are under-represented in the current literature; however, the inclusion of data from patients treated with these anti-TNFs within registry reports is increasing.8–10 For this reason, real-world evidence studies evaluating the effectiveness of CZP are needed. 11 Real-world, observational studies are particularly useful as they provide data on treatment tolerability and safety in large heterogeneous populations, and show how the clinical setting influences treatment outcomes, and thus complement the data provided in RCTs. 12
Here, we report the largest sample of real-world effectiveness and safety data of CZP treatment, to our knowledge, in patients with RA in a Canadian practice setting from the observational FαsT-CAN trial. This study is also the first to report real-world workplace and household productivity in Canadian patients with RA.
Methods
Patients
Patients aged ⩾18 years with moderate to severe, active RA were enrolled into the study. All patients provided written, informed consent prior to their participation in the study. The decision to initiate CZP treatment was made by the physician prior to their patient’s enrolment into the study; all patients were prescribed CZP in line with the Canadian CZP product monograph, during routine clinical practice. 3 Prior biologic use was permitted and enrolled patients could take non-biologic DMARDs concomitantly during the study; all RA medications were prescribed at the discretion of the treating physician.
Any patients who had previously been treated with CZP, or had a known hypersensitivity to CZP, or any of its components, were not permitted to take part in the study. Patients with active tuberculosis or other severe infections such as sepsis, abscesses and opportunistic infections were not eligible for inclusion.
Study design
FαsT-CAN was a prospective, observational, multi-center study conducted between 22 December 2010 and 6 December 2016 at a total of 48 sites in Canada. Patients were observed for a duration of 104 weeks, with an additional 10-week safety follow-up if patients did not prematurely discontinue CZP treatment. No investigational products were used in this study; CZP was provided only upon prescription by the patient’s physician. All patient clinical procedures, assessments and decisions were undertaken as decided by the physician in the framework of current standard clinical practice and as directed in the Canadian Cimzia™ Product Monograph. In accordance with the Canadian product monograph for CZP, a loading dose of 400 mg CZP by subcutaneous injection was given at Weeks 0, 2 and 4, followed by a maintenance dose of 200 mg CZP every 2 weeks or 400 mg CZP every 4 weeks. The full analysis set (FAS) consisted of all patients who received ⩾1 dose of CZP, with a baseline DAS28 value and ⩾1 valid post-baseline DAS28 values. The safety set (SS) included all patients who received ⩾1 dose of CZP.
The study was performed in full compliance with the Declaration of Helsinki and was approved by the local or central ethics committees.
Study procedures and evaluations
The primary objective of this study was to assess the clinical effectiveness of CZP in achieving a DAS28 < 2.6 after 2 and years of therapy in adult patients with RA. DAS28 was preferentially assessed using C-reactive protein (CRP); however, if CRP measurements were unavailable erythrocyte sedimentation rate (ESR) was used, providing that the assessment was consistent for that patient for the duration of the study. Post-hoc analyses determined the proportions of patients achieving DAS28(ESR) < 2.6 and ⩽3.2 (i.e. disease remission, and low disease activity) and DAS28(CRP) < 2.6 and ⩽3.2.
The procedures carried out during the study were in accordance with current clinical practice for RA; data were collected during physician visits which corresponded most closely to the study schedule of Weeks 0, 12, 20/24, 76, 104, and 114 (for patients included in the safety follow-up).
Additional study outcomes
Disease activity was measured using the Clinical Disease Activity Index (CDAI) at each study visit. The joint assessment was carried out on 28 joints; if joints were missing or not assessable, the number of joints was weighted by the actual number of evaluated joints.
The Health Assessment Questionnaire-Disability Index (HAQ-DI) was measured at Week 104. The proportion of patients achieving the minimal clinically important differences (MCIDs) in HAQ-DI, defined as a decrease of ⩾0.22 points from baseline, was assessed post-hoc and reported to Week 104.13,14 Patients reported the duration of morning stiffness, in minutes, which was defined as the time elapsed between the patient waking and being as limber as would be normal for the patient during a typical day. Patients rated the impact of RA on their fatigue during the past week on the validated Canadian versions of the Fatigue Assessment Scale (0–10 scale), at all timepoints to Week 104. Change from baseline in patients’ assessment of arthritis pain (PtAAP) was measured using a visual analogue scale [VAS; 0 (no symptoms), 100 (severe symptoms)]. Patients scored the level of pain caused by arthritis at the time of the visit, using the validated Canadian versions of the questionnaire.
The validated arthritis-specific work productivity survey (WPS-RA) was used to assess the impact of RA on productivity within the household and the workplace, and is reported to Week 104. 15 The number of days of work missed (absenteeism), the number of days with productivity reduced by ⩾50% (presenteeism), and the level of arthritis interference with productivity (0–10 scale; 0 = no interference and 10 = complete interference) were recorded.
Safety analyses
Safety data report treatment-emergent adverse events (TEAEs), including serious adverse events (SAEs), assessed as related to CZP, and adverse events of special interest (serious infections, malignancies, serious hemorrhage and serious skin reactions) irrespective of their relationship to CZP. Other TEAEs (including SAEs), assessed as not related to CZP were also recorded when reported, although their collection was not foreseen in the study protocol or performed systematically, so should be interpreted with caution.
Statistical analyses
Statistical differences in DAS28 were calculated between baseline and Week 12, 20/24, 52, and 104. Student’s t-tests were performed Post-hoc; the resulting p values are nominal and should therefore be interpreted in an exploratory nature. The p values have not been provided for secondary outcomes because it would be inappropriate to infer differences when the values would be associated with bias due to an increased level of type I error. The FAS, defined as all patients with a baseline DAS28 ⩾ 2.6, who took ⩾1 dose of CZP and provided ⩾1 valid post-baseline DAS28 measurement, was used for all clinical effectiveness measurements.
Safety analyses were performed on the SS, which included all patients having taken ⩾1 dose of CZP. All TEAEs were classified according to the Medical Dictionary for Regulatory Activities version 19.0. Incidence of TEAEs were reported as the number of first occurrences of an event per 100 patient-years of exposure. The exposure-adjusted event rate (EAER) was reported per 100 patient-years to account for the mean total duration of CZP, and was calculated as:

Missing binary values were imputed using non-responder imputation (NRI), while missing continuous values were not imputed. Patients who did not complete the 104 weeks were considered to be non-responder.
Results
Patient disposition and baseline characteristics
A total of 546 patients were enrolled into the study, of which 229/546 (41.9%) completed to Week 104 (Supplementary Figure S1). The reasons provided by the treating physician for discontinuation included adverse events (n = 73), lack of efficacy (n = 177), lost to follow-up (n = 28), protocol deviation (n = 1), consent withdrawn (n = 14), and other (n = 22). The majority of patients within the SS were female [424/546 (77.7%)] and the mean age [standard deviation (SD)] was 55.8 (12.5) years (Table 1). Of the patients enrolled into the study, 373/546 (68.3%) patients had an RA disease duration of 2 years or more (Table 1). A total of 210/546 (38.5%) patients had prior experience of another anti-TNF or other biologic medication, prior to starting CZP. A greater proportion of patients with prior anti-TNF experience had RA disease duration ⩾2 years [190/209 (90.9%)] compared with anti-TNF-naïve patients [183/337 (54.3%)]. All other baseline demographics and measures of disease activity were similar between patients with and without prior anti-TNF use (Supplementary Table S1).
Baseline patient demographics and disease characteristics.

Full analysis set. ªSafety set [all patients having taken ⩾1 dose of CZP (n = 546)]. bPrior anti-TNFs and biologics refer to treatments with a start date prior to the date of the first dose of CZP. cMedications were considered to be concomitant when the start date was prior to the date of the last administration of CZP plus 14 or 28 days (depending upon the regimen), and when the stop date was on or after the date of the first administration of CZP, or missing.
ACPA, anti-citrullinated protein antibody; CDAI, clinical disease activity index; CRP, C-reactive protein; DAS28, 28-joint disease activity score based on either CRP or ESR; DAS28(CRP) based on CRP; DAS28(ESR) based on ESR; ESR, erythrocyte sedimentation rate; FAS, full analysis set; HAQ-DI, Health Assessment Questionnaire-Disability Index; PhGADA, physician’s global assessment of disease activity; PtAAP-VAS, patient’s assessment of arthritis pain-visual analogue scale; PtGADA, patient’s global assessment of disease activity; RF, rheumatoid factor; SD, standard deviation; SJC, 28-count swollen joint count; TJC, 28-count tender joint count; TNF, tumor necrosis factor; VAS, visual analogue scale.
Disease activity
At Week 104, 90/451 (20.0%) patients achieved the primary objective of DAS28 < 2.6. The proportion of patients achieving DAS28 < 2.6 was sustained from Week 12 through Week 104, when data were imputed using the NRI [Figure 1(a)]. Similar proportions of patients achieved DAS28 < 2.6 at Week 104, whether they had <2 year RA duration [31/142 (21.8%)] or ⩾2 years RA duration [59/309 (19.1%)].
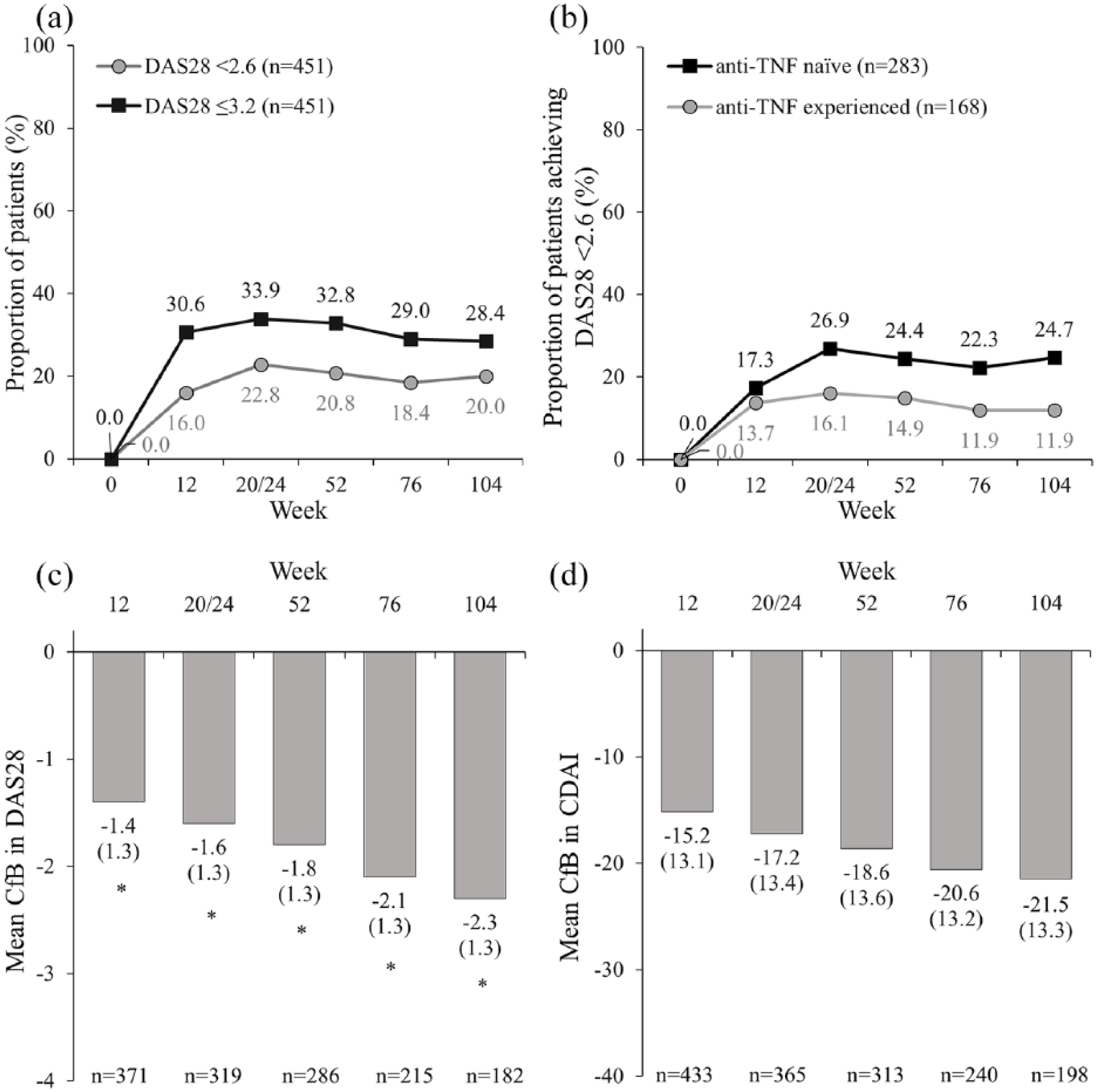
(a) Proportion of patients achieving DAS28 < 2.6 and ⩽3.2 (NRI), (b) proportion of patients achieving DAS28 < 2.6 in patients by prior anti-TNF use (NRI) and, (c) mean change from baseline in DAS28 (NRI), and (d) mean change from baseline in CDAI (observed).
A greater proportion of anti-TNF-naïve patients achieved DAS28 < 2.6 at Week 104 [70/283 (24.7%)] compared with anti-TNF-experienced patients [20/168 (11.9%); Figure 1(b)]. The proportion of anti-TNF-naïve patients achieving DAS28 < 2.6 increased up to Week 20/24, this proportion of patients was sustained through Week 104 [Figure 1(b)]. DAS28 ⩽ 3.2 was achieved by 128/451 (28.4%) at Week 104, and the proportion of patients achieving DAS28 ⩽ 3.2 was sustained over time [Figure 1(a)]. The mean change (SD) from baseline in DAS28 score (calculated using CRP preferentially, but ESR was used if CRP was unavailable) was −1.6 (1.3) at Week 20/24 and −2.3 (1.3) at Week 104 [Figure 1(c); both p < 0.0001]. Similar trends were observed when assessing low disease activity and remission rates using DAS28(CRP) and DAS28(ESR), as shown in Supplementary Figure S2(a–d). CDAI decreased at each visit, with a mean reduction (SD) from baseline of −21.45 (13.25) at Week 104 [Figure 1(d)].
Patient-reported outcomes
Patients’ physical function, measured by the Canadian validated versions of HAQ-DI, improved over time; by Week 104 the mean change (SD) from baseline was −0.52 [0.68; Figure 2(a)]. The proportion of patients achieving MCID in HAQ-DI increased from Week 12 to Week 104 [Figure 2(b)]. Mean duration (SD) of morning stiffness decreased from 142.5 (251.5) minutes at baseline to 62.7 (225.8) minutes at Week 104 [Figure 2(c)]. Mean patient-reported fatigue (SD) decreased from 6.60 (2.2) at baseline to 4.20 (2.7) at Week 104 [Figure 2(d)]. Patients’ arthritis pain, assessed by PtAAP, decreased at each visit with a mean change (SD) from baseline of −27.1 (30.3) at Week 104 [Supplementary Figure S3(a–b)].
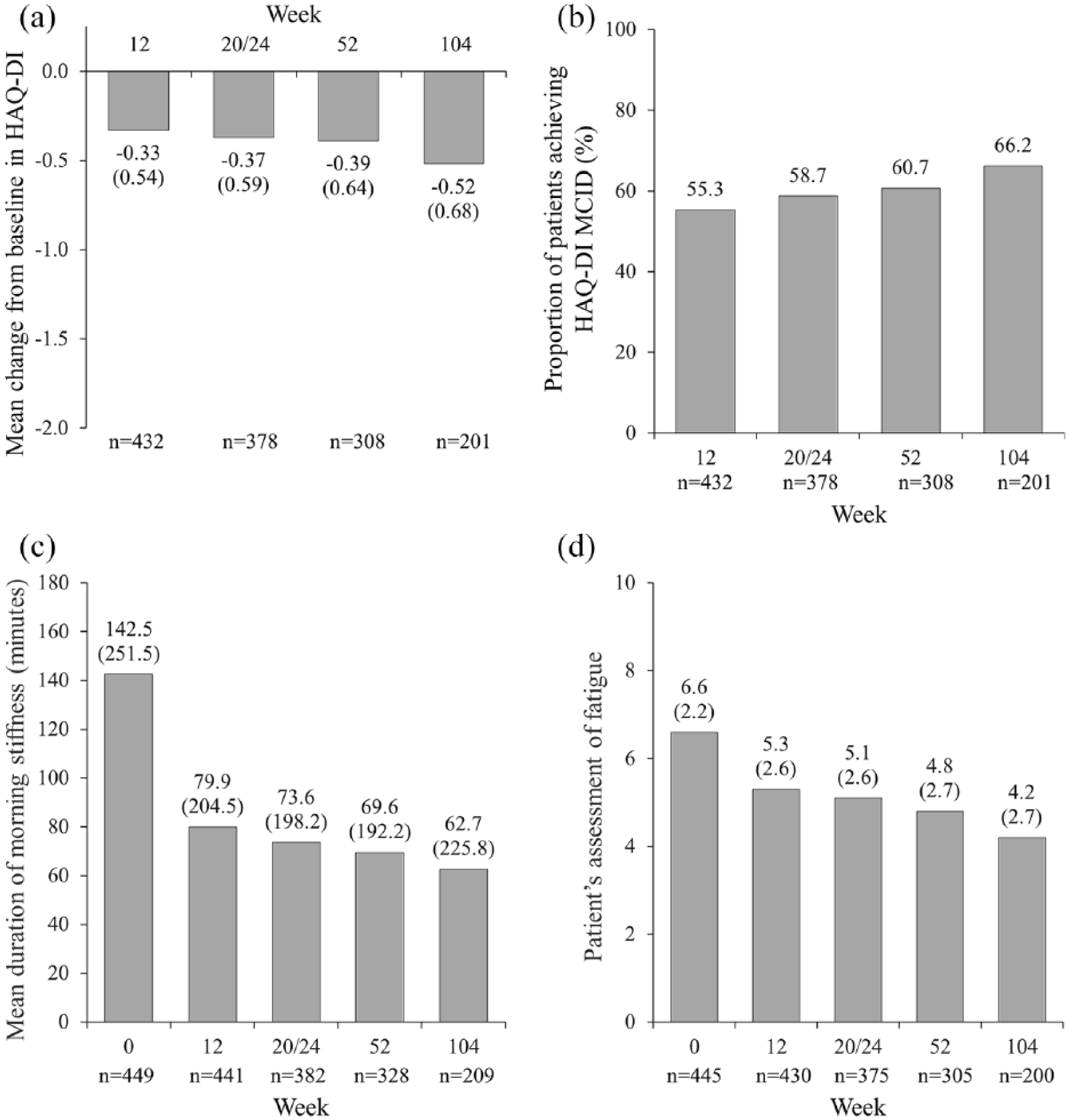
(a) Change from baseline in HAQ-DI, (b) proportion of patients achieving HAQ-DI MCID, (c) mean duration of morning stiffness, and (d) patient-reported fatigue assessments.
Household and workplace productivity
At baseline, 187 (41.7%) patients were employed, of whom the majority had a non-manual job. All measures of household and workplace productivity improved at Week 104, despite a high burden of RA on workplace and household productivity at baseline (Figure 3).
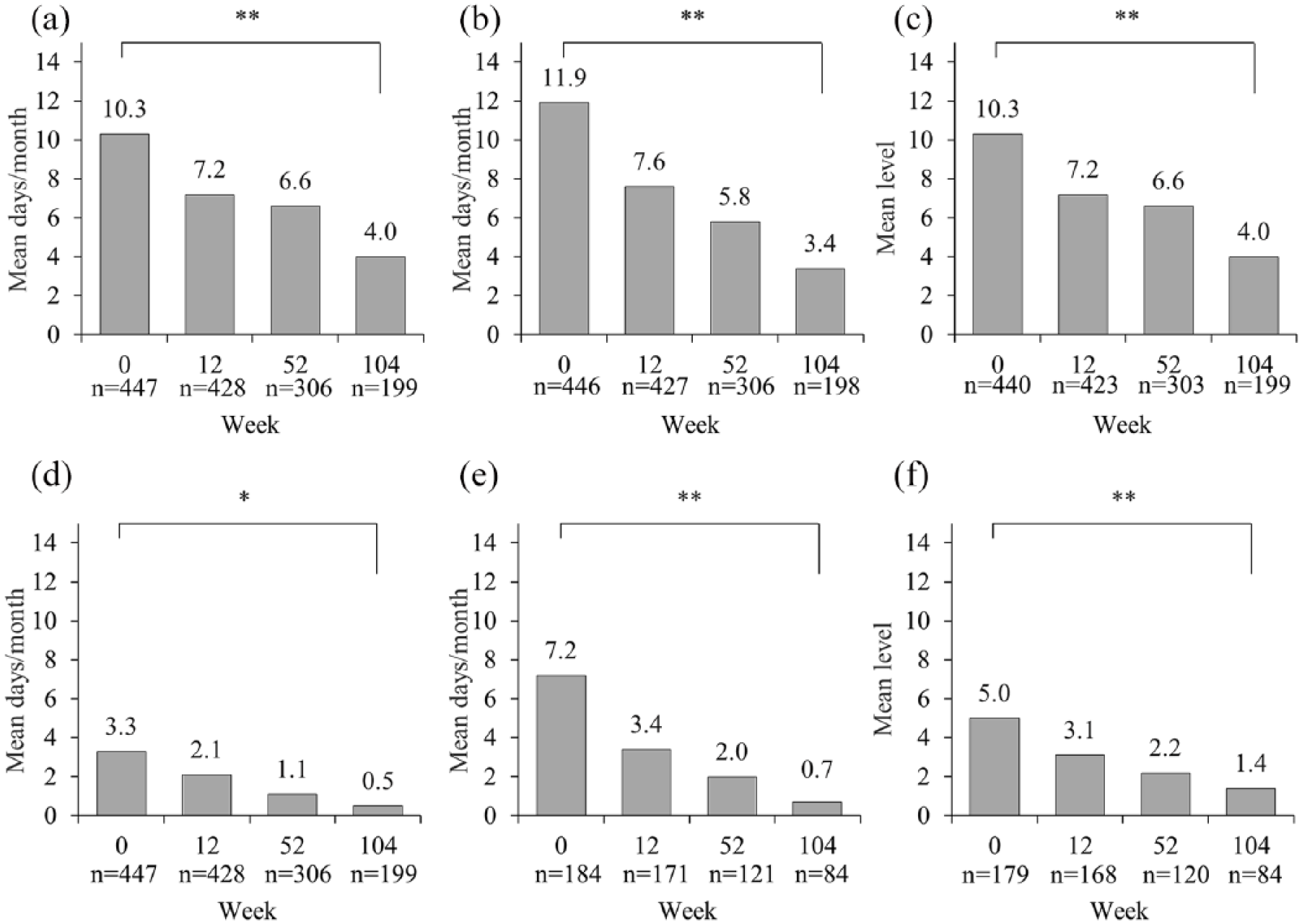
Work productivity survey results. (a) Number of household days missed due to arthritis/month. (b) Number of days with household productivity reduced by ⩾50%/montha. (c) Level of arthritis interference with household work productivity/monthb. (d) Number of paid work days missed due to arthritis/month (absenteeism)a. (e) Number of days with paid work productivity reduced by ⩾50%/month (presenteeism)a, c. (f) Level of arthritis interference with paid work productivity/monthb.
Safety
The mean duration (SD) of exposure to CZP was 482.0 (292.6) days, with a total exposure of 800.6 patient-years. A total of 279 patients reported 706 TEAEs during the study, of which 162 patients reported 281 TEAEs which were considered as related to CZP treatment (Table 2). The most commonly reported TEAE (occurring in ⩾5% of patients) by MedDRA preferred term was upper respiratory tract infection (Table 2). Severe TEAEs were reported in 35 (6.4%) patients, of which the most commonly reported severe TEAEs [12 (2.2%) patients] were classified within the MedDRA system organ class ‘Infections and Infestations’. A total of 74 (13.6%) patients experienced TEAEs which led to discontinuation of CZP. The most common related TEAEs leading to discontinuation by MedDRA preferred term (occurring in ⩾0.5% patients) were headache (seven patients), psoriasis (seven patients), rash (four patients), and nausea (three patients). The most common drug-related TEAEs by MedDRA preferred term (occurring in ⩾2% of patients) were upper respiratory tract infection (14 patients), sinusitis (13 patients) and rash (11 patients), shown in Table 2.
TEAEs for all patients enrolled into the prospective, observational study.

Safety set. EAER is given per 100 patient-years. Incidence rate is given per 100 patient-years.
number of individual occurrences of the TEAE. Collection of TEAEs (including SAEs) judged by a physician as unrelated to CZP, was not foreseen in the study protocol or performed systematically, so the summary should be interpreted with caution. aActual total is 75 (one patient had a fatal AE with no further information available and was not included in this table as the event was not recorded in the patient’s AE case report form as leading to discontinuation or ‘drug withdrawn’). bOverall, five deaths were reported during the study, however due to the lack of information available for the fatal adverse event experienced by one patient, the reason for discontinuation was recorded as an ‘adverse event’, instead of a death.
AE, adverse event; CI, confidence interval; CZP, certolizumab pegol; EAER, exposure-adjusted event rate; IR, incidence rate; NR, not reported; SAE, serious adverse event; TEAE, treatment-emergent adverse event. MedDRA Version 19.0.
A total of 76 SAEs were reported during the study. SAEs, which were considered to be related to CZP, were reported by 20 (3.7%) patients. A total of 24 serious treatment-emergent infections were reported by 14 (2.6%) patients, the most commonly reported serious infections by preferred term (occurring in ⩾0.4% of patients) were pneumonia [5 (0.9%) patients] and sepsis [3 (0.5%) patients]. Of these, 14 serious infections, reported by 10 patients, were considered to be related to CZP treatment by the patient’s physician. No cases of tuberculosis were observed during the study.
Malignancies were reported in nine (1.6%) patients and included one case each of lymphoma, lung cancer, throat cancer, invasive ductal breast carcinoma, Hodgkin’s lymphoma, chronic lymphocytic leukemia, squamous cell carcinoma, and two cases of basal cell carcinoma. The case of lymphoma was considered by the patient’s physician to be related to CZP, while the remaining eight reported malignancies were not considered to be related to CZP by the patients’ physicians.
Overall, five deaths were reported during the study, four of which were considered not to be related to treatment with CZP. A total of three cases with fatal TEAEs were assessed as not related to CZP and the causes of death were reported as severe malignant lung neoplasm, severe throat cancer, and severe intracranial aneurysm. The causes of death for the remaining two patients were unknown.
Discussion
This is the first study to report real-world effectiveness and safety data of CZP in Canadian patients with RA. Overall, CZP was effective in the treatment of patients with RA, particularly with improvements in both work absenteeism and presenteeism, and no new safety signals were identified. A fifth of all patients achieved the primary objective of DAS28 < 2.6 at Week 104, and rapid improvements were observed in all additional study outcomes, when data were imputed using NRI. The proportion of patients achieving DAS28 < 2.6, or DAS28 < 3.2 increased from Week 12, and this proportion of patients was sustained to Week 104. Patient-reported improvements in pain and fatigue were observed from Week 12 and mean scores were sustained through Week 104. Improvements in all parameters of productivity within the household and the workplace, as assessed by the WPS-RA, were observed from Week 12 and the mean responses were sustained to Week 104. Overall, these observations are in line with the PREDICT, RAPID-1 and RAPID-2 studies which show that CZP treatment in patients with RA, for 24, 52 or 256 weeks, resulted in improved disease activity measured by DAS28(ESR), physical function by HAQ-DI, patient-reported fatigue, pain, and attendance and productivity in the workplace and household.5,6,16
The proportion of patients in the FAS who completed the study to Week 104 was 42%, which is similar to the retention rate (36.2%) observed in the German FαST non-interventional study at Week 52. 17 While, the PROACTIVE non-interventional study in the United Kingdom and Ireland had a higher retention rate, with 68.5% of patients completing the study to Week 88. 18 Within the present study, it was observed that similar proportions of patients achieved DAS28 < 2.6 at Week 104, whether they had <2 years or ⩾2 years RA duration. Greater improvements in disease activity (DAS28) were observed in anti-TNF-naïve patients, when compared to patients with prior anti-TNF experience. In this study, >15% of patients had prior experience with ⩾2 anti-TNFs or other biologic agents. Prior experience with anti-TNFs is associated with lower response rates; the greater the number of anti-TNFs previously used, the lower the associated response.19,20 Patients with moderate to high disease activity, who had only taken one prior anti-TNF, were more likely to achieve remission than patients with ⩾2 prior anti-TNF treatments. 20 Similarly, in the EXXELERATE trial, patients with one prior anti-TNF, showed a better DAS28(ESR) response as >50% of patients went on to achieve low disease activity [DAS28(ESR) ⩽ 3.2] from Week 12, compared to patients with >1 prior anti-TNF. 21 However, the REALISTIC study showed similar improvements in DAS28(CRP) and ACR20, 50 and 70 responses when patients were stratified by prior anti-TNF use; although a numerical trend for higher response rates was observed in anti-TNF-naïve patients. 22 Similarly, the results from the South Swedish Arthritis Treatment Group Register showed that first-time anti-TNF switchers had similar response rates to anti-TNF-naïve patients. 23
Patient-reported outcomes showed CZP treatment improved symptoms such as fatigue and arthritis associated pain through Week 104. These findings are consistent with short-term 12-week RCT data and longer-term data from the Corrona registry which showed that patients experienced improvements in pain and fatigue after anti-TNF treatment initiation.14,24,25 These improvements were associated with better disease control, based on CDAI. 24
The improvements observed in household and workplace productivity are the first to be reported in a real-world Canadian setting and are consistent with RCTs where improvements in workplace and household productivity were maintained for the duration of the study.14,16 Similarly, clinically meaningful reductions in the rate of RA interference with workplace productivity have been observed in patients achieving HAQ-DI MCID. 14 We also report reductions in patient-reported pain and fatigue over 104 weeks, which are in line with observations from the RAPID-1 and REALISTIC trials.26,27 Observational data from the British Society of Rheumatology (BSR) Biologics Register also showed improvements in fatigue in patients treated with anti-TNFs (infliximab, etanercept and adalimumab); however, a different measure of fatigue was used than that in the present study. 28 Improvements in morning stiffness have previously been observed in patients treated with adalimumab (from the Corrona registry) and etanercept or infliximab compared with patients not receiving anti-TNF treatment, which complement the findings of the present study.29,30
No new safety signals were identified and the incidence of CZP-related TEAEs were in line with the known safety profile of CZP.5,6
The limitations of the study included the use of DAS28(CRP) as the preferred measure for the primary outcome as this was not validated in the most recent European League Against Rheumatism (EULAR) recommendations for the management of RA. 31 However, a comparison study showed that DAS28(CRP) and DAS28(ESR) were both useful measures for assessing disease activity in patients with RA, 32 and the post-hoc analyses performed in this study indicated very similar results. Another limitation of the study was the observational design, which can result in inherent selection bias as the patients were not randomized into treatment and control groups, as in an RCT. This can result in the over-estimation of treatment effects due to the lack of a control group. 33 Another limitation of the present study was that a high proportion of patients did not remain in the study to Week 104, and thus did not provide data for the primary endpoint of the study. Data were therefore imputed by NRI for the primary outcome; however, patients usually respond to CZP by Week 12 [DAS28(ESR)], after which their response is maintained, 34 these patients were likely to be those who did not respond to CZP.
Conclusion
Overall, the FαsT-CAN study demonstrated a long-term benefit of CZP treatment in patients with moderate to severe RA, in a Canadian practice setting. This is the first study to report patient-reported improvements in workplace and household productivity after 2 years of CZP treatment in a real-world Canadian practice setting, and these results are consistent with the results of previously published RCTs. 35 Similarly, rapid and sustained improvements in disease activity and patient-reported improvements in pain and fatigue were demonstrated.
Supplemental Material
Supplementary_Section_30Oct2018 – Supplemental material for Effectiveness and safety of certolizumab pegol in rheumatoid arthritis patients in Canadian practice: 2-year results from the observational FαsT-CAN study
Supplemental material, Supplementary_Section_30Oct2018 for Effectiveness and safety of certolizumab pegol in rheumatoid arthritis patients in Canadian practice: 2-year results from the observational FαsT-CAN study by Louis Bessette, Boulos Haraoui, Andrew Chow, Isabelle Fortin, Sanjay Dixit, Majed Khraishi, Derek Haaland, Sami Elmoufti, Fabienne Staelens, Irina Bogatyreva, Jerry Syrotuik and Saeed Shaikh in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors thank the patients, the investigators and their teams who took part in this study. The authors also acknowledge Simone E. Auteri, MSc, EMS from UCB Pharma, Brussels, Belgium, for publication coordination and Sarah Jayne Clements, PhD and Simon Foulcer, PhD from Costello Medical, Cambridge, UK, for medical writing and editorial assistance in preparing this manuscript for publication, based on the authors’ input and direction.
The author contributions were as follows: Substantial contributions to study conception and design: LB, BH, AC, IF, SD, MK, DH, SE, FS, IB, JS, SS; Substantial contributions to acquisitions of data: LB, BH, AC, IF, SD, MK, DH, SE, FS, IB, JS, SS; Substantial contributions to analysis and interpretation of data: LB, BH, AC, IF, SD, MK, DH, SE, FS, IB, JS, SS; Drafting the article or revising it critically for important intellectual content: LB, BH, AC, IF, SD, MK, DH, SE, FS, IB, JS, SS; Final approval of the article to be published: LB, BH, AC, IF, SD, MK, DH, SE, FS, IB, JS, SS
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study and the development of the manuscript were supported by UCB Pharma. UCB Pharma reviewed the text to ensure that from a UCB perspective, the data presented in the publication are scientifically, technically and medically supportable, that they do not contain any information that has the potential to damage the intellectual property of UCB, and that the publication complies with applicable laws, regulations, guidelines and good industry practice. The authors approved the final version to be published after critically revising the manuscript for important intellectual content.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LB: Advisory boards/consulting, and/or received research grants: Amgen, BMS, Janssen, Roche, UCB Pharma, AbbVie, Pfizer, Merck, Celgene, Sanofi, Eli Lilly and Novartis; BH: Advisory boards/consulting, and/or received research grants: AbbVie, Amgen, BMS, Celgene, Janssen, Eli Lilly, Merck, Novartis, UCB Pharma and Pfizer; AC: Advisory boards/consulting, and/or received research grants: AbbVie, Amgen, AstraZeneca, BMS, Celgene, Eli Lilly, Genzyme, GSK, Janssen, Merck, Novartis, Pfizer, Roche, Sanofi Aventis, UCB Pharma; IF, SD: None declared; MK: Received research grants: Abbott, Amgen and Pfizer; DH: Advisory boards/consulting, conducted research, and/or received grants: AbbVie, Amgen, AstraZeneca, Adiga Life Sciences, Abbott, BMS, Celgene, Circassia, GSK, Janssen, Eli Lilly, Novartis, Pfizer, Roche, Sanofi Genzyme, Takeda, and UCB Pharma; SE, JS: Employees of UCB Pharma; SS: Consulting: Roche, Eli Lilly, Sanofi, and Amgen.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.