
Abstract
Sternocostoclavicular hyperostosis (SCCH) is a chronic inflammatory disorder which presents with erythema, swelling, and pain of the sternoclavicular joint. Approximately one half of patients have acne or pustular lesions with the best described association being with palmoplantar pustulosis (PPP). Extrasternal articular disease occurs in about a quarter of patients. The inflammatory process spans several years and has periods of exacerbation followed by remission. The histologic picture demonstrates a sterile osteomyelitis of the sternum and medial end of the clavicle. The diagnosis of SCCH is confirmed radiographically by hyperostosis and sclerosis of the sternum with involvement of the first rib on computed tomography (CT). The focal uptake of radiopharmaceutical on bone scintigraphy called the ‘bullhead’ sign is highly sensitive of SCCH. Treatment is aimed at easing pain and modifying the inflammatory process. Evidence over the last two decades suggests a role for intravenous bisphosphonates and tumor necrosis factor alpha inhibitors. A low level of awareness of SCCH often leads to a delay in diagnosis. This translates into significant morbidity and brings a psychological burden. Untreated chronic inflammation of the sternoclavicular joint leads to restricted mobility and secondary degenerative joint changes. In the search for a diagnosis, patients often undergo multiple serologic and imaging studies and in the experience of the author are referred to multiple specialists before a correct diagnosis is made. Greater awareness of SCCH is needed to prevent the irreversible physical and psychological impairments associated with the disease.
Introduction
Although it was speculated that the clinical and radiographic manifestations of sternocostoclavicular hyperostosis (SCCH) were initially described in the early 20th century [Chigira and Shimizu, 1989] the first case of SCCH appeared in the Japanese medical literature in 1967 when Sasaki reported a Japanese patient who had ‘bilateral clavicular osteomyelitis accompanied by palmar and plantar pustulosis’ [Dihlmann and Dihlmann, 1991, p. 250; Sasaki, 1967]. In 1974 Sonozaki and colleagues reported the first case of SCCH in English [van der Kloot et al. 2010; Sonozaki et al. 1974]. Cases published between the late 1960s and early 1970s reported patients with bilateral hyperostosis of the clavicles uniformly associated with pustulosis of the palms and soles [Fritz et al. 1992]. The first case of SCCH reported in the Western medical literature with similar clinical and radiographic findings appeared in the German medical literature in 1975 [van der Kloot et al. 2010; Köhler et al. 1975]. In 1979 Sonozaki and colleagues [Sonozaki et al. 1979] coined the term intersternocostoclavicular ossification based on the sternoclavicular findings in a cohort of over 20 Japanese patients. By the early 1990s SCCH had over 50 synonyms such as pustulotic arthro-osteitis, pustulotic arthro-osteopathy, hyperostotic pustulopsoriatic spondyloarthropathy, and acquired hyperostosis syndrome [Dihlmann and Dihlmann, 1991]. A more commonly applied term has been the acronym SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome [Chamot et al. 1987]. It was first introduced by Chamot and colleagues in 1987 to describe a group of bone and joint abnormalities associated with skin lesions. While there is overlap between the clinical, histological, and radiographic manifestations of SAPHO syndrome and SCCH, it is recognized that SAPHO syndrome is a heterogeneous disorder [Schilling, 2003] and SCCH continues to appear as a distinct medical and diagnostic term publishable in the literature [van der Kloot et al. 2010]. For these reasons SCCH will be the term used to categorize the clinical, histologic, and radiographic findings discussed in this review.
SCCH is considered a rare disorder [van der Kloot et al. 2010] with no well defined incidence because the current literature consists of case reports and case series. It is a disorder of midlife with a relatively broad age range. A recent series of 52 patients reported ages ranging between 24 and 79 years [van der Kloot et al. 2010]. One explanation for such a broad age range is that the clavicle can be involved in other arthritic disorders. Condensing osteitis of the clavicle, a rare but benign condition which has clinical and radiographic findings similar to that of SCCH, can occur in women in their late childbearing years without a dermatosis [Noble, 2003; Tait et al. 1994]. Chronic recurrent multifocal osteomyelitis (CRMO), a disorder which has the same hyperostotic changes in the sternum and clavicles, occurs exclusively in patients from infancy to young adulthood [Fritz et al. 1992]. While some thought that SCCH was on a continuum with CRMO [Fritz et al. 1992; Dihlmann and Dihlmann, 1991], more recent authors have argued that the two diseases have no distinguishable features [Katz et al. 1989]. Insight about the ethnic prevalence of SCCH information remains limited because case series variably report data about the ethnicity of their patients. While the majority of patients may be Japanese, European/ White patients make up a significant minority [Johnston and Elston, 1998]. To date, only one other case has reported a patient of African descent [Kalke et al. 2001]. While a male predominance was previously reported, recent case series suggest a female predominance [van der Kloot et al. 2010; Economou et al. 1993].
Pathophysiology
The sternoclavicular joint is a true synovial lined articulation composed of the inferior portion of the medial head of the clavicle, an indentation in the upper outer portion of the sternum, and the cartilage of the first rib [Yood and Goldenberg, 1980]. The joint is divided into two compartments which in nearly all people is separated by an intra-articular disc. The articular capsule surrounding the sternoclavicular joint is reinforced anteriorly and posteriorly by ligaments as well as superiorly by the interclavicular ligament. The costoclavicular ligaments extend from the cartilage of the first ribs to the clavicles and are each separated into an anterior and posterior sheet by a bursa [Yood and Goldenberg, 1980]. Surrounding structures like the sternomanubrial joint form a symphysis rather than a true synovium and the costochondral joints form synchondroses [Katz et al. 1989]. Thus the sternoclavicular joint area possesses a variety of structures that can potentially be involved in an inflammatory arthritis or enthesitis [Katz et al. 1989].
SCCH typically starts with nonspecific inflammation of the sternoclavicular ligaments [Fritz et al. 1992]. Surrounding soft tissues may also be involved in the early inflammatory process [Saghafi et al. 1993] and perichondritis appears to play a more important role than a true arthritis [Chigira and Shimizu, 1989] but eventually an erosive arthritis develops [Fritz et al. 1992; Dihlmann and Dihlmann, 1991]. As the inflammatory process continues, endosteal and periosteal bone formation occurs along with the growth of partially destructive fibrous tissue [Fritz et al. 1992]. Chronic inflammation leads to progressive hyperostosis and eventual soft tissue ossification [Fritz et al. 1992; Sartoris et al. 1986]. After several years of chronic inflammation, fusion of the sternoclavicular joints may occur [Fritz et al. 1992]. Concomitant with the hyperostosis involving the sternoclavicular joint, similar enthesopathic and hyperostotic changes may involve the shafts of the long bones, sacroiliac joints, or peripheral joints [Johnston and Elston, 1998].
Histologically SCCH resembles a nonspecific inflammatory cellular response akin to that seen in chronic osteomyelitis or Paget's disease [Nungu et al. 1997; Economou et al. 1993; Sartoris et al. 1986]. The disorder starts with an ossifying periostitis, with newly formed periosteal bone fusing with the existing cortex and the original trabecular bone adapting to this alteration [Kalke et al. 2001; Köhler et al. 1977]. As the inflammatory response continues, bone turnover accelerates, resulting in formation of woven bone and the appearance of osteoid seams [Kohler et al. 1977]. Thickening of trabecular bone, formation of osteoid and fibrous tissue, and round cell infiltrates can also be found [Fritz et al. 1992; Sartoris et al. 1986]. In some cases granulation tissue accumulates and angiogenesis occurs [Fritz et al. 1992; Sartoris et al. 1986]. Inflammation at junctional sites may slowly extend to involve all of the entheses around the manubrium [Economou et al. 1993]. Eventually the inflammatory process diminishes or resolves leaving the characteristic hyperostotic bone changes in the sternoclavicular area and a nonspecific osteosclerosis [Fritz et al. 1992; Köhler et al. 1977].
To date no etiology has been linked to the pathogenesis of SCCH. Based on the response of early case reports to antibiotics an infectious trigger was initially an appealing etiology, however more recent case series have cast significant doubt on such efficacy [Noble, 2003; Freyschmidt and Sternberg, 1998; Taylor and Dawes, 1992]. The association of SCCH with pustular dermatoses led some authors to conclude that both conditions were triggered by a ‘bacterid reaction’ [Chigira and Shimizu, 1989]. Propionibacterium acnes was implicated as a possible infectious agent in patients with SCCH and palmoplantar pustulosis (PPP) in the 1980s, but little has been published since then to support such an association [Saghafi et al. 1993; Karagevrekis et al. 1990].
Clinical manifestations
SCCH very infrequently may be asymptomatic with radiographic findings only [Katz et al. 1989] but in most cases the disorder presents with pain and palpable tenderness in the sternoclavicular region [Dihlmann and Dihlmann, 1991; Chigira and Shimizu, 1989]. Local swelling and warmth is almost always present [Chigira and Shimizu, 1989]. Symptoms can be unilateral [Economou et al. 1993] but most patients develop bilateral involvement [Prevo et al. 1989; Sartoris et al. 1986]. Symptoms are often chronic in nature and have a relapsing and remitting course [Kalke et al. 2001; Economou et al. 1993; Prevo et al. 1989; Sartoris et al. 1986; Köhler et al. 1977]. Pain is typically reported in the shoulder, neck, or upper anterior chest wall area with swelling and tenderness of the sternoclavicular area invariably present [Kalke et al. 2001; Economou et al. 1993]. Resultant to inflammation of the medial clavicle, motion of the ipsilateral shoulder is often restricted [Economou et al. 1993; Chigira and Shimizu, 1989]. Sternoclavicular joint pain may be provoked by shrugging or retracting the ipsilateral shoulder [Kalke et al. 2001]. In advanced cases, the shoulder girdle may become fixed in a ‘squared shoulder’ position [Economou et al. 1993].
Extrasternal articular manifestations may be encountered in SCCH. There is limited information on whether or not these manifestations precede, occur during, or develop after the onset of sternoclavicular area inflammation. Multiple reports since the early 1980s suggest that axial skeleton manifestations can occur in around 50% of patients but these reports commented on radiographic changes only [Fritz et al. 1992; Sartoris et al. 1986]. Information about the symptoms associated with axial skeleton inflammation remains limited. Symptomatic peripheral arthritis may occur in up to 22% of patients [Kalke et al. 2001; Fritz et al. 1992]. The peripheral arthritis of SCCH is typically an oligoarthritis [Fritz et al. 1992] that preferentially involves large joints [Kalke et al. 2001] with the knee and ankle most frequently involved, followed by the wrist and less commonly the proximal interphalangeal joints [Kalke et al. 2001].
Since it was first recognized, SCCH has classically been associated with pustulotic skin changes, specifically PPP. In addition to PPP, other dermatoses associated with SCCH are pustular psoriasis, acne conglobata, acne fulminans, hidradenitis suppurativa, and psoriasis vulgaris [Taylor and Dawes, 1992; Dihlmann and Dihlmann, 1991]. A recent study reported that 53.9% of patients had current or prior skin manifestations [van der Kloot et al. 2010]. In the majority of patients (70%) the interval between the onset of skeletal symptoms and skin disease was less than 2 years [Freyschmidt and Sternberg, 1998] yet patients may present with PPP 2 years before SCCH or up to 5 years later [Nungu et al. 1997; Sartoris et al. 1986].
There are no laboratory tests that are diagnostic of SCCH and the value of serologic testing is to exclude alternative disorders [Nungu et al. 1997]. While initial case reports documented markedly elevated values for inflammatory markers such as erythrocyte sedimentation rate (ESR), α2-globulin, and C-reactive protein, it is now recognized that changes in these labs do not relate to the disease activity or course [Nungu et al. 1997]. Although SCCH is a hyperostotic process, only normal to slight elevations in the alkaline phosphatase have been reported [Nungu et al. 1997; Fritz et al. 1992]. Tests for rheumatoid factor and other immunological tests are usually negative [Economou et al. 1993]. Although patients of European descent may demonstrate a slightly increased prevalence of HLA-B27 positivity, no clear relationship to SCCH has been demonstrated [Dihlmann and Dihlmann, 1991].
Imaging
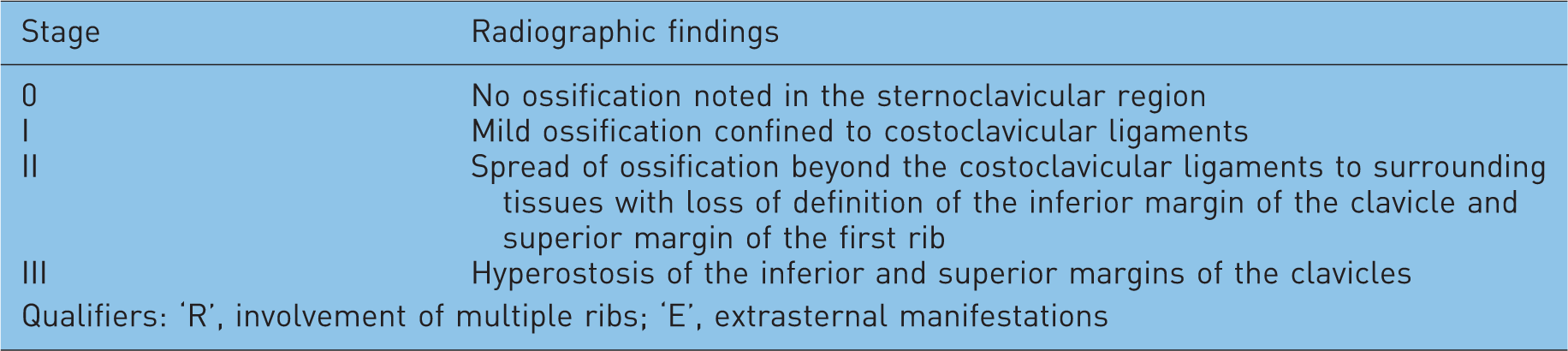
The characteristic radiographic changes of SCCH are ossification progressing to hyperostosis of the clavicles, sternum, and anterior upper ribs [Prevo et al. 1989; Dehdashti and Siegel, 1989]. Early in the disorder it is possible that no radiographic changes may be present, thus the prominence of ossification and hyperostosis depends on disease chronicity. Recognizing this, Sonozaki and colleagues in the late 1970s proposed a radiographic staging system for SCCH [Dehdashti and Siegel, 1989]. This is shown in Table 1. The most common radiographic stage at the time of diagnosis is stage II [Fritz et al. 1992; Dehdashti and Siegel, 1989] and multiple authors have reported that such changes infrequently progress even in the presence of continued inflammation [Economou et al. 1993; Fritz et al. 1992; Prevo et al. 1989; Sartoris et al. 1986]. Chigira and Shimizu added a stage 0 to the Sonozaki staging in which no ossification could be clearly demonstrated [Chigira and Shimizu, 1989]. Joint spaces in the sternoclavicular region initially are preserved, but as the disorder progresses radiographic evidence of erosive changes predominantly in the sternoclavicular joint may be detected [Fritz et al. 1992; Dihlmann and Dihlmann, 1991]. Recognizing that ossification and hyperostotic changes occur beyond the sternoclavicular region, Fritz and colleagues further modified the Sonozaki staging in 1992 by adding the qualifiers of ‘R’ for concomitant involvement of multiple ribs and ‘E’ for concomitant extrasternal manifestations [Fritz et al. 1992]. These modifications have been included in Table 1.
Radiographic staging of sternocostoclavicular hyperostosis proposed by Sonozaki et al. [Dehdashti and Siegel, 1989; Sonozaki et al. 1979] with modifications by Chigira and colleagues [Chigira and Shimizu, 1989] and Fritz and colleagues [Fritz et al. 1992].
Sternal involvement in SCCH can involve the first to fourth ribs [Prevo et al. 1989; Sartoris et al. 1986; Köhler et al. 1977] but some case series have reported involvement to the seventh rib [Fritz et al. 1992]. Ossification involving or beyond the eighth rib has not been reported [Fritz et al. 1992]. Radiographic axial involvement may appear as erosive changes and exuberant bone formation along the anterior aspects of the vertebral bodies [Karagevrekis et al. 1990; Dehdashti and Siegel, 1989]. It can also appear as sclerotic changes without proliferative or destructive changes [Fritz et al. 1992]. Anywhere from 41% to 55% of patients in various case series have had radiographic findings [Fritz et al. 1992; Sartoris et al. 1986]. Any part of the cervical, thoracic, or lumbar spine may be involved, and the changes reported have been compared to an ‘erosive spondyloarthropathy’ [Prevo et al. 1989; Sartoris et al. 1986]. Radiographic changes similar to those seen in diffuse idiopathic skeletal hyperostosis and ankylosing spondylitis have also been reported [Dehdashti and Siegel, 1989].
As a more sensitive imaging modality, computed tomography (CT) has the ability to detect abnormalities in the sternoclavicular area not obvious on radiographs (stage 0). CT facilitates earlier detection of pathologic changes in SCCH and changes found can differ from those on radiographs [Economou et al. 1993]. Chigira and Shimizu 1989 devised a staging system for the CT findings for SCCH [Economou et al. 1993; Chigira and Shimizu, 1989], which is shown in Table 2. Typical CT changes involving the sternoclavicular joint are shown in Figure 1. Given the sensitivity of CT, it is possible to ‘over-call’ age-related changes such as calcification and ossification of the costal cartilage [Dihlmann and Dihlmann, 1991, p. 261]. Dihlmann and Dihlmann reported that ‘both inflammatory enthesopathy of the costoclavicular ligament and the occurrence of small hyperostotic foci of at least 5 mm diameter at the sternal end of the first pair of ribs are among the diagnostically decisive early findings' in the sternoclavicular area in SCCH [Dihlmann and Dihlmann, 1991]. When these changes are identifiable they can help establish SCCH as a diagnosis early in the disease course.
Computed tomographic (CT) staging of sternoclavicular hyperostosis proposed by Chigira and colleagues [Chigira and Shimizu, 1989; Economou et al. 1993].


Axial (left) and coronal (right) images of right sternal (black arrow) and clavicular (black arrowhead) erosions with early enthesophyte (white arrow) involving the right clavicular head.
Scintigraphy is another imaging modality able to identify uptake in characteristic regions when clinically SCCH is mild and radiographic changes are absent or subtly abnormal [Kim et al. 2001; Nungu et al. 1997; Dehdashti and Siegel, 1989; Sartoris et al. 1986]. Increased uptake is almost always found in the sternoclavicular joint area, the costal cartilages of the first and second ribs, and the manubrium [Kalke et al. 2001; Dihlmann et al. 1997]. The predominant uptake in these areas has lead several authors to label this configuration as the ‘bullhead’ sign [Freyschmidt and Sternberg, 1998; Dihlmann et al. 1997]. This scintigraphic finding is shown in Figure 2. This sign is defined as the ‘typical, mostly symmetrical high uptake of the sternoclavicular region like a “bullhead”: the manubrium representing the upper skull of the bull and the horns corresponding to the inflamed sternoclavicular joints and the adjacent claviculae' [Freyschmidt and Sternberg, 1998, p. 808]. Although the shape can be modified or slightly asymmetric, the characteristic pattern is considered to be always visible [Freyschmidt and Sternberg, 1998]. While some authors have argued that the ‘bullhead’ sign is both sensitive and specific for SCCH [Jurik, 1991], the specificity of this finding is dependent on the presence of skin lesions. When patients with pustular skin changes are removed the specificity has been found to be lower than that noted earlier [Dihlmann et al. 1997]. To distinguish patients who have true sternoclavicular joint involvement caused by SCCH, Dihlmann and colleagues recommended anterior and posterior scanning with increased uptake in both areas being consistent with an inflammatory process [Dihlmann et al. 1997].
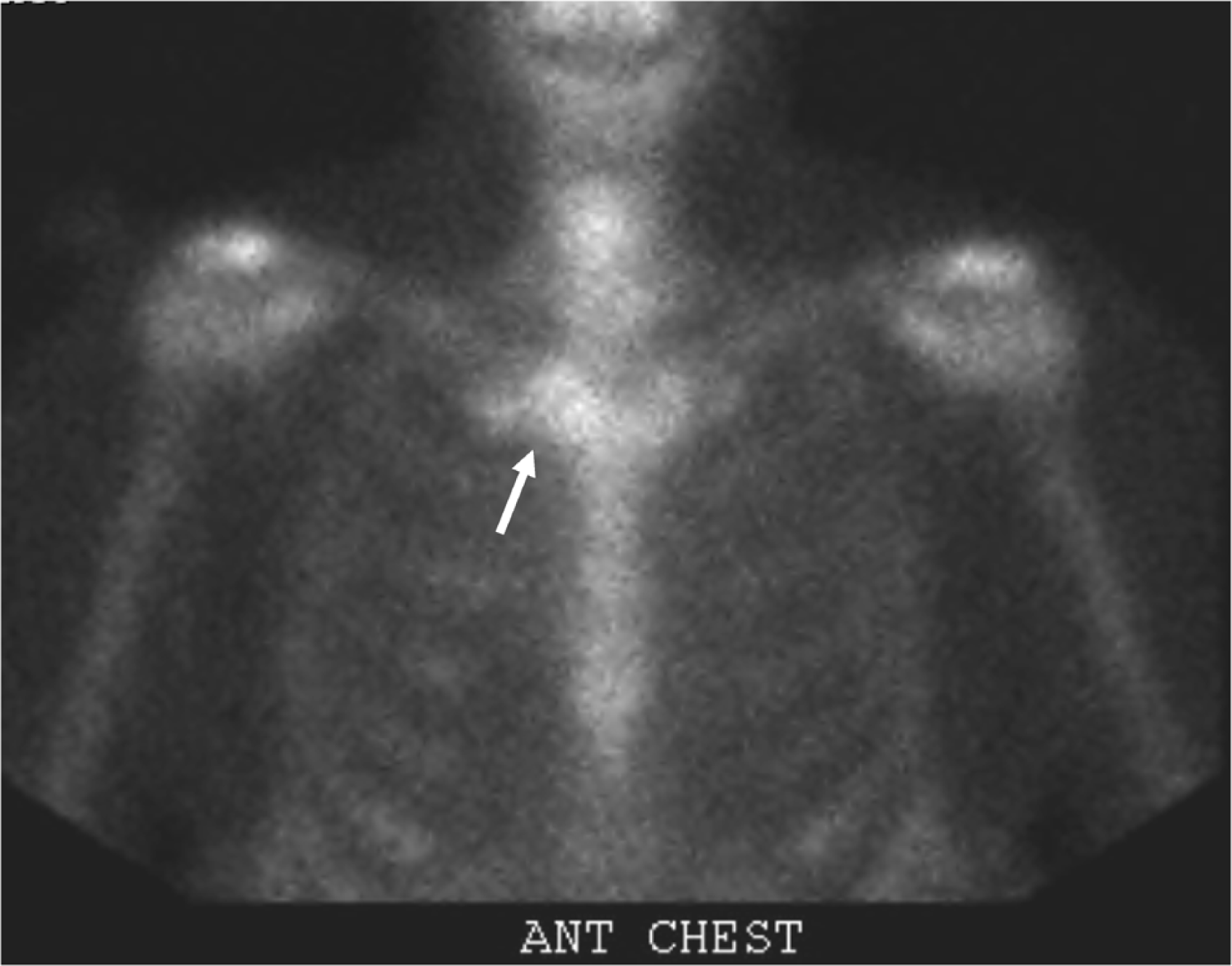
Bone scan image demonstrating increased uptake in the area of the sternoclavicular joints appearing like the head of a bull, the ‘bullhead’ sign (white arrow).
In addition to the somewhat distinctive ‘bullhead’ sign, scintigraphy also has the advantage of identifying additional sternal and extrasternal involvement, even when the patient is asymptomatic [Kim et al. 2001; Freyschmidt and Sternberg, 1998; Dihlmann et al. 1997; Fritz et al. 1992]. In one series scintigraphic changes in the axial skeleton were noted in up to 67% of patients and in the peripheral joints in 29% [Freyschmidt and Sternberg, 1998]. It has been argued that scintigraphy should be considered in patients with anterior chest wall symptoms suspicious for SCCH since it can be useful investigating the extent and intensity of disease [Dihlmann et al. 1997].
Differential diagnosis
A variety of conditions can produce the clinical or radiographic findings typical of SCCH. Early in the disease when symptoms present with or without radiographic changes, an infectious or neoplastic etiology must be excluded [Dehdashti and Siegel, 1989; Katz et al. 1989]. Salmonellosis, brucellosis, tuberculosis, staphylococcal infection, and syphilis are a few organisms that can cause infection of the sternoclavicular joint or a subacute osteomyelitis [Taylor and Dawes, 1992; Dehdashti and Siegel, 1989]. A pancoast tumor with local extension, thyroid cancer, lymphoma, or metastatic breast or prostate cancer should also be considered in any patient at risk for these neoplasias [Economou et al. 1993; Dihlmann and Dihlmann, 1991; Katz et al. 1989; Prevo et al. 1989]. Aseptic necrosis of the clavicle (Friedrich's disease) and a healing fracture are other conditions to consider early in the disease course [Freyschmidt and Sternberg, 1998; Economou et al. 1993]. Scintigraphically it is possible to distinguish these two disorders from SCCH because they typically do not cause bilateral disease and do not involve joints as well as adjacent bones [Freyschmidt and Sternberg, 1998]. As discussed earlier, condensing osteitis of the clavicle is a benign disorder thought to be a mechanical phenomenon [Lissens et al. 1990; Sartoris et al. 1986; Yood and Goldenberg, 1980]. Changes are restricted to the medial portion of the clavicle with sparing of the sternoclavicular joint [Dihlmann et al. 1997; Tait et al. 1994; Yood and Goldenberg, 1980].
Differentiating SCCH from the seronegative spondyloarthropathies may be challenging at any stage of the illness since this group of arthritides may involve the joints of the sternoclavicular area and distinguishing features may not appear for years after the onset of inflammation. Histologically the mixture of destructive and proliferative bone changes may suggest a seronegative spondyloarthropathy [Freyschmidt and Sternberg, 1998; Dehdashti and Siegel, 1989]. To date, in patients with SCCH there have been no reports of symptoms, examination findings, or imaging abnormalities involving the gastrointestinal tract, the genitourinary tract, or the eyes, even after long periods of follow up. Thus, patients with involvement of these organ systems are more likely to have a seronegative spondyloarthropathy or possibly the SAPHO syndrome and not SCCH.
Treatment
A variety of therapies have been utilized to mitigate the symptoms of SCCH as well as modify disease progression. Traditional analgesic agents such as nonsteroidal anti-inflammatory drugs (NSAIDs) have been tried in most case series (up to 94% in one study) [Kalke et al. 2001]. While improvement in pain with NSAIDs has frequently been reported, the degree and duration of relief is variable [Freyschmidt and Sternberg, 1998; Nungu et al. 1997; Economou et al. 1993; Taylor and Dawes, 1992; Prevo et al. 1989; Köhler et al. 1977]. No significant serologic or radiographic improvements have been reported with the routine use of NSAIDs. In the absence of information to suggest a long-term disease-modifying benefit from the daily use of NSAIDs it is prudent to limit use to pain control [Freyschmidt and Sternberg, 1998]. In the absence of a clear infectious etiology, antibiotics have no role in the treatment of SCCH [Freyschmidt and Sternberg, 1998; Taylor and Dawes, 1992].
In 1990 injectable calcitonin was first reported to be effective in the treatment of some manifestations of SCCH in Japanese patients [Misaki et al. 1991; Lissens et al. 1990]. Injectable eel calcitonin within 48 h improved pain and swelling and produced a quantitative improvement in scintigraphic tracer uptake but did not improve inflammatory markers [Misaki et al. 1991]. No improvement was noted in any facet of SCCH when patients were transitioned to nasal calcitonin [Misaki et al. 1991]. Traditional disease-modifying antirheumatic drugs such as methotrexate and sulfasalazine have been used in some patients but with very limited information available about their efficacy [Kalke et al. 2001]. Cyclosporine A has also been used in some patients and improvement in both the skin and bone manifestations of SCCH has been shown [Freyschmidt and Sternberg, 1998], but renal toxicity and hypertension limit widespread use. A paucity of information currently exists in the medical literature about the role or efficacy of tumor necrosis factor α (TNF-α) inhibitors in SCCH. From the author's experience personally treating several patients with SCCH, methotrexate and sulfasalazine have been marginally effective in improving clinical symptoms and modifying the disease course whereas TNF-α inhibitors such as adalimumab and etanercept seem to be more effective. Prospective trials are needed to validate the efficacy of this class of medications.
Therapeutic interventions have also focused on controlling heterotopic ossification. In the 1970s ‘anti-inflammatory radiation therapy’ was used in four out of five patients whose condition had previously failed to respond to NSAIDs and/ or corticosteroids [Köhler et al. 1977]. Although the long-term follow up was limited and toxicity was a concern, the authors suggested that lasting remission could be achieved with this treatment modality [Köhler et al. 1977]. Bisphosphonates have a similar inhibitory effect on heterotopic bone growth. Case reports suggesting success with the use of pamidronate in patients with refractory symptoms have led to the use of the newer, more potent aminobisphosphonate ibandronate [Ringe et al. 2006]. Ringe and colleagues reported that three patients treated with ibandronate experienced rapid improvement in pain, showed radiographic and scintigraphic evidence of improvement, a gradual decline in ESR, and improvement in bone mineral density despite their condition failing to respond to other pharmacologic and nonpharmacologic interventions [Ringe et al. 2006]. A potential concern with the use of bisphosphonates is that, upon cessation, florid mineralization in areas of suppressed hyperostotic bone formation may occur [Economou et al. 1993].
The role of surgery in SCCH has been restricted to patients whose condition has failed to respond to all other therapeutic interventions [Taylor and Dawes, 1992]. Surgical resection of the medial clavicle or the sternoclavicular joint seems to provide variable improvement in pain, although some authors report no improvement with this intervention [Nungu et al. 1997; Chigira and Shimizu, 1989].
Disease course and complications
Long-term follow up of patients with SCCH suggests most have a good prognosis [Kalke et al. 2001; Economou et al. 1993], although the disease carries a significant psychological burden [van der Kloot et al. 2010]. To date, the longest published follow up of a patient with SCCH has been 31 years [Economou et al. 1993; Fallet et al. 1983]. In SCCH, there seems to be a period of about a decade in which painful exacerbations may occur with transient elevations in ESR and persistence of activity on scintigrams [Economou et al. 1993; Köhler et al. 1977]. Spontaneous remission may occur in patients after the sixth decade of life [Nungu et al. 1997]. Although radiographic changes typically progress slowly, after about 12 years of disease activity ossification of the costoclavicular ligament is universally found [Dihlmann and Dihlmann, 1991]. In a recent study the delay in making the diagnosis was strongly associated with patients feeling they were not being taken seriously, a higher level of emotional distress, more health-related impairments in daily functioning, and increased unemployment [van der Kloot et al. 2010].
A frequently encountered complication of SCCH is chronic ipsilateral shoulder pain with a resultant degenerative arthritis from recurrent inflammation and ultimately fusion of the sternoclavicular joint. Since the 1970s it has been recognized that upper extremity edema and venous congestion from retrosternal soft tissue proliferation and secondary occlusion of the subclavian vein can complicate longstanding SCCH [Economou et al. 1993; Fritz et al. 1992; Dehdashti and Siegel, 1989; Prevo et al. 1989; Sartoris et al. 1986; Köhler et al. 1977]. The retrosternal proliferation of soft tissue and bone creates a thoracic inlet syndrome by compressing local venous structures [Fritz et al. 1992]. Other unusual complications include aortic calcification [Watts et al. 1993], clavicular stress fracture with delayed healing [Kuroda et al. 2005], and chronic sterile discharging sinuses [Wilson and Evans, 1996].
Classification criteria
Confusion from overlapping nomenclature, widespread lack of familiarity with the disorder, and delays in characteristic radiographic changes have hindered formulation of uniform criteria to classify SCCH. There is often a considerable delay in establishing the diagnosis, with the time to diagnosis in one case series between 9 months and 5 years [Economou et al. 1993]. A recent study confirmed that diagnosis of SCCH was on average delayed for 5.6 years [van der Kloot et al. 2010]. Incorporating observations from other authors and multiple case series, the literature suggests that the criteria for classifying SCCH should embrace two tenets [Nungu et al. 1997]:
The presence of clinical inflammation in the sternoclavicular area: pustulotic skin changes are not always required for the diagnosis [Karagevrekis et al. 1990]. Bilateral but occasionally unilateral sternoclavicular involvement can occur. Axial skeleton or a large joint oligoarthritis may be present. There is an absence of symptoms involving other organ systems such as the gastrointestinal tract, the genitourinary system, or the eye (which excludes seronegative spondyloarthropathies). Radiologic, scintigraphic, or CT changes in the sternoclavicular area imaging: scintigraphy has emerged as a useful tool to screen for inflammation of the sternoclavicular area as well as other typical but potentially asymptomatic areas of involvement [Freyschmidt and Sternberg, 1998; Dihlmann et al. 1997; Nungu et al. 1997; Fritz et al. 1992]. The ‘bullhead’ sign on scintigraphy appears to be a highly sensitive sign of SCCH [Kim et al. 2001]. The specificity of this sign is dependent on the presence of pustulotic skin lesions [Freyschmidt and Sternberg, 1998]. Involvement of any rib on radiography or scintigraphy beyond the seventh should decrease suspicion for SCCH [Fritz et al. 1992].
The role of biopsy and histology helps exclude alternative diagnoses. Not all cases reported have had biopsies of areas of inflammation and the histologic picture will evolve with chronicity of the disorder. Several authors have commented that when histology was nonspecific the diagnosis was never made from biopsy alone [Freyschmidt and Sternberg 1998]. The aforementioned features attempt to incorporate the most pertinent findings of SCCH that make it a unique clinical entity and distinguish it from other chronic inflammatory disorders involving the skin and joints.
Conclusion
SCCH is a chronic inflammatory disorder with a predilection for the sternoclavicular joints but it may potentially involve other axial and peripheral joints and in some cases can be associated with pustular skin changes as well. Nomenclature discord has hindered the formulation of a standard definition of findings that constitute the disorder. Rheumatologists as well as other clinicians that evaluate patients with musculoskeletal complaints should familiarize themselves with the clinical and radiographic changes associated with SCCH because a delay in diagnosis has been shown to be associated with irreversible long-term physical and psychological impairments. Although treatment is currently limited, hope may lie in the efficacy of newer bisphosphonates and possibly TNF-α inhibitors.
Footnotes
Acknowledgements
The author confirms that this manuscript has neither been submitted nor is simultaneously being submitted elsewhere. No portion of the data has been or will be published in proceedings or transactions of meetings or symposium volumes. The views expressed in this article are those of the author and do not reflect the official policy or position of the United States Air Force, Department of Defense, or the US Government.
The author has no financial support or other benefits from commercial sources to disclose.
None declared.