
Abstract
Background:
Biological DMARDs (bDMARDs) have been proven to prevent joint damage and bone erosions. Nevertheless, approximately 15% of rheumatoid arthritis (RA) patients on bDMARDs will progress despite good control of joint inflammation.
Objectives:
The objective of our study is to investigate the factors associated with radiological progression of patients treated with bDMARDs.
Design:
We conducted a retrospective analysis of longitudinally collected data on RA patients starting bDMARDs.
Methods:
Presence or development of new erosions was assessed by a skilled rheumatologist at the time of the visit (baseline and 12 months thereafter). To determine the predictors of erosions, we employed multivariable logistic regression models. Discriminatory capacity for the prediction of new erosion development was assessed with receiver operating characteristic (ROC) curve, which was based on the logistic regression model.
Results:
A total of 578 RA patients starting bDMARDs were included in the study. Overall, 46 patients (approximately 10%) had radiographic progression (at least one new erosion) at 12 months of follow-up. The factors independently associated with higher risk of developing new erosions while on bDMARD were younger age, high disease activity at baseline, not being treated with cDMARDs, and presenting with erosions at baseline. In addition, we built a predictive model that can accurately foresee new erosions (AUC 0.846) in patients receiving bDMARDs
Conclusion:
We found that baseline erosive disease, higher disease activity during treatment, younger age, and monotherapy were the factors independently associated with the development of bone erosions. Our study may inform future targeted intervention in RA patients at risk of radiographic progression.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory joint disease with possible systemic involvement, characterized by cartilage and bone damage. 1 The prevention of bone erosions is critical to avoid future disability. 2 Early treatment initiation targeting clinical remission represents crucial goal of RA treatment. 3 In the span of the last century, disease-modifying anti-rheumatic drugs (DMARDs) have become largely available, leading to better outcomes and good quality of life for RA patients. In addition, biological DMARDs (bDMARDs) have been proven to prevent joint damage and bone erosions. 4 Nevertheless, 10–15% of RA patients on bDMARDs will, sooner or later, experience radiographic progression even in spite of good control of joint inflammation. 5 The pathogenesis of these bone erosions is largely unknown. Unraveling the factors associated to the development of bone erosions in such patients is crucial in order to target intervention. The objective of this study is to investigate the factors associated to the development of bone erosion in RA patients treated with bDMARDs.
Material and methods
Data collection
We retrospectively analyzed prospectively collected data of patients with RA starting bDMARDs at the outpatient service of the Rheumatology Unit of the University of Verona from January 2016 through January 2020. Patients were seen every 3–4 months as per clinical practice. Inclusion criteria were (1) diagnosis of RA according to ACR/EULAR 2010 classification criteria, 6 (2) age ⩾ 18 years, and (3) starting treatment bDMARDs. Patients on bDMARDs received treatment according to the manufacturer’s instructions at full dosage. The following clinical, radiological, and demographic parameters were collected: gender, age, weight, height, disease activity score on 28 joints (DAS28), C-reactive protein (CRP) serum levels, X-ray of hands and feet, disease duration, systemic treatment with conventional, and biological therapies including methotrexate, leflunomide, infliximab, etanercept, adalimumab, golimumab, certolizumab pegol, rituximab, abatacept, tocilizumab, baricitinib, and tofacitinib. Presence or development of new erosions was assessed by a skilled rheumatologist at the time of the visit. X-ray of hands and feet were performed at baseline and at month 12.
Statistical analyses
Group comparisons were performed using a Student’s t-test and Mann–Whitney U-test (for normally and non-normally distributed continuous variables, respectively). We employed multivariable logistic regression models to determine the predictors of erosions at baseline (before bDMARD start) and the predictors of development of new erosions during treatment. Discriminatory capacity for the prediction of new erosion development was assessed with receiver operating characteristic (ROC) curve, which was based on the logistic regression model (new erosion as binary dependent variable). Differences were considered significant at p < 0.05. All statistical analyses were performed using SPSS version 26 (SPSS, Inc., Chicago, IL, USA) and GraphPad Prism 9.3.1 (GraphPad Software, San Diego, CA, USA). The reporting of this study conforms to the STROBE statement. 7 The methodology of this study can be reproduced freely.
The study was conducted according to the protocol BIOREVE 534CESC approved by the University of Verona local Ethic Committee, in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. All patients provided signed informed consent for treatment, data collection, and publication.
Results
Baseline characteristics
We included data on consecutively selected 578 patients with RA starting bDMARD with 2625 follow-up visits every 6 months over a median follow-up of 1.8 years [interquartile range (IQR): 1.1–2.8]. In Table 1 are presented the descriptive characteristics of the population. At baseline, 296 (51.2%) patients had an erosive disease and 344 (59.5%) had seropositive RA.
Baseline characteristics of the cohort.
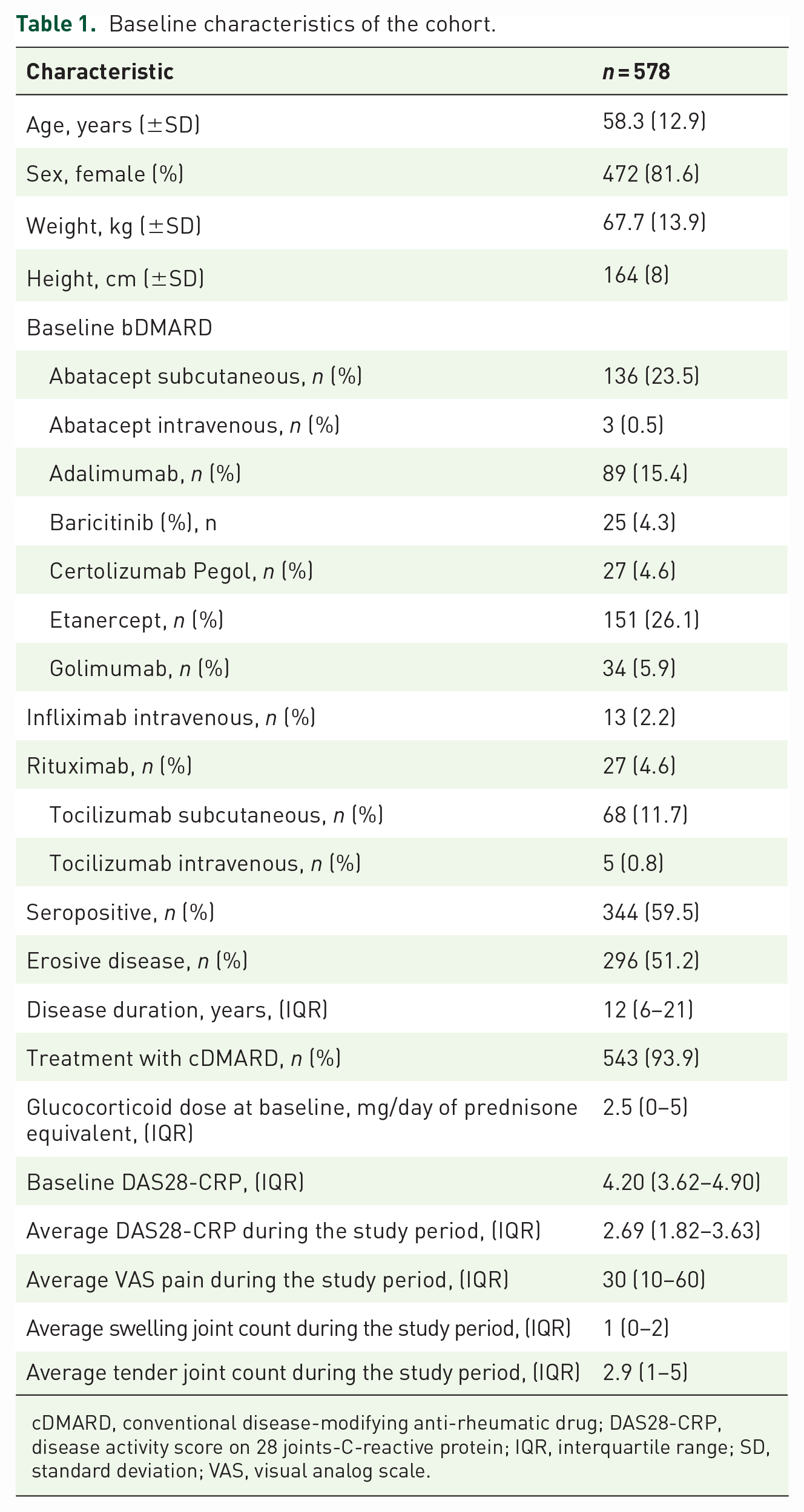
cDMARD, conventional disease-modifying anti-rheumatic drug; DAS28-CRP, disease activity score on 28 joints-C-reactive protein; IQR, interquartile range; SD, standard deviation; VAS, visual analog scale.
Factors associated with erosive disease at baseline
In Table 2 are presented the factors associated with erosive disease at baseline. We found that older age and higher DAS28-CRP were associated with higher risk of presenting with erosions at baseline, whereas greater body mass index (BMI) was protective. Seropositive patients had 50% higher risk of presenting with bone erosions compared to seronegative patients [adjusted odds ratio (aOR) 1.549, 95% confidence interval (CI): 1.090–2.205]. We found no influence of gender, disease duration, treatment with cDMARD, or glucocorticoids on the risk of erosions at baseline.
Factors associated with erosions at baseline, before initiation of bDMARD.
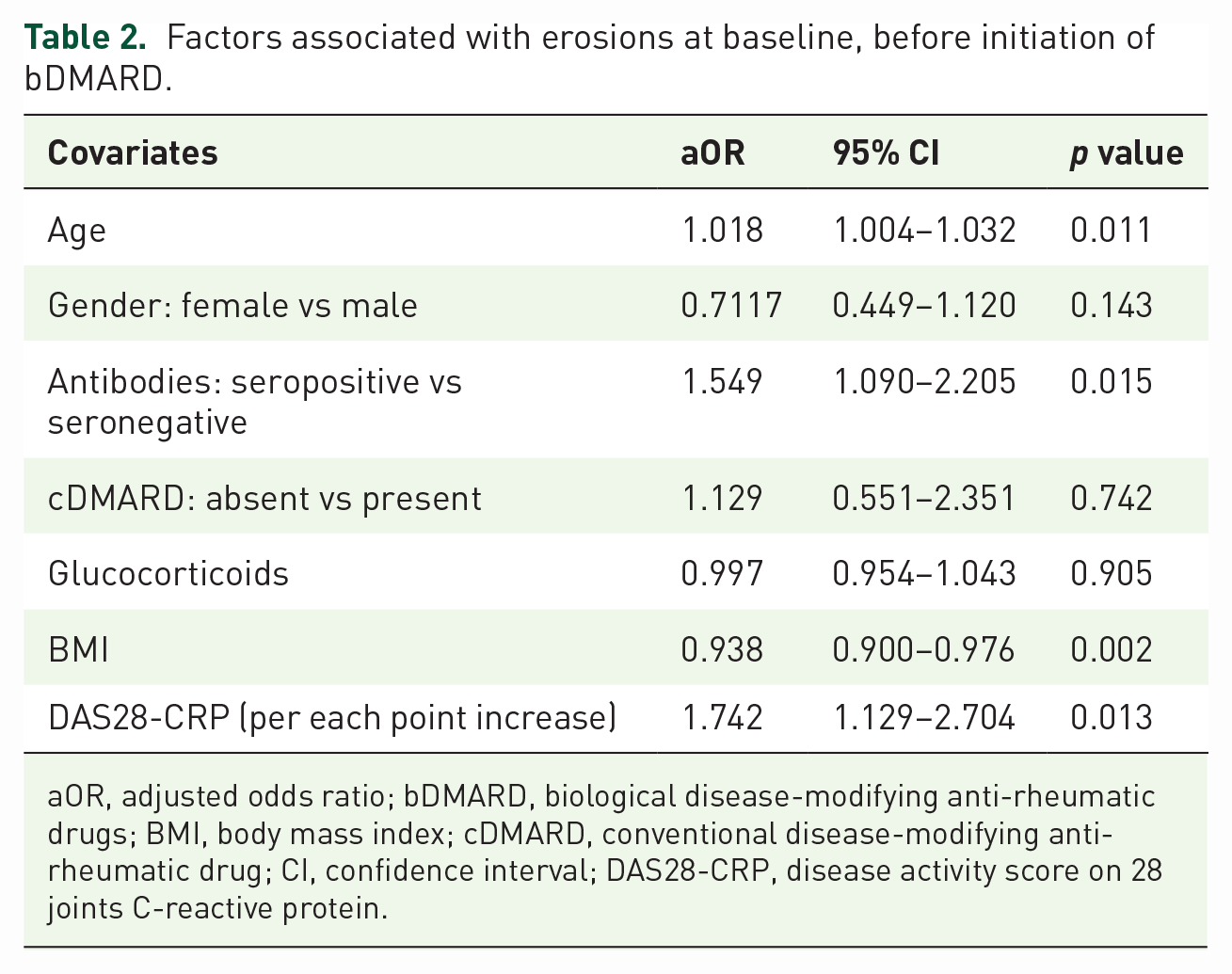
aOR, adjusted odds ratio; bDMARD, biological disease-modifying anti-rheumatic drugs; BMI, body mass index; cDMARD, conventional disease-modifying anti-rheumatic drug; CI, confidence interval; DAS28-CRP, disease activity score on 28 joints C-reactive protein.
Factors associated with development of new erosions
Among the whole cohort, 429 patients underwent radiographic evaluation at 12 months of follow-up and represented the sample for the prediction of erosion development. Overall, 46 patients (10.7%) had radiographic progression (at least one new erosion) at 12 months of follow-up. The factors independently associated with higher risk of developing new erosions while on bDMARD were younger age, high disease activity at baseline, not being treated with cDMARDs (aOR: 2.068; 95% CI: 1.053–4.034) and presenting with erosions at baseline (7.820, 95% CI: 5.073–12.410). In Table 3 are presented the results of the multivariable logistic regression analysis. In Figure 1 is depicted the ROC curve for the prediction ability of the model for the detection of new erosions (AUC: 0.846).
Factors associated with development of new erosions in rheumatoid arthritis patients starting bDMARDs and tsDMARDs.

aOR, adjusted odds ratio; bDMARD, biological disease-modifying anti-rheumatic drugs; tsDMARD, targeted synthetic disease-modifying anti-rheumatic drugs; BMI, body mass index; cDMARD, conventional disease-modifying anti-rheumatic drug; TNFi, tumoral necrosis factor inhibitors; IL6, interleukin 6; JAK, janus kinases; CI, confidence interval; DAS28-CRP, disease activity score on 28 joints-C-reactive protein; MOA, mechanism of action of bDMARD.
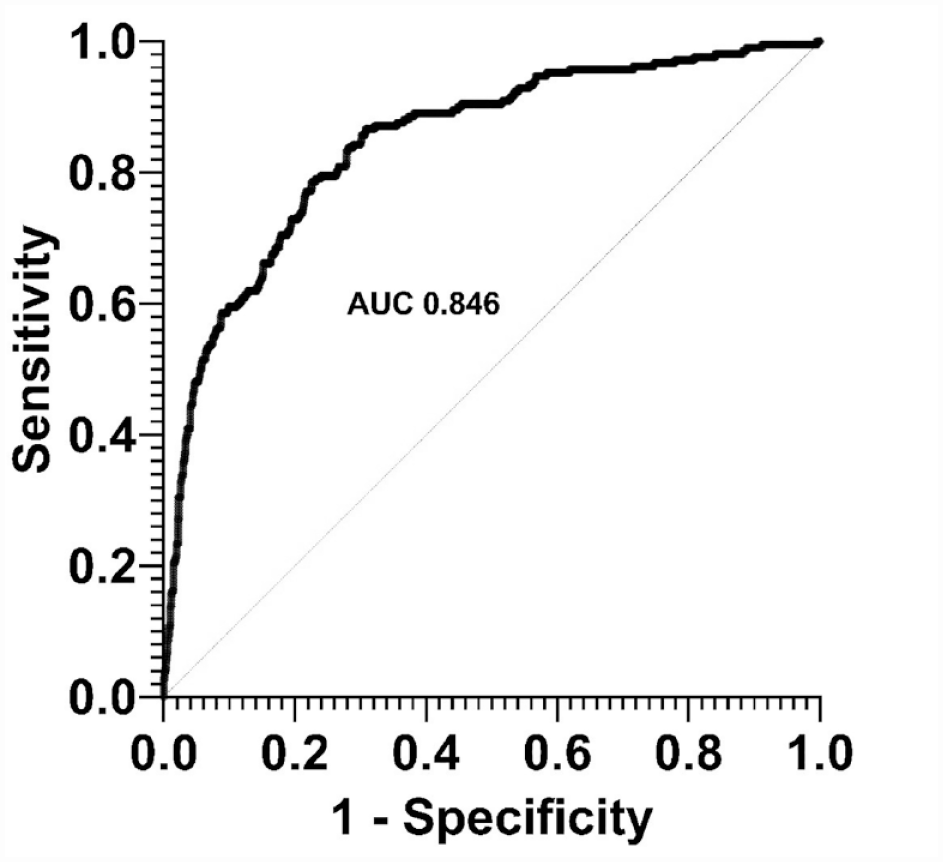
Receiver operator characteristic (ROC) curve for the prediction of development of new erosions during the treatment with bDMARD.
Discussion
Herein we conducted a longitudinal observational study on the factors associated with radiographic progression in patients with RA treated with bDMARDs. Overall, we found that prevalent erosions at baseline, higher disease activity, younger age, and monotherapy were the factors independently associated with the development of bone erosions during the treatment. In addition, we built a predictive model that may accurately foresee new erosions (AUC 0.846) in patients receiving bDMARDs.
Our study adds to the body of the literature on the factors associated with radiographic progression in RA.2,4,8 With our real-life experience, we have confirmed that younger patients, who are likely being in the early stages of the disease, are at higher risk of developing erosions. 5 In addition, patients with erosions and more severe disease before treatment initiation are more likely to progress over the time. These findings further support an early and aggressive treatment to target remission in all early RA, independently from autoantibodies positivity and other clinical factors.
In contrast to part of the established literature,8–11 we did not find any significant association between autoantibodies and risk of radiographic progression in RA. However, we did find an association between baseline erosions and autoantibodies. This controversial result might be explained by a possible channeling bias that has led to selection bias in the cohort. Indeed, according to the EULAR recommendations, 3 seropositive patients might have been treated more aggressively and earlier than seronegative patients, possibly reducing the risk of new erosions in the former group. In addition, part of the detrimental effect induced by autoantibodies might have been blunt by the erosions score at baseline.
Concomitant treatment with cDMARDs was associated with lower chance of radiographic progression among patients receiving bDMARDs. Our finding is in line with the existing literature and further supports the need for combination treatment, especially in patients at high risk of progression. However, the majority of the cohort was treated with tumor necrosis factor (TNF)-inhibitors; therefore, no strong conclusion can be drawn on other mechanisms of action which might behave differently in monotherapy.
We found that BMI was protective against erosions at baseline. This finding is in line with another study published in 2018 by Rydell and colleagues. 8 The authors found that high BMI was associated with reduced risk of severe joint damage. Lower BMI might be indeed a proxy for prominent inflammatory status in RA patients. As a matter of fact, inflammation has been consistently associated with weight loss and lower BMI. In contrast, in the SWEFOT trial obesity was found to be associated with a higher risk of worse clinical outcomes. 12 Nonetheless, obesity was not independently associated with radiographic progression even in the SWEFOT trial. 12 We may therefore speculate on a possible J-shaped relationship between obesity and clinical outcomes or radiographic progression. In other words, very low and very high BMI might pose a risk for patients with RA, whereas normal range BMI might have the best outcomes.
We found that approximately 10% of patients on bDMARDs developed a new erosion at 1 year of follow-up. This result is in line with other studies in the literature,5,10 further confirming the representativeness of our cohort and the generalizability of the results.
Our study has strengths and limitations. The main strength is the large sample of patients affected by RA naïve to bDMARDs followed over a long period. However, we did not have access to other possible determinants of bone erosions, such as bone turnover markers or other biomarkers or environmental conditions which have been associated with radiographic and clinical progression in RA.13–19 As a matter of fact, approximately 15% of the new erosions that occurred in our cohort of patients were not explained by the logistic regression model. We did not have access to other autoantibodies that have been shown to predict erosions 20 possibly reducing our model ability to predict radiographic progression. In addition, this was a retrospective study, which might be flawed by selection bias.
Conclusion
In summary, we described the factors associated with higher risk of developing new bone erosions in RA patients. Our study may help inform future risk reduction strategies in patients receiving bDMARDs at risk of radiographic progression.