
Abstract
Background:
Previous studies have demonstrated that thoracic radiotherapy (TRT) following first-line chemoimmunotherapy improves survival in extensive-stage small cell lung cancer (ES-SCLC). However, its efficacy and safety in elderly patients remain unclear.
Objectives:
To evaluate the efficacy and safety of consolidative TRT in elderly patients with ES-SCLC following first-line chemoimmunotherapy.
Design:
A multicenter retrospective cohort study.
Methods:
Elderly (⩾70 years old) ES-SCLC patients from three large-scale cancer centers who received chemoimmunotherapy in the first line were included, they were divided into two groups according to whether they received TRT. The primary outcomes were overall survival (OS) and progression-free survival (PFS).
Results:
A total of 240 patients who completed four to six of first-line chemoimmunotherapy without progression were included, 83 of whom received consolidative TRT. In the analysis with time zero set at chemoimmunotherapy initiation, TRT was associated with longer median PFS (10.56 vs 8.30 months; hazard ratio (HR), 0.71, p = 0.034) and median OS (18.43 vs 14.39 months; HR, 0.64, p = 0.008). Using time-dependent Cox models with time zero reset to cycle 4 completion to address guarantee-time bias, TRT remained significantly associated with improved OS (14.59 vs 10.92 months; HR, 0.64, p = 0.007) and PFS (7.80 vs 5.12 months; HR, 0.72, p = 0.047). The presence of baseline liver metastasis emerged as an independent adverse prognostic factor. No significant increase in grade ⩾3 adverse events was observed in patients receiving TRT.
Conclusion:
In elderly ES-SCLC patients undergoing first-line chemoimmunotherapy, the addition of TRT is associated with a survival benefit and an acceptable safety profile. These results hold significant implications for current clinical practice and may help inform treatment strategies for elderly patients with ES-SCLC.
Plain language summary
Introduction
Small-cell lung cancer (SCLC), a neuroendocrine malignancy accounting for 13%–15% of lung cancers,1,2 is characterized by aggressive behavior, rapid progression, and poor survival, with approximately two-thirds of patients presenting with extensive-stage disease at diagnosis. 3 As the population ages, the proportion of elderly patients is increasing every year. Epidemiological data from the past four decades reveal a rising trend in the proportion of elderly patients with SCLC, notably, those aged over 70 now constitute nearly half of all cases. 4 Moreover, elderly patients often present with poor baseline health and multiple comorbidities. These factors, compounded by heightened susceptibility to significant adverse effects, collectively contribute to poor treatment tolerance, underscoring the imperative for tailored therapeutic strategies in this clinically significant subgroup.
With the advent of the immunotherapy era, chemotherapy combined with immunotherapy has become the standard first-line therapy for extensive-stage small cell lung cancer (ES-SCLC). 5 In the IMpower133 trial, atezolizumab in combination with chemotherapy significantly prolonged overall survival (OS; 12.3 vs 10.3 months, hazard ratio (HR), 0.70, p = 0.007) and progression-free survival (PFS; 5.2 vs 4.3 months, HR, 0.77, p = 0.02). 6 Similarly, the CASPIAN trial demonstrated a significant OS benefit with durvalumab in combination with chemotherapy (13.0 vs 10.3 months, HR, 0.73; p = 0.0047). 7 Despite high initial objective response rates (ORRs) to chemoimmunotherapy, 8 ES-SCLC remains an aggressively progressive disease. Only 0.8%–2.5% of patients achieve complete remission, 9 and metastatic relapse is a primary driver of disease progression and mortality.10,11 Consequently, controlling thoracic disease is critical for delaying progression and achieving long-term survival. ES-SCLC is highly sensitive to radiotherapy, and prospective studies have indicated that radiotherapy can confer a survival benefit in patients with ES-SCLC who achieve a good response to chemotherapy.12,13 Accordingly, global guidelines recommend consolidative thoracic radiotherapy (TRT) for selected patients with ES-SCLC who respond favorably to first-line chemotherapy, particularly those with residual intrathoracic disease and limited extrathoracic metastases.5,14,15 However, a critical evidence gap remains. Neither the IMpower133 nor the CASPIAN trial incorporated TRT into its study designs, leaving the role of TRT in the modern chemoimmunotherapy era undefined. 16 This gap is particularly salient for elderly patients (aged ⩾70 years), a population that is frequently underrepresented in clinical trials due to poorer baseline health and a higher comorbidity burden. No study to date has evaluated the value of TRT following first-line chemoimmunotherapy specifically in this growing and clinically vulnerable subgroup. Therefore, the purpose of this study was to evaluate the role of TRT in the elderly patients with ES-SCLC by comparing the outcomes of patients who received TRT after first-line chemotherapy combined with immunotherapy versus those who did not.
Patients and methods
Patients
This retrospective cohort study included treatment records from three large-scale cancer centers, namely, elderly patients diagnosed with ES-SCLC at Shandong Cancer Hospital (from May 20, 2020, to December 28, 2023), Tianjin Cancer Hospital (from March 13, 2020, to July 13, 2023), and Shanghai Chest Hospital (from February 11, 2019, to May 6, 2023) were included. We defined elderly patients as those who were ⩾70 years of age at diagnosis. All participants who met the following criteria were eligible for this study: (a) aged ⩾70 years, (b) newly diagnosed, histologically or cytologically confirmed SCLC, (c) had extensive-stage disease as classified by the Veterans Administration Lung Study Group, (d) received at least four cycles of first-line chemoimmunotherapy with platinum, etoposide, and a PD-1/PD-L1 inhibitor, and (e) did not progress after chemoimmunotherapy. The exclusion criteria were as follows: (a) patients with a second primary tumor, (b) previously received other treatment for the disease, (c) presence of active immune disease requiring long-term immunosuppression, (d) patients who progressed after first-line chemoimmunotherapy, and (e) incomplete treatment records or follow-up data. The decision to administer consolidative TRT was made by the multidisciplinary tumor board based on the following criteria: (1) completion of four to six cycles of first-line chemoimmunotherapy without progression, (2) residual intrathoracic disease amenable to radiotherapy. Patients with extensive extrathoracic progression or deteriorating performance status were not considered candidates for TRT. Eligible patients were divided into two groups: the TRT group, which included patients who received TRT after receiving chemoimmunotherapy, and the non-TRT group, which included patients who received chemoimmunotherapy but not TRT. Prophylactic cranial irradiation was not routinely administered in this cohort. The number of metastatic sites was defined as the count of distinct organ systems involved at diagnosis, as documented on baseline imaging (chest CT, abdominal CT or ultrasound, and brain MRI).
The study was approved by the Ethics Committee of Shandong Cancer Hospital and Institute, the Medical Ethics Committee of Tianjin Cancer Hospital, and the Ethics Committee of Shanghai Chest Hospital.
Treatment
Patients received first-line treatment with a platinum-etoposide chemotherapy regimen in combination with a PD-1/PD-L1 inhibitor (serplulimab, adebrelimab, durvalumab, or atezolizumab), with platinum in the form of either cisplatin (75 mg/m2 on day 1, Q3W) or carboplatin (AUC 5 on day 1, Q3W) and etoposide 100 mg/m2 on days 1–3, Q3W, all intravenously. The chemotherapy portion was administered every 21 days as a treatment cycle for four to six cycles. PD-1/L1 was administered on the first day of each cycle at a dose of 4.5 mg/kg for serplulimab, 20 mg/kg for adebrelimab, 1500 mg for durvalumab, atezolizumab 1200 mg, and maintenance therapy continued until disease progression according to Response Evaluation Criteria for Solid Tumors (RECIST) version 1.1 criteria, an unacceptable toxicity event, withdrawal of informed consent by the patient, or study closure. Among the 240 patients, 98 (40.8%) received cisplatin-based chemotherapy, and 142 (59.2%) received carboplatin-based chemotherapy. The distribution of immunotherapy agents was as follows: serplulimab (n = 90, 37.5%), adebrelimab (n = 68, 28.3%), durvalumab (n = 47, 19.6%), and atezolizumab (n = 35, 14.6%). The proportion of patients receiving each immunotherapy agent was balanced between the TRT and non-TRT groups (p = 0.42).
All patients in the TRT group were treated with either three-dimensional conformal radiation therapy or intensity-modulated radiation therapy for thoracic consolidation. TRT was administered as consolidative therapy for patients who have not progressed after first-line chemoimmunotherapy. Patients received four to six cycles of first-line chemoimmunotherapy, followed by consolidative TRT initiated within 3–6 weeks. Immunotherapy was suspended during radiotherapy and resumed post-treatment, continuing as maintenance therapy until disease progression. Organs at risk (OARs) and target volumes were defined according to the radiotherapy and tumor group guidelines for lung cancer. The Gross tumor volume (GTV) included the residual primary tumor and positive lymph nodes after chemoimmunotherapy; the clinical target volume (CTV) consisted of 5 mm of extravasation of the GTV as well as the drainage area of positive lymph nodes; and the planned target volume (PTV) was 5–8 mm of extravasation of the CTV. Daily image guidance with cone-beam CT was performed prior to each fraction to ensure accurate target localization. The radiotherapy plan was validated to ensure that the radiation dose covered 95% of the PTV. Dose constraints for OARs included: mean lung dose <20 Gy, V20 <35%, mean heart dose <26 Gy, maximum spinal cord dose <45 Gy, and mean esophageal dose <34 Gy.
Given the different dose fractionation regimens of radiotherapy, we used the biological effective dose (BED) formula: BED = nd × [1 + d/(α/β)], where n represents the number of fractions of radiotherapy treatments, d represents the dose per fraction, and α/β = 10. 17 Among the 83 patients who received TRT, the total radiation dose ranged from 25 to 60 Gy. These patients were categorized into three groups based on their dose fractionation regimens: conventional (40–60 Gy in 20–30 fractions of 1.8–2 Gy; BED 44.8–72.0 Gy; n = 48), hypofractionated (35–45 Gy in 10–15 fractions of 2.5–3 Gy; BED 31.25–58.5 Gy; n = 17), and hyperfractionated (30–60 Gy in 20–40 fractions of 1.5 Gy; BED 34.5–69.0 Gy; n = 18).
Endpoints and assessments
The primary study endpoints were patient OS and PFS. PFS was defined as the time from the first day of chemoimmunotherapy to disease progression or death or last follow-up. OS was defined as the time from the first day of chemoimmunotherapy to death from any cause or the last follow-up. To address time bias arising from the delayed initiation of TRT, a landmark analysis was performed with time zero redefined at completion of cycle 4. In this analysis, OS and PFS were measured from cycle 4 completion to event or last follow-up, and TRT was modeled as a time-dependent covariate using Cox regression to account for the change in TRT status at the time of initiation. Secondary study endpoints included OS and PFS in different baseline metastasis subgroups, analysis of adverse events (AEs), survival analysis with different BEDs and different dose fractionation regimens, ORR, defined as the proportion of patients with complete response (CR) and partial response (PR), and disease control rate (DCR), which included patients with CR, PR, and stable disease (SD) lasting for at least 4 weeks. There were no missing data for the primary endpoints (OS and PFS) or baseline characteristics included in the analysis. Follow-up imaging (chest and abdominal CT) was performed every 6–8 weeks during chemoimmunotherapy, and every 8–12 weeks thereafter until disease progression or death. For patients receiving TRT, the first post-treatment response assessment was scheduled 4–6 weeks after TRT completion. The RECIST version 1.1 was used to assess tumor response by local radiologists and treating physicians in our study. 18
Safety assessment
AEs were assessed and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. 19 AEs were captured from the initiation of first-line chemoimmunotherapy until 90 days after the completion of TRT for patients in the TRT group, or until 90 days after the last dose of immunotherapy for patients in the non-TRT group. The analysis focused on the incidence and maximum grade per event for each patient, with a particular focus on pneumonitis and hematologic toxicities.
The overall incidence and severity of AEs were compared between the TRT and non-TRT groups to assess the additional toxicity burden associated with the addition of consolidative TRT. Given the retrospective design and overlapping treatment timelines, definitive attribution of individual AEs to a specific treatment component (chemoimmunotherapy vs TRT) was not feasible; therefore, no attempt was made to assign causality for specific events. These comparisons should be interpreted with caution given the non-randomized design and potential confounding factors.
Statistical analysis
Statistical analyses were performed using SPSS statistical software version 27.0 (IBM Corporation, Armonk, NY, USA) and Prism software version 8.02 (GraphPad, San Diego, CA, USA). Categorical variables were compared using the Chi-square test. Kaplan–Meier curves were constructed and compared using the log-rank test. Univariate and multivariate Cox proportional hazards models were used to estimate HRs and 95% confidence intervals (CIs). The propensity-score matching (PSM) was conducted to adjust the unbalanced confounding baseline factors and minimize the selection bias between the two groups.
To account for guarantee-time bias arising from the delayed initiation of TRT, we performed two complementary analyses: (1) a landmark analysis with time zero reset to cycle 4 completion—the earliest point at which TRT could be initiated after response assessment, and (2) time-dependent Cox models in which TRT was treated as a time-varying covariate. These time-dependent models were also used in univariate and multivariate analyses to evaluate prognostic factors while adjusting for guarantee-time bias. The association between BED and survival was evaluated using Cox models with BED treated as a continuous variable. Restricted cubic spline analysis was performed to explore potential non-linear relationships. An exploratory analysis using receiver operating characteristic (ROC) curves was also performed to identify a potential optimal BED cutoff. However, given the limitations of dichotomizing continuous variables, the results of the restricted cubic spline analysis were considered the primary finding. Survival differences among the three radiotherapy fractionation regimens were assessed using the log-rank test.
All subgroup analyses were pre-specified based on clinically relevant variables (including metastatic sites and number of metastases) but should be considered exploratory. To assess whether the treatment effect of TRT varied across different patient subgroups, we performed interaction tests by introducing an interaction term between treatment allocation (TRT vs non-TRT) and each subgroup variable into the Cox proportional hazards model. Given the multiple comparisons performed, results from subgroup analyses should be interpreted with caution, as the risk of type I error may be inflated. All tests were two-sided, and p < 0.05 was considered statistically significant.
Reporting guidelines
This retrospective cohort study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cohort studies. 20 The completed STROBE checklist is provided as Supplemental File 1.
Results
Patient characteristics
Of the 327 patients initially enrolled after screening, 69 were excluded for various reasons, and 18 were lost to follow-up, a total of 240 elderly patients (⩾70 years) with ES-SCLC receiving first-line chemoimmunotherapy were included in the final analysis. The cohort comprised 83 patients in the TRT group and 157 patients in the non-TRT group (Figure 1). The median age was 73 years. Overall, the ORR and SD rate after initial chemoimmunotherapy were 73.0% and 27.0%, respectively. The ORR was 80% in the TRT group versus 69% in the non-TRT group. There was no significant difference in clinical response to the initial chemoimmunotherapy treatment between the two groups (p = 0.094). All patients were followed up until December 31, 2024, with a median follow-up of 23.02 months (range 21.42–24.61 months). Baseline patient characteristics are summarized in Table 1. Baseline characteristics of patients after PSM are shown in Supplemental Table 1. There was no statistically significant difference in the efficacy of first-line chemoimmunotherapy between the TRT group and the non-TRT group (p = 0.545).

Flowchart of the screening procedure.
Baseline characteristics of the study cohort.

CHD, coronary heart disease; CIT, chemo-immunotherapy; CR, complete response; KPS, Karnofsky performance status; PR, partial response; SD, stable disease; TRT, thoracic radiotherapy.
Efficacy
At the data cutoff, the median follow-up was 23.02 months (range, 21.42–24.61 months). Disease progression occurred in 165 patients (68.7%), and 167 deaths (69.5%) were recorded. For the entire cohort, median OS was 15.97 months (Figure 2(a)), and median PFS was 8.95 months (Figure 2(b)). After resetting the zero-time, median OS was 12.23 months (Figure 2(c)), and median PFS was 5.77 months (Figure 2(d)). The addition of TRT was associated with a significant survival benefit, yielding a median OS of 18.43 versus 14.39 months (HR, 0.64; 95% CI, 0.47–0.87; p = 0.008) and a median PFS of 10.56 versus 8.30 months in the non-TRT group (HR, 0.71; 95% CI, 0.52–0.97; p = 0.034), corresponding to absolute improvements of 4.04 and 2.26 months, respectively (Figure 3(a) and (b)). In the time-dependent Cox analysis with time zero redefined at completion of cycle 4 to account for guarantee-time bias (Figure 3(c) and (d)), the median OS was 14.59 versus 10.92 months (HR, 0.64; 95% CI, 0.46–0.88; p = 0.007), and the median PFS was 7.80 versus 5.12 months (HR, 0.72; 95% CI, 0.52–0.98; p = 0.047), confirming that TRT remained associated with a significant survival benefit.

(a) OS in the entire cohort. (b) PFS for all patients. (c) OS for all patients after redefining time zero. (d) PFS for all patients after redefining time zero.

(a) OS in the TRT group versus the non-TRT group. (b) PFS in the TRT group versus the non-TRT group. (c) OS in the TRT group versus the non-TRT group after redefining time zero. (d) PFS in the TRT group versus the non-TRT group after redefining time zero.
After PSM, survival analysis revealed that the TRT group demonstrated superior OS (18.52 vs 15.77 months; HR, 0.69; 95% CI, 0.47–0.98; p = 0.048) and PFS (10.56 vs 7.51 months; HR, 0.68; 95% CI, 0.47–0.97; p = 0.032). After resetting the time point, the TRT group demonstrated superior OS (14.66 vs 11.93 months; HR, 0.68; 95% CI, 0.46–0.99; p = 0.046) and PFS (7.80 vs 4.46 months; HR, 0.67; 95% CI, 0.46–0.97; p = 0.035; Supplemental Figure 1).
The TRT group also had significantly higher 1- and 2-year PFS rates (36.14% vs 22.23%, p = 0.022; 10.84% vs 4.45%, p = 0.035) and OS rates (72.29% vs 53.50%, p = 0.005; 16.87% vs 8.28%, p = 0.045). Furthermore, the ORR was significantly higher in the TRT group (79.5% vs 58.0%, p = 0.01). Detailed treatment responses are summarized in Table 2.
Treatment response.

Comparison between TRT group and non-TRT group.
CI, confidence interval; TRT, thoracic radiotherapy.
Subgroup survival analysis
Exploratory subgroup analyses based on the number of metastatic sites and metastatic sites were performed, and the results are shown in Figure 4. In the group of patients with ⩽2 metastatic sites, the addition of TRT improved both PFS (10.56 vs 8.40; HR, 0.70; 95% CI, 0.50–0.99; p = 0.039) and OS (18.43 vs 14.66; HR, 0.63; 95% CI, 0.44–0.89; p = 0.008), but this improvement did not occur for the group of patients with >2 metastatic sites (Figure 4(a)). However, the interaction test did not reveal a statistically significant difference in treatment effect between these two subgroups (p for interaction = 0.33). In addition, a significant survival benefit from TRT was observed specifically in patients with the absence of both liver and brain metastases. A total of 143 patients without liver metastases had a prolonged PFS of 3.41 months (14.39 vs 10.98; HR, 0.61; 95% CI, 0.38–0.99; p = 0.044) and a prolonged OS of 3.01 months after receiving TRT (19.71 vs 16.16; HR, 0.57; 95% CI, 0.35–0.93; p = 0.023; Figure 4(b)). The interaction test between the liver metastasis subgroup and the non-liver metastasis subgroup yielded a p-value of 0.15. A total of 187 patients without baseline brain metastases had longer PFS (9.77 vs 7.84; HR, 0.67; 95% CI, 0.46–0.93; p = 0.034) and OS (19.64 vs 14.39; HR, 0.51; 95% CI, 0.34–0.76; p < 0.001; Figure 4(c)). The interaction test between the brain metastasis subgroup and the non-brain metastasis subgroup yielded a p-value of 0.21.

(a) OS and PFS in patients with ⩽2 metastatic sites. (b) OS and PFS in patients without baseline liver metastases. (c) OS and PFS in patients without baseline brain metastases.
After resetting the zero-time, as shown in Figure 5, the clinically significant subgroups demonstrating substantial survival benefit remained the subgroups with ⩽2 metastatic sites, no liver metastases, and no brain metastases. In the subgroup of patients with ⩽2 metastatic sites, TRT was associated with improved median OS (14.66 vs 11.25 months; HR, 0.64; 95% CI, 0.46–0.90; p = 0.009) and PFS (7.74 vs 5.51 months; HR, 0.72; 95% CI, 0.52–0.95; p = 0.048). Among patients without liver metastasis, TRT extended median OS by 3.93 months (HR, 0.60; 95% CI, 0.37–0.97; p = 0.037) and PFS by 4.07 months (HR, 0.60; 95% CI, 0.37–0.97; p = 0.037). Similarly, in the absence of brain metastasis, patients receiving TRT had significantly longer median OS (15.61 vs 10.85 months; HR, 0.66; 95% CI, 0.46–0.93; p < 0.001) and PFS (6.95 vs 4.46 months; HR, 0.72; 95% CI, 0.52–0.99; p = 0.030). The interaction tests for both liver and brain metastasis status were statistically significant (both p for interaction < 0.001). Given the exploratory nature of these analyses and the multiple comparisons performed, these findings should be interpreted with caution.

(a) OS and PFS in patients with ⩽2 metastatic sites after redefining time zero. (b) OS and PFS in patients without baseline liver metastases after redefining time zero. (c) OS and PFS in patients without baseline brain metastases after redefining time zero.
Radiotherapy fractionation and dose analysis
Subgroup analyses were performed based on different radiotherapy fractionation patterns: conventional fractionation, hypofractionation, and hyperfractionation. Survival analysis of the three modes was performed by the log-rank test, and the results revealed that hyperfractionation radiotherapy provided the greatest survival benefit (p = 0.038), as shown in Figure 6(a). After resetting the zero-time, the three fractionation regimens were associated with significantly different survival outcomes (p = 0.048; Figure 6(b)). Pairwise comparison revealed that hyperfractionation conferred a significant survival benefit over conventional fractionation (HR, 2.805; 95% CI, 1.164–6.760; p = 0.022), with median OS of 23.05 versus 13.45 months. No significant difference was observed between hypofractionation and hyperfractionation (HR, 2.077; 95% CI, 0.788–5.478; p = 0.140). Hypofractionation also showed no significant difference compared with conventional fractionation (HR, 1.35; 95% CI, 0.62–2.94; p = 0.267).

(a) Kaplan–Meier graph of OS in patients of different radiotherapy fractionation patterns. (b) Kaplan–Meier graph of OS in patients of different radiotherapy fractionation patterns after redefining time zero.
In an exploratory ROC analysis, a BED cutoff of 52.43 Gy was identified (Supplemental Figure 2). However, when BED was analyzed as a continuous variable using restricted cubic splines (RCS)—a more statistically robust approach—no significant association with OS was observed (overall p = 0.370; p for non-linearity = 0.606), suggesting the absence of a clear dose–response relationship across the range of doses delivered in this study (Figure 7). Given the well-recognized limitations of dichotomizing continuous variables, the results of the RCS analysis are considered the primary finding.

Dose–response relationship between BED and OS.
Analysis of survival predictors
The findings from univariate and multivariate survival analyses (Table 3) indicate that liver metastasis emerged as the sole independent adverse prognostic factor. Patients without liver metastasis had a significantly reduced risk of death (HR, 0.555; 95% CI, 0.402–0.766; p < 0.001). After adjusting for guarantee-time bias (Table 4), liver metastasis remained a significant independent prognostic factor (HR, 0.579; 95% CI, 0.419–0.803; p < 0.001). Notably, brain metastasis was not an independent prognostic factor in the multivariate model (p = 0.293), indicating that the presence of brain metastases did not independently predict worse survival when accounting for other factors. However, interaction tests revealed important differences in treatment effect. The forest plot (Figure 8) illustrates the consistency of the TRT benefit across clinically relevant subgroups in the original analysis, with interaction tests showing no significant heterogeneity by sex, KPS, smoking status, or comorbidities (all p for interaction > 0.05). After resetting time zero to address guarantee-time bias (Figure 9), significant interactions emerged for both liver and brain metastasis status (both p for interaction < 0.001).
Univariate and multivariable analyses for OS.
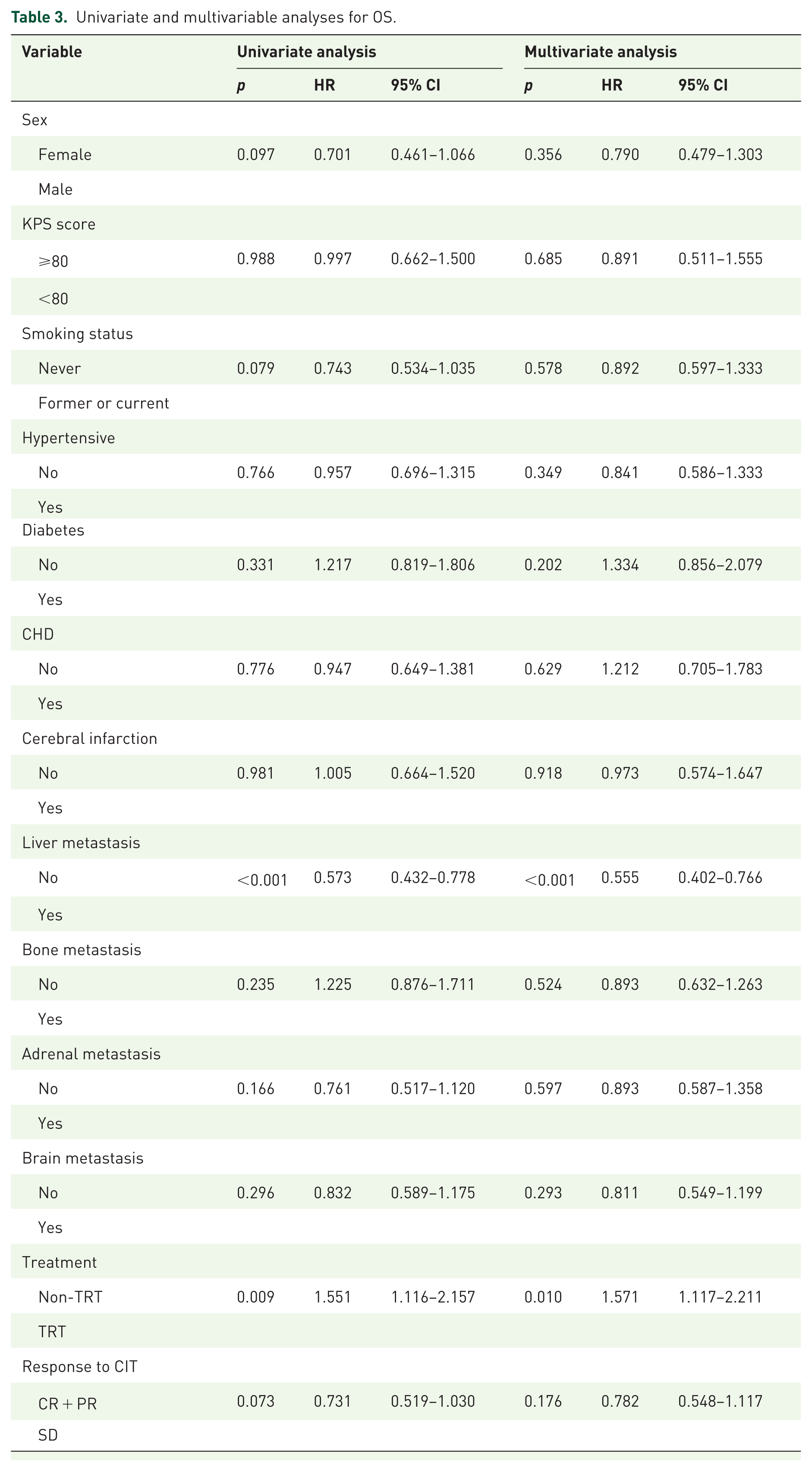
CHD, coronary heart disease; CI, confidence interval; CIT, chemo-immunotherapy; CR, complete response; HR, hazard ratio; KPS, Karnofsky Performance Status; OS, overall survival; PR, partial response; SD, stable disease; TRT, thoracic radiotherapy.
Univariate and multivariable analyses for OS after adjusting for bias.

CHD, coronary heart disease; CI, confidence interval; CIT, chemo-immunotherapy; CR, complete response; HR, hazard ratio; KPS, Karnofsky Performance Status; OS, overall survival; PR, partial response; SD, stable disease; TRT, thoracic radiotherapy.

Forest plot of subgroup analysis of OS.

Forest plot of subgroup analysis of OS after redefining time zero.
In the subgroup of patients with liver metastasis, TRT was associated with a numerical improvement in median OS of approximately 4 months (HR, 0.71; 95% CI, 0.45–1.13), although this did not reach statistical significance. Notably, even among those who received TRT, patients with liver metastasis had a shorter median OS (14.0 months) compared with patients without liver metastasis who did not receive TRT (16.16 months), underscoring the poor prognosis associated with liver involvement. These findings remained consistent after redefining time zero.
Safety
Table 5 shows the toxicity reactions in the TRT and non-TRT groups. Most of the adverse reactions were tolerable, self-limiting, and easy to manage and did not affect the patient’s treatment. Anemia was the most common adverse reaction, with 179 cases (74.5%), and leukopenia was the second most common, with 162 cases (67.5%). For any grade of adverse reactions, patients who received TRT had significant leukopenia (80.7% vs 60.5%, p < 0.001) and anemia (83.1% vs 70.0%, p = 0.027) compared with the non-TRT group, but for grade ⩾3 adverse reactions, there was no significant difference between the two groups. For treatment-related pneumonia, there were 15 cases (18.67%) in the TRT group and 17 cases (10.83%) in the non-TRT group, with no statistically significant difference between the two groups (p = 0.166).
Adverse events.

TRT, thoracic radiotherapy.
Discussion
Radiotherapy is a highly effective tumor-directed therapy, with approximately 60% of newly diagnosed cancer patients receiving RT as a first-line treatment. 21 Early clinical evidence suggests that radiotherapy can elicit significant responses not only at the treatment site but also at distant, unexposed tumor deposits—the so-called “abscopal effect.” 22 Moreover, ionizing radiation can work together with immune checkpoint blockade to enhance immune-mediated tumor recognition and rejection.23,24 When combined with immunotherapy, radiotherapy enhances T-cell trafficking to locally treated tumor sites and augments preexisting anticancer T-cell responses. 25 Moreover, preclinical studies have demonstrated that radiotherapy can enhance tumor immunogenicity by upregulating the expression of tumor-associated antigens on the cell surface, thereby promoting the opsonization of tumor cells by specific antibodies. 26 Several previous clinical studies have demonstrated the survival benefits of radiotherapy in combination with ICI.24,27,28
The IMpower133, CASPIAN, and CAPSTONE-1 trials represent breakthrough advances in ES-SCLC treatment, establishing chemotherapy combined with immunotherapy as the standard first-line therapy.6 –8 However, the role of consolidative TRT in the modern chemoimmunotherapy era for ES-SCLC has not been definitively established, particularly in elderly patients who are underrepresented in clinical trials.
The efficacy of TRT has been substantiated by robust evidence demonstrating survival benefits in NSCLC. In the PACIFIC trial, compared with placebo, the addition of durvalumab to concurrent chemoradiotherapy significantly prolonged OS in patients with stage III unresectable NSCLC. 29 The 5-year follow-up data revealed that the median OS was 47.5 vs 29.1 months (HR, 0.72; 95% CI, 0.59–0.89), and the median PFS was 16.9 vs 5.6 months (HR, 0.55; 95% CI, 0.45–0.68) in the durvalumab group and the placebo group, respectively. The 5-year OS rates were 42.9% and 33.4%, respectively, and the 5-year PFS rates were 33.1% and 19.0%, respectively. 30 Similarly, the Pembro-RT trial demonstrated that compared with pembrolizumab alone, stereotactic body radiotherapy (SBRT) followed by pembrolizumab resulted in a doubled ORR and prolonged PFS and OS. 31 The results of the present study were similar to those of these two clinical trials, demonstrating that consolidation TRT after first-line chemoimmunotherapy prolonged OS and PFS in elderly ES-SCLC patients, providing a significant survival benefit. The ASTRO guideline on radiation therapy for ES-SCLC recommends TRT for ES-SCLC patients who respond to chemotherapy and immunotherapy. 32
In terms of ES-SCLC, Jeremic et al. 33 first reported that compared with chemotherapy alone, the introduction of chest radiotherapy to chemotherapy resulted in a higher survival rate (mOS, 17 vs 11 months, p = 0.041). In 2015, a phase III randomized CREST trial enrolled ES-SCLC patients who responded to initial ChT and randomly assigned them to receive either TRT or no TRT. Two-year OS (13% vs 3%, p = 0.004) and mPFS (4 vs 3 months, p = 0.001) significantly improved with TRT. 34 A 2025 systematic review and meta-analysis encompassing 20 studies and 5282 patients represents the most robust evidence to date regarding consolidative TRT, confirming significant OS (HR, 0.57; 95% CI, 0.48–0.66) and PFS (HR, 0.53; 95% CI, 0.45–0.63) in ES-SCLC. Notably, that analysis demonstrated that patients with baseline brain metastases still derived a clear survival benefit (OS: HR, 0.57; 95% CI, 0.39–0.84), whereas those with liver metastases showed no significant improvement. 35 In contrast, our subgroup analysis in elderly patients (⩾70 years) revealed that those with brain metastases did not derive significant benefit from consolidative TRT (OS: HR, 1.14; 95% CI, 0.78–2.67; p = 0.50), while the lack of benefit in patients with liver metastases was consistent with the meta-analysis findings. This discrepancy may reflect the unique characteristics of the elderly population, including differences in tumor biology, treatment tolerance, or competing risks of mortality. These findings highlight the importance of age-specific considerations when applying evidence from mixed-age populations to elderly patients and underscore the need for further research in this underrepresented group.
Meanwhile, several retrospective studies have focused on evaluating the impact of adding TRT to first-line chemotherapy-immunotherapy regimens for ES-SCLC. A multicenter retrospective analysis by Cai et al. 36 confirmed that consolidation TRT combined with chemotherapy-immunotherapy is safe and effective. Yao et al.’s 37 propensity score-matched study indicated that adding TRT significantly improved OS (21.67 vs 16.60; p = 0.009) and PFS (10.76 vs 7.63; p = 0.014). A phase II clinical trial also demonstrated that first-line adebrelimab plus chemotherapy and TRT significantly benefited patients with ES-SCLC, with a mOS of 22.9 months (an increase of 9.5 months) and a mPFS of 11.3 months (an increase of 7.2 months). The median age of enrolled patients was 57.66 years, with 63% under 65 years old. 16
Notably, the survival outcomes observed in our elderly cohort (mOS 18.43 months with TRT from the start of first-line chemoimmunotherapy) are comparable to those reported in younger populations. For instance, Chen et al. 16 reported a mOS of 22.9 months in a phase II trial with a median age of 57.7 years, and Yao et al. 37 observed a mOS of 21.67 months in a propensity-matched analysis including patients with a median age of 62 years. These comparisons suggest that advanced age alone should not preclude consideration of consolidative TRT, and that elderly patients can derive clinically meaningful survival benefits comparable to their younger counterparts.
To our knowledge, this multicenter study is the first to specifically evaluate the efficacy and safety of consolidative TRT following first-line chemoimmunotherapy in a purely elderly ES-SCLC cohort (⩾70 years). Results indicate that the addition of consolidative TRT is associated with significantly improved survival in this clinically important and underrepresented population, prolonging OS and PFS by 4.04 and 2.3 months, respectively.
However, the combination of chemoimmunotherapy and chest radiotherapy remains a prudent option. Pneumonia is a particularly worrisome complication of immunotherapy and a recognized sequela of chest radiotherapy.38,39 Radiotherapy produces reactive oxygen species, which cause cellular damage and initiate an inflammatory cascade. An excessive localized response to this process can lead to radiological lung injury.40,41 The safety profile for combining TRT with chemoimmunotherapy was established in the PACIFIC study, which observed no statistically significant increase in pneumonitis risk (33.9% vs 24.8%) for patients with NSCLC. 30 In this study, the incidence of pneumonitis was comparable between groups (18.7% vs 10.8%, p = 0.116), with no significant increase in risk attributable to TRT. The incidence of grade 3 or higher pneumonia was 6.0% and 3.9%, respectively. There was no significant difference between the two control groups (p = 0.438).
Notably, further discussion is needed regarding the optimal therapeutic dose and treatment modality. Clinical data on the combination of radiotherapy and immunotherapy in ES-SCLC are limited, and the optimal TRT dose is still debated. In a retrospective study, high-dose (tBED >50 Gy) TRT treatment and low-dose (tBED ⩽50 Gy) TRT treatment were given after ChT. The 2-year OS, PFS, and LC rates were 32.3%, 15.3%, and 47.1%, respectively, for high-dose radiotherapy and 17.0% (p < 0.001), 12.9% (p = 0.097), and 34.7% (p = 0.029), respectively, for low-dose radiotherapy. 42 These findings demonstrate that high-dose TRT is superior to low-dose TRT for improving OS. Conversely, Han et al. 17 found that while radiation dose did not significantly affect survival outcomes in the entire study population, a significant benefit for low-dose radiotherapy was observed in patients who were CR/PR to systemic therapy, evidenced by improved median OS (27.1 vs 22.7 months, p = 0.026) and PFS (11.4 vs 11.2 months, p = 0.032). In this study, the ROC curve was plotted to determine the relationship between the radiotherapy dose and survival, with a cutoff value of 52.43 Gy, and patients were categorized into low-dose (BED ⩽52.43 Gy) and high-dose (BED > 52.43 Gy) groups on the basis of the predetermined cutoff value according to the ROC curve. Compared with patients in the high-dose group, patients in the low-dose group had significantly better survival (mOS, 22.59 vs 16.36; p = 0.026), with a prolonged mPFS of 3.91 months, although the difference was not statistically significant (p = 0.19). Therefore, researchers still need to explore the optimal dose for radiotherapy further. Although our exploratory ROC analysis suggested superior efficacy below 52.43 Gy, this finding should be interpreted with caution due to the inherent limitations of dichotomizing continuous variables. A more rigorous restrictive cubic spline analysis failed to confirm a significant dose–response relationship (p = 0.370). Our study cohort comprised exclusively elderly patients (⩾70 years), who may exhibit distinct tumor biology, immune function, and treatment tolerance compared to younger populations, potentially altering dose–response relationships. Moreover, the relatively narrow BED range (31.25–72.0 Gy) and sample size (n = 83) may have limited statistical power to detect subtle dose–response effects. These findings underscore the need for larger prospective studies to definitively determine the optimal radiotherapy dose for this population.
With respect to radiotherapy modalities, Luan et al. 43 reported that compared with 60 Gy/30f, 45 Gy/30f had a better survival advantage (mPFS, 11 vs 9; p = 0.043). Similarly, we found that hyperfractionation radiotherapy was the most effective treatment (p = 0.038). After redefining the baseline time point and adopting time-dependent Cox analysis, hyperfractionated radiotherapy still demonstrated therapeutic advantages (p = 0.048). Furthermore, pairwise comparisons revealed that hyperfractionation significantly improved patient survival compared to conventional fractionation (HR, 2.805; 95% CI, 1.164–6.760; p = 0.022), with a mOS extension of 9.6 months. Although hypofractionation showed a trend toward poorer outcomes compared with hyperfractionation (HR, 2.077; 95% CI, 0.788–5.478; p = 0.140), this difference did not reach statistical significance, likely due to the relatively small sample size in this group (n = 17). Furthermore, no significant difference was observed between hypofractionation and conventional fractionation (p = 0.267). These findings suggest that hyperfractionated therapy may be the preferred option when clinically feasible, while hypofractionation represents a reasonable alternative, particularly given its shorter treatment duration and comparable efficacy to conventional fractionation. Larger prospective studies are still needed to explore the optimal radiotherapy regimen for elderly patients with ES-SCLC.
After resetting the time point to zero, interaction tests revealed that both liver and brain metastasis status significantly modified the therapeutic effect of TRT (p values for both interactions < 0.001). These findings indicate that the benefit of consolidation TRT is not uniform across all patients but critically depends on the location of metastatic disease. Notably, while brain metastases were not an independent prognostic factor in multivariate analysis (p = 0.293), they emerged as a significant treatment effect modifier: patients without brain metastases derived substantial benefit from TRT, whereas those with brain metastases did not. This distinction holds important clinical implications: even if brain metastases cannot independently predict OS, their presence should guide patient selection for consolidation TRT. Our finding that patients with brain metastases failed to benefit from TRT (HR, 1.48; 95% CI, 0.80–2.73) contrasts with a recent meta-analysis suggesting significant survival benefit for those with brain metastases (OS: HR, 0.57; 95% CI, 0.39–0.84; p = 0.01; PFS: HR, 0.42; 95% CI, 0.28–0.64; p < 0.001). 35 This discrepancy reflects the unique characteristics of elderly cohorts, including differences in tumor biology and treatment tolerance. Older patients may exhibit altered immune function and vascular permeability, thereby modifying their response to radiotherapy-immunotherapy combinations. These observations underscore the importance of age-specific considerations in geriatric populations and the necessity for studies specifically designed for the elderly.
Regarding metastatic burden, patients with ⩽2 metastatic sites derived significant benefit from TRT, whereas those with >2 metastatic sites did not. Xu et al. 44 reported that patients with oligometastatic ES-SCLC could benefit more in terms of OS, PFS, and local control with the addition of TRT. A secondary analysis of the CREST revealed that patients with no liver metastases or those with only zero to two distant metastases had significantly longer PFS (p = 0.001 and p = 0.003, respectively). 45 Zhang et al. 46 reported that TRT improved PFS and OS in patients with oligometastatic ES-SCLC and in patients without brain or liver involvement. Consistent with our findings, patients with lower tumor burden (0–2 distant metastases, particularly those without liver or brain metastases) were more likely to benefit from combined TRT. However, the interaction test for number of metastatic sites did not reach statistical significance (p = 0.33; p = 0.21 after reset time), suggesting treatment response may be influenced more by specific metastatic sites than absolute number.
In contrast, liver metastases acted as both a treatment effect modifier and an independent poor prognostic factor. Our multivariate analysis identified liver metastases as the sole independent poor prognostic factor (p < 0.001). A retrospective analysis of 118 patients with ES-SCLC who received first-line chemoimmunotherapy (45 of whom received TRT) demonstrated that liver metastases were an independent predictor of OS in multivariate analysis, suggesting that patients with liver metastases may not benefit from consolidative TRT. 14 Dominik’s systematic review and meta-analysis also indicated that patients with baseline liver metastases receiving combined chemo-immunotherapy showed no significant survival improvement after consolidation TRT (OS: HR, 0.90; 95% CI, 0.61–1.32; PFS: HR, 0.59; 95% CI, 0.17–2.01). 35 This landmark research underscores the efficacy of cTRT and validates the profound impact of different baseline metastatic patterns on prognosis—particularly the adverse prognostic effect associated with liver metastases. This finding is comparable to our findings.
In summary, these findings support individualized treatment decisions for consolidation TRT based on metastatic patterns, with particular attention to the presence of liver or brain metastases. Future prospective studies should stratify patients according to metastatic sites and burden to validate these observations and further refine treatment recommendations for elderly ES-SCLC patients.
The limitations of this study include those inherent to its retrospective, real-world design. The potential for selection bias exists, as consolidation TRT was likely offered to patients with better performance status. To address guarantee-time bias arising from the delayed initiation of TRT, we performed landmark analyses and time-dependent Cox models with time zero redefined at cycle 4 completion, as described in the “Methods and patients.” Furthermore, heterogeneity in treatment administration (e.g., doses and cycles) must be acknowledged. While we sought to mitigate these issues via a multicenter design and multivariate analysis, further validation through large-scale, prospective trials is warranted to confirm our conclusions.
Conclusion
In conclusion, the addition of TRT in elderly ES-SCLC patients receiving first-line platinum-based chemotherapy in combination with immunotherapy resulted in significant survival benefits and tolerability. The results suggest that TRT plus chemoimmunotherapy may be a first-line therapeutic strategy for elderly ES-SCLC patients, but further studies are needed to confirm this conclusion.
Supplemental Material
sj-docx-2-tam-10.1177_17588359261444162 – Supplemental material for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study
Supplemental material, sj-docx-2-tam-10.1177_17588359261444162 for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study by Ke Zhao, Qinhao Xu, Xuwei Cai, Lujun Zhao, Weikang Xin, Wanjing Li, Yaru Tian, Yulan Sun and Hui Zhu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-4-tam-10.1177_17588359261444162 – Supplemental material for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study
Supplemental material, sj-docx-4-tam-10.1177_17588359261444162 for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study by Ke Zhao, Qinhao Xu, Xuwei Cai, Lujun Zhao, Weikang Xin, Wanjing Li, Yaru Tian, Yulan Sun and Hui Zhu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-1-tam-10.1177_17588359261444162 – Supplemental material for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study
Supplemental material, sj-jpg-1-tam-10.1177_17588359261444162 for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study by Ke Zhao, Qinhao Xu, Xuwei Cai, Lujun Zhao, Weikang Xin, Wanjing Li, Yaru Tian, Yulan Sun and Hui Zhu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-jpg-3-tam-10.1177_17588359261444162 – Supplemental material for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study
Supplemental material, sj-jpg-3-tam-10.1177_17588359261444162 for Consolidation thoracic radiotherapy after chemoimmunotherapy provides survival benefit in elderly patients with extensive-stage small-cell lung cancer: a multicenter study by Ke Zhao, Qinhao Xu, Xuwei Cai, Lujun Zhao, Weikang Xin, Wanjing Li, Yaru Tian, Yulan Sun and Hui Zhu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.