
Abstract
Background:
Taxane–carboplatin-based neoadjuvant chemotherapy (NAC) improves the pathological complete response (pCR) rate in human epidermal growth factor receptor 2 (HER2)-negative breast cancer. However, its effect on long-term survival remains unclear. Reliable prognostic biomarkers are needed to guide personalized postoperative strategies.
Objectives:
To evaluate the prognostic significance of the platelet-to-lymphocyte ratio (PLR) and to construct a predictive model for overall survival (OS) in this clinical setting.
Design:
This was a retrospective, multicenter cohort study involving an internal development cohort and an external validation cohort.
Methods:
We retrospectively analyzed 178 HER2-negative breast cancer patients treated with taxane–carboplatin NAC at Fudan University Shanghai Cancer Center (FUSCC). The optimal PLR cutoff (129.75) was identified via receiver operating characteristic (ROC) analysis. Logistic regression assessed the association between PLR and pCR, and multivariate Cox regression evaluated its prognostic value for OS. A nomogram incorporating PLR, estrogen receptor (ER) status, and clinical stage was built using the FUSCC cohort. The nomogram was externally validated in 34 patients from Fujian Cancer Hospital.
Results:
Among the 178 patients, 94 (52.8%) had high PLR and 84 (47.2%) had low PLR. High PLR was not independently associated with pCR (odds ratio = 1.006; 95% confidence interval (CI): 0.999–1.013; p = 0.079). However, in non-pCR patients, high PLR was significantly linked to poorer OS (p = 0.001). Multivariate analysis identified high PLR (hazard ratio = 5.718; 95% CI: 1.664–19.646; p = 0.006), clinical stage III disease, and ER positivity as independent OS predictors. The nomogram integrating these factors demonstrated strong predictive performance in both cohorts.
Conclusion:
This is the first study to evaluate PLR as a prognostic marker in HER2-negative breast cancer treated with taxane–carboplatin NAC. High PLR was independently associated with poorer survival. The proposed nomogram provides a practical tool for postoperative risk stratification and personalized care.
Plain language summary
Keywords
Introduction
Breast cancer is a leading malignancy affecting women globally. 1 Human epidermal growth factor receptor 2 (HER2)-negative breast cancer, comprising triple-negative breast cancer (TNBC) and hormone receptor-positive/HER2-negative (HR+/HER2−) breast cancer, accounts for nearly 85% of all breast cancer cases.2 –4 Neoadjuvant chemotherapy (NAC) is widely applied in HER2-negative breast cancer treatment; however, its efficacy varies. HR+/HER2− breast cancer patients generally have low chemotherapy response rates, with pathological complete response (pCR) ranging from 5% to 10%.5,6 Patients with TNBC can achieve a pCR rate of 30%–40%; however, those who do not attain pCR have a 5-year overall survival (OS) rate of <50%. 7 Reliable biomarkers are thus needed to optimize personalized treatment, refine NAC prediction, and guide postoperative management in patients with HER2-negative breast cancer.
The taxane–carboplatin combination, a non-anthracycline chemotherapy regimen, has recently gained popularity for neoadjuvant treatment of HER2-negative breast cancer due to its reduced cardiotoxicity and favorable tolerability profile.8 –10 Taxanes inhibit microtubule depolymerization, consequently disrupting tumor cell division,11,12 while carboplatin induces DNA crosslinking to enhance antitumor activity. 13 Studies have shown the efficacy of this regimen in increasing pCR rates. The GeparSixto 9 and CALGB40603 14 trials reported that adding carboplatin to standard chemotherapy markedly elevated pCR rates in patients with TNBC. The BrighTNess trial 15 confirmed that paclitaxel combined with carboplatin led to superior pCR outcomes compared to paclitaxel alone. Similarly, the NeoCART study 16 revealed that docetaxel combined with carboplatin resulted in higher pCR rates in TNBC than epirubicin and cyclophosphamide. Furthermore, the FINEST trial 17 in HR+/HER2− breast cancer noted a 21.1% pCR rate in the chemotherapy-sensitive group, suggesting potential clinical benefit in specific subgroups.
The taxane plus carboplatin regimen has been widely used in treating TNBC and has demonstrated promising applicability in HR+/HER2− patients, thereby becoming a key component of NAC for HER2-negative breast cancer. Despite these encouraging findings in terms of pCR improvement, whether the taxane plus carboplatin regimen results in better long-term survival outcomes remains unclear. Therefore, identifying biomarkers that can predict both pCR and OS is essential for making more precise treatment decisions.
Platelets facilitate tumor proliferation, angiogenesis, and immune escape in the tumor microenvironment.18,19 Meanwhile, lymphocytes are pivotal in antitumor immunity. 20 Several studies have indicated a consistent link between elevated platelet-to-lymphocyte ratio (PLR) and both OS and disease-free survival.21,22 However, the prognostic significance of PLR in the context of NAC for HER2-negative breast cancer, particularly with specific chemotherapy regimens, is yet to be fully confirmed.
Therefore, this study evaluated baseline PLR as a predictor of pCR and OS in patients with HER2-negative breast cancer treated with taxane–carboplatin NAC. We also explored potential biomarkers for personalized therapy and examined the clinical implications of this regimen.
Materials and methods
Patient selection
This retrospective study included patients with HER2-negative breast cancer who received taxane–carboplatin-based NAC followed by surgery at Fudan University Shanghai Cancer Center (FUSCC) between January 2010 and December 2019. Clinical data were extracted from medical records, including age, menopausal status, and clinicopathological characteristics: estrogen receptor (ER), progesterone receptor (PR), HER2, Ki-67 index, clinical T and N stages, pCR, and PLR. PLR was calculated using peripheral blood counts obtained within 1 week prior to NAC initiation. Clinical staging was determined according to the 8th edition of the American Joint Committee on Cancer (AJCC) staging system.
The inclusion criteria were as follows: (1) ultrasound-guided core needle biopsy before NAC, (2) pathologically confirmed HER2-negative breast cancer, (3) complete baseline laboratory data, (4) taxane–carboplatin-based NAC followed by surgery, and (5) comprehensive follow-up and clinicopathological data.
The exclusion criteria were as follows: (1) bilateral or inflammatory breast cancer, (2) male breast cancer, (3) neoadjuvant endocrine therapy only, (4) NAC completed without surgery, (5) postoperative HER2-positive pathology, (6) presence of acute or chronic inflammatory diseases, identified either by clinical records (such as active infections or autoimmune diseases) or by abnormal laboratory indicators (including elevated C-reactive protein (>10 mg/L) and/or abnormal white blood cell (WBC) counts (WBC >10 × 10⁹/L or <4 × 10⁹/L)), all assessed within 1 week prior to the initiation of NAC, (7) history of other malignancies, and (8) use of medications that could significantly affect peripheral blood cell counts (such as systemic corticosteroids or granulocyte colony-stimulating factor), within 1 week prior to the initiation of NAC.
A total of 178 patients were included and categorized into the training and validation sets (7:3 ratio) to develop the prediction model. Thirty-four patients with HER2-negative breast cancer treated with taxane–carboplatin-based NAC and surgery at Fujian Cancer Hospital between 2019 and 2024 formed the external validation group. Figure 1 shows the study design and patient selection process. Ethics approval was obtained from both FUSCC (approval number: 050432-4-1911D) and Fujian Cancer Hospital (approval number: K2024-469-01), with data confidentiality maintained.

Flow chart.
Pathology
Immunohistochemistry (IHC) was performed on core needle biopsy and resected tumor specimens using formalin-fixed, paraffin-embedded sections. ER, PR, HER2, and Ki-67 expression were assessed. ER and PR positivity were defined as ⩾1% nuclear staining or Allred scores 2–8, and negativity with a score of 0. 23 HER2 status was classified per the American Society of Clinical Oncology/College of American Pathologists guidelines: 3+ as positive and 0/1+ as negative. Tumors scored 2+ underwent fluorescent in situ hybridization using PathVysion (Vysis, IL, USA) or HER2 inform (Ventana) (Roche Diagnostics, Tucson, AZ, USA).24,25 HER2-negative IHC 0 expression was categorized as HER2-0 expression, and HER2-negative IHC + or ++ expression was classified as HER2-low expression. 26 Ki-67 values of ⩽20% and >20% were considered low and high expressions, respectively. 27
Study endpoints
The primary endpoint was OS, defined as the time from diagnosis to death from any cause. The secondary endpoint, pCR, was defined as the absence of residual invasive cancer in the breast and lymph nodes, with possible ductal carcinoma in situ in the breast.28,29 Cases that failed to meet this criterion, such as those with partial response or non-response, were categorized as the “non-pCR” group.
Statistical analysis
Categorical variables are expressed as frequencies and percentages. The optimal PLR cutoff was identified using receiver operating characteristic (ROC) curve analysis to maximize sensitivity and specificity for survival prediction. Binary logistic regression was employed to assess pCR predictors. Survival curves were generated using the Kaplan–Meier method and compared via the log-rank test. Variables with p < 0.05 in univariate Cox analysis were included in the multivariate model, with hazard ratios (HRs) and 95% confidence intervals (CIs) calculated. Patients were randomly assigned to the training and validation sets (7:3 ratio) using the “create Data Partition” function in R software (R Foundation for Statistical Computing, Vienna, Austria), ensuring balanced event distribution. The training set was used for model development, and the validation sets were used to assess the model’s performance. The final model, integrating PLR and independent clinicopathological factors, was presented as a nomogram. Discriminatory ability was evaluated using the concordance index (C-index) and the area under the ROC curve (AUC). Calibration was assessed using a calibration curve. All statistical analyses were performed using R software (version 4.1.3). Statistical significance was set at p < 0.05.
Reporting guideline compliance
The reporting of this study conforms to the TRIPOD-AI statement 30 (see Supplemental File).
Results
Patient characteristics
A total of 178 eligible patients were enrolled, with a median age of 50 (range, 39–61) years. The ROC curve analysis identified 129.75 as the optimal PLR cutoff for OS prediction, with an AUC of 0.749 (Supplemental Figure 1). Based on this threshold, 84 (47.2%) and 94 (52.8%) patients were classified as low-PLR (PLR <129.75) and high-PLR (PLR ⩾129.75), respectively.
Baseline characteristics were comparable between the two groups (Table 1). Among the total population, over three-fifths of patients were postmenopausal. The diagnosis for all patients was invasive ductal carcinoma, with 55.06% and 53.37% being ER-positive and PR-positive, respectively, and 90.45% having lymph node metastases. HER2 negativity was observed in all patients, with 92 (51.69%) showing HER2-low expression.
Baseline characteristics of the study population.

ER, estrogen receptor; HER2, human-epidermal growth factor receptor 2; HR+/HER2−, hormone receptor-positive/HER2-negative; pCR, pathological complete response; PLR, platelet-to-Lymphocyte Ratio; PR, progesterone receptor; TNBC, triple-negative breast cancer.
A total of 107 patients (60.11%) had HR+/HER2− breast cancer, while 71 (39.89%) were diagnosed with TNBC. PLR distribution was similar between the two groups. According to the AJCC 8th edition TNM classification, all patients had stages II–III disease. Postoperatively, a pCR was achieved in 37 (20.79%) patients.
Relationship between PLR and pCR
Among all participants, pCR was achieved by 15 (17.86%) and 22 (23.40%) patients in the low PLR (n = 84) and high PLR (n = 94) groups, respectively, with no significant difference (p = 0.363; Table 1). Univariate logistic regression analysis revealed no association between PLR and pCR (odds ratio (OR) = 1.406, 95% CI: 0.674–2.930, p = 0.364; Table 2). Similarly, multivariate logistic regression analysis showed that PLR was not an independent predictor of pCR (OR = 1.006, 95% CI: 0.999–1.013, p = 0.079). However, tumor grade, Ki-67 levels, and clinical stage emerged as independent predictors of pCR. Grade III tumors were more likely to achieve pCR (OR = 2.773, 95% CI: 1.147–6.705, p = 0.024). Ki-67 >20% significantly increased the likelihood of pCR compared to Ki-67 ⩽20% (OR = 16.403, 95% CI: 2.114–127.284, p = 0.007). Clinical stage III disease was less likely to achieve pCR than clinical stage II (OR = 0.239, 95% CI: 0.144–0.655, p = 0.001).
Multivariate model of factors predicting pCR among all patients.

CIs, confidence intervals; ER, estrogen receptor; HER2, human-epidermal growth factor receptor 2; HR+/HER2−, hormone receptor-positive/HER2-negative; OR, odds ratio; pCR, pathological complete response; PLR, platelet-to-lymphocyte ratio; PR, progesterone receptor; TNBC, triple-negative breast cancer.
Among the 107 patients with HR+/HER2− breast cancer, 11 (10.28%) achieved pCR. Five (9.62%) and six (10.91%) patients achieved pCR in the low-PLR (n = 52) and high-PLR (n = 55) groups, respectively, with no significant difference (p = 0.826; Supplemental Table 1). Univariate logistic regression analysis did not reveal a significant correlation between PLR and pCR (OR = 1.151, 95% CI: 0.329–4.027; p = 0.826). Subsequent analysis indicated that tumor grade and clinical stage were correlated with pCR (Supplemental Table 3). PLR remained insignificant in the multivariate regression analysis, whereas tumor grade and clinical stage remained independent predictors of pCR.
Of the 71 patients with TNBC, 26 (36.62%) achieved pCR. Ten (31.25%) and 16 (41.02%) patients achieved pCR in the low-PLR (n = 32) and high-PLR (n = 39) groups, respectively, with no significant difference (p = 0.395; Supplemental Table 2). Univariate logistic regression revealed no significant link between PLR and pCR (OR = 1.530, 95% CI: 0.573–4.089; p = 0.396; Supplemental Table 4). Likewise, no other clinicopathological factors showed a significant correlation with pCR.
Survival outcomes based on PLR
Due to the low incidence of outcome events (<50%), it was not possible to estimate the median survival time. During follow-up, patients with low PLR had significantly longer survival time than those with high PLR (p < 0.001; Figure 2). The5-year OS rate was 95.53% (95% CI: 89.54%–100%) and 69.31% (95% CI: 57.73%–83.22%) in the low-PLR and high-PLR groups, respectively.

KM curves for OS stratified by baseline PLR (all patients).
Univariate and multivariate Cox analyses revealed PLR to be significantly associated with OS. In univariate Cox analysis, PLR, ER status, clinical stage, and tumor grade were linked to OS, with high PLR being a negative prognostic factor (HR = 6.328, 95% CI: 1.862–21.509, p = 0.003). After adjusting for significant variables, high PLR remained an independent predictor of poor OS (HR = 5.718, 95% CI: 1.664–19.646, p = 0.006). ER positivity (HR = 0.349, 95% CI: 0.143–0.853, p = 0.021) and clinical stage III disease (HR = 4.922, 95% CI: 1.140–21.251, p = 0.033) also emerged as independent prognostic factors (Table 3).
Univariate and multivariate Cox regression model analyses of prognostic factors of OS among all patients.

CIs, confidence intervals; ER, estrogen receptor; HER2, human-epidermal growth factor receptor 2; HRs, hazard ratios; HR+/HER2−, hormone receptor-positive/HER2-negative; OR, odds ratio; OS, overall survival; pCR, pathological complete response; PLR, platelet-to-lymphocyte ratio; PR, progesterone receptor; TNBC, triple-negative breast cancer.
Survival outcomes stratified by PLR and pCR
Among patients who achieved pCR, survival was similar between the high-PLR and low-PLR groups (p = 0.221; Supplemental Figure 2(A)). Conversely, in the non-pCR subgroup, patients with a high PLR experienced significantly poorer survival than those with a low PLR (p = 0.001; Supplemental Figure 2(B)).
Construction and validation of the prognostic nomogram
Data from FUSCC were classified into the training (n = 124) and internal validation (n = 54) sets, whereas 34 HER2-negative patients from Fujian Cancer Hospital formed the external validation cohort. Baseline characteristics of the three cohorts are presented in Table 4. With a PLR cutoff of 129.75, high PLR was observed in 52.42%, 53.7%, and 55.88% of the training, internal validation, and external validation sets, respectively.
Baseline characteristics of the study population (training cohort, internal validation cohort, and external validation cohort).

ER, estrogen receptor; HER2, human-epidermal growth factor receptor 2; HR+/HER2−, hormone receptor-positive/HER2-negative; pCR, pathological complete response; PLR, platelet-to-lymphocyte ratio; PR, progesterone receptor; TNBC, triple-negative breast cancer.
As shown in Table 5, univariate analysis identified high PLR (HR = 12.843, p = 0.014), ER positivity (HR = 0.308, p = 0.039), clinical stage III (HR = 8.278, p = 0.042), and grade III (HR = 3.649, p = 0.022) as OS predictors. These variables were further assessed in a stepwise multivariate model, where high PLR (HR = 15.163, p = 0.011), ER positivity (HR = 0.248, p = 0.018), and clinical stage III (HR = 7.929, p = 0.049) remained significant predictors.
Univariate and multivariate Cox regression model analyses of prognostic factors of OS among the training cohort.

CIs, confidence intervals; ER, estrogen receptor; HER2, human-epidermal growth factor receptor 2; HR, hazard ratio; OS, overall survival; pCR, pathological complete response; PLR, platelet-to-lymphocyte ratio; PR, progesterone receptor.
A prognostic nomogram was created by including these independent variables (Figure 3). The nomogram assigns a particular score to each factor (PLR level, ER status, and clinical stage) and calculates a total score to forecast personalized survival probability following NAC. Within our group, the total nomogram scores varied from 0 to 260, facilitating survival estimation for healthcare providers and patients.

Nomogram for predicting survival outcomes in HER-2-negative breast cancer patients after NAC.
Evaluation of the predictive model
The nomogram demonstrated good discrimination, achieving a C-index of 0.863 (95% CI: 0.786–0.939), 0.723 (95% CI: 0.631–0.815), and 0.784 (95% CI: 0.687–0.881) in the training, internal validation, and external validation sets, respectively. These results indicated robust generalizability.
Time-dependent ROC curve analysis demonstrated the model’s predictive performance, with AUCs of 0.920, 0.887, and 0.845 at 3, 5, and 8 years, respectively, in the training set (Figure 4(a)). The AUCs were 0.667 and 0.791 at 3 and 5 years, respectively, in the internal validation set (Figure 4(b)), and 0.849 at 3 years in the external validation set (Figure 4(c)). These results confirmed model robustness.

ROC curves for overall OS. (a) ROC curves for 3-, 5-, and 8-year OS in the training set. (b) ROC curves for 3- and 5-year OS in the internal validation set. (c) ROC curve for 3-year OS in the external validation set.
Calibration plots for the training set (Figure 5(a) and (b)), internal validation set (Figure 5(c) and (d)), and external validation set (Figure 5(e)) showed strong alignment between predicted and observed survival, confirming calibration accuracy. Decision curve analysis (Figure 6) further demonstrated clinical utility with increased net benefit across risk thresholds.
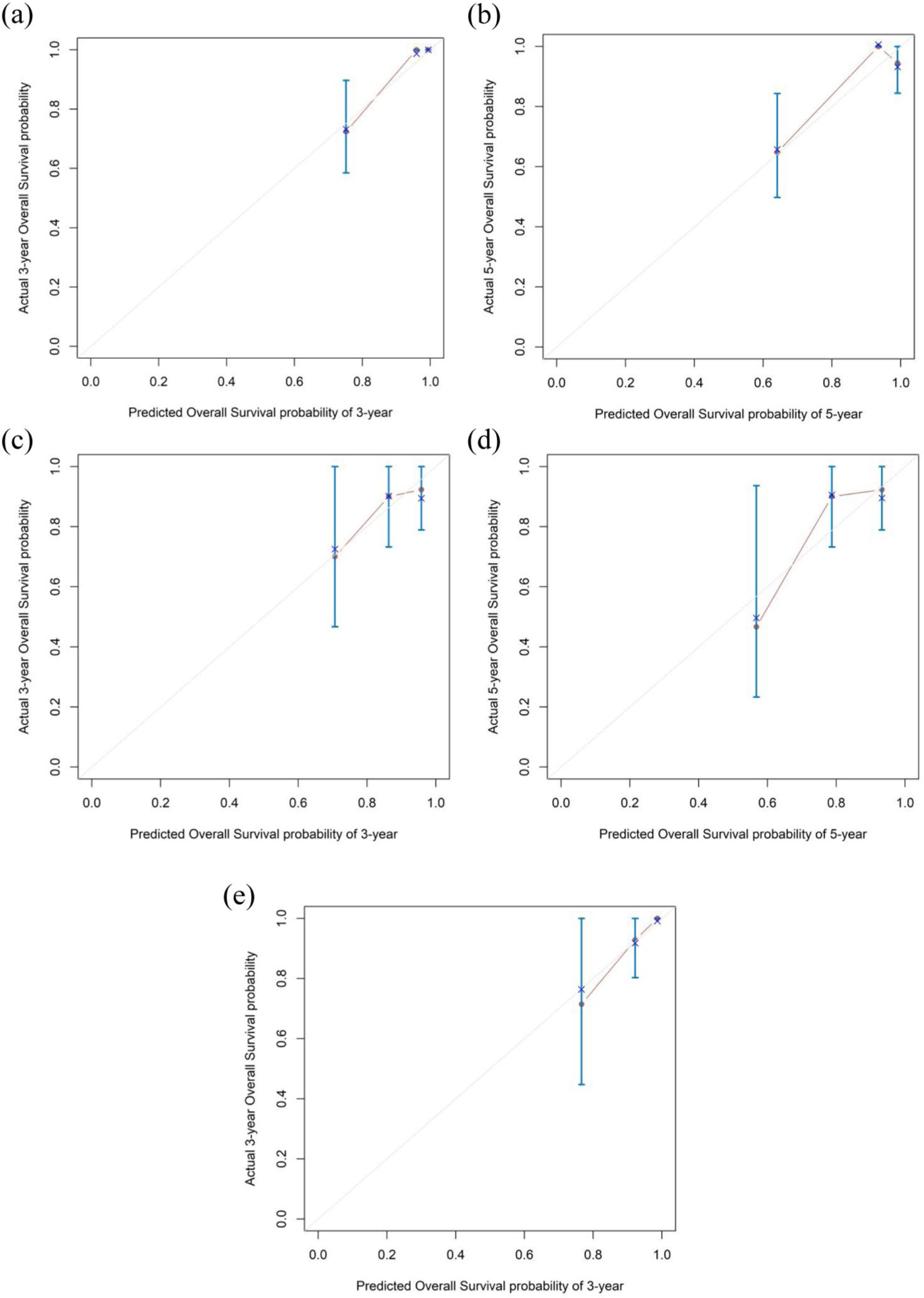
Calibration curves for predicting OS. (a) 3-Year OS in the training set. (b) 5-Year OS in the training set. (c) 3-Year OS in the internal validation set. (d) 5-Year OS in the internal validation set. (e) 3-Year OS in the external validation set.

DCA curve of the nomogram predicting prognosis in HER2-negative breast cancer after NAC.
We assessed the model’s performance separately for pCR and non-pCR patients. The AUC was 0.864 (Supplemental Figure 3(A)) and 0.811 (Supplemental Figure 3(B)) in the pCR and non-pCR subgroups, respectively. These results demonstrated the nomogram’s effectiveness in both response-based subgroups.
Discussion
This study systematically evaluated the prognostic significance of baseline PLR in patients with HER2-negative breast cancer undergoing taxane–carboplatin-based NAC. While PLR was not independently associated with pCR, a high PLR was significantly correlated with poorer OS, particularly in the non-pCR subgroup. These findings suggest that PLR may potentially serve as a simple and accessible marker of systemic inflammation and immune status, holding promise for identifying high-risk patients and informing individualized postoperative treatment strategies.
Recent advances in biomarkers and treatment strategies have significantly transformed breast cancer management. In particular, Ki-67 can be used to predict pCR in luminal breast cancer, 31 PARP inhibitor resistance may be overcome in TNBC, 32 and novel targeted therapies have been developed for HER2-positive 33 and HER2-low subtypes. 34 However, there is a persisting lack of simple, cost-effective, and broadly applicable biomarkers for individualized risk stratification, particularly in HER2-negative patients. Our study demonstrates the prognostic value of the PLR, an accessible inflammation-based marker, in guiding postoperative management in non-pCR patients.
Taxane–carboplatin combination is a commonly used NAC regimen for HER2-negative breast cancer. Carboplatin triggers apoptosis via DNA double-strand breaks, showing efficacy in patients with TNBC with BRCA-associated DNA repair deficiencies. 35 Taxanes stabilize microtubules and inhibit mitosis, thereby inducing cell cycle arrest and apoptosis.11,36 Several studies have confirmed that this combination boosts pCR rates in TNBC9,15 and also shows efficacy in the HR+/HER2− subtype.8,17 However, the long-term survival benefit of this regimen remains inconclusive.
The taxane–carboplatin NAC regimen has significantly improved short-term efficacy, as reflected by higher pCR rates. However, its impact on long-term survival remains inconclusive, and there is a lack of reliable tools for risk assessment, particularly in the postoperative management of non-pCR patients. This study identified PLR as an independent predictor of OS, demonstrating strong risk stratification capability, especially within the non-pCR subgroup. Incorporating PLR into this treatment pathway may help address the limitations of this regimen. Thus, it could help evaluate long-term outcomes, enhance overall management strategies, and provide more targeted postoperative interventions for patients without complete remission. Ultimately, this would facilitate a clinical shift from “improving response rates” to “improving survival outcomes.”
PLR serves as a low-cost indicator of systemic inflammation and immune status.
Platelets promote tumorigenesis and progression by enhancing angiogenesis, preventing apoptosis, and protecting circulating tumor cells from immune detection. 37 While lymphocytes support anti-tumor immunity, lymphopenia reflects immune dysfunction. High PLR, marked by elevated platelets or lymphopenia, suggests a pro-inflammatory, immunosuppressive tumor microenvironment linked to greater invasiveness and metastasis. 18
Our findings showed that in TNBC, high PLR was not an independent predictor of pCR post-NAC, consistent with those from previous studies.38,39 The discrepancy between the prognostic significance of PLR for OS and its lack of predictive value for pCR may reflect distinct biological processes underlying short-term chemotherapy response and long-term disease progression. pCR is primarily determined by tumor-intrinsic factors such as proliferative activity, genetic alterations, and chemosensitivity. Meanwhile, systemic inflammation captured by PLR may influence the tumor microenvironment, immune surveillance, and metastatic potential over time. Elevated PLR, indicative of a pro-inflammatory and immunosuppressive state, may not directly affect initial chemotherapy sensitivity but can promote tumor progression, recurrence, and poorer long-term outcomes. Lusho et al. 40 reported that a high PLR independently predicted pCR in patients with TNBC post-NAC. The disparity in findings may stem from variations in study methodologies. Compared to this previous study, our study encompassed additional confounding factors (e.g., tumor size, lymph node, and Ki-67), potentially explaining the difference in outcomes. A recent meta-analysis by Qi et al. 41 also found no significant link between baseline PLR and pCR in TNBC. Similarly, high PLR was not significantly associated with pCR in HR+/HER2− cases, consistent with the findings of Graziano et al. 42 Indeed, they found that PLR is not an independent predictor of pCR across breast cancer subtypes.
While some studies 43 have suggested a potential association between lower PLR pre-treatment and higher pCRs, further validation is warranted. In our cohort of HER2-negative breast cancer patients treated with a taxane–carboplatin-based NAC regimen, elevated PLR was not significantly associated with pCR but emerged as an independent predictor of OS. Along with ER positivity and clinical stage III disease, PLR was identified as an independent prognostic factor for OS. Specifically, high PLR and clinical stage III disease were significantly associated with poorer survival outcomes, whereas ER positivity indicated a more favorable prognosis.
Notably, high PLR was significantly more associated with lower OS than low PLR in the non-pCR subgroup. PLR may serve as a marker for identifying high-risk cases given the poor prognosis of non-pCR patients, particularly those with TNBC. Consistent with the CREATE-X study, 44 postoperative capecitabine improved survival in non-pCR patients with TNBC. Although studies such as Monarche 45 and PENELOPE-B 46 have examined the use of CDK4/6 inhibitors in combination with endocrine therapy for HR+/HER2− non-pCR patients, inconsistent results have hindered the establishment of a standard treatment strategy. Incorporating PLR into preoperative assessment may facilitate the early identification of high-risk subgroups and support more tailored postoperative treatment decisions.
The nomogram model constructed using PLR, ER status, and clinical stage demonstrated excellent performance in predicting OS in patients with HER2-negative breast cancer. The model achieved a C-index of 0.863, with 3-, 5-, and 8-year AUC values of 0.920, 0.887, and 0.845, respectively, indicating strong discriminative ability and long-term predictive accuracy. The calibration curve showed good agreement between predicted probabilities and actual outcomes, while decision curve analysis further confirmed the model’s high clinical net benefit. Notably, in the non-pCR subgroup, the model enabled early identification of high-risk patients and provided a scientific basis for identifying patients who needed intensified postoperative interventions.
Furthermore, the model is based on three routinely available preoperative indicators (PLR, ER status, and clinical stage), requires no additional testing, and is easy to implement in clinical settings—including those with limited medical resources. External validation in an independent cohort from Fujian Cancer Hospital yielded results consistent with those of the FUSCC cohort, suggesting that the model has strong generalizability and broad clinical applicability.
In conclusion, this study is the first to systematically validate the prognostic value of PLR for OS in patients with HER2-negative breast cancer treated with a taxane–carboplatin NAC regimen. The results help address the lack of long-term prognostic biomarkers in this field. The nomogram model incorporating PLR, ER status, and clinical stage serves as a valuable tool for clinical risk stratification and treatment decision-making, particularly in guiding intensified interventions for non-pCR patients. This model holds significant potential for broad clinical translation.
Nevertheless, this study has several limitations despite the inclusion of a large multicenter cohort and external validation. First, selection bias may have occurred due to the retrospective design, as patients with incomplete clinical or follow-up data were excluded, potentially affecting the representativeness of the study population. Second, the absence of dynamic PLR monitoring precluded assessment of the impact of PLR changes during NAC on prognosis. Serial measurements may better reflect the patient’s inflammatory response and treatment efficacy over time. In addition, the external validation cohort included only 34 patients, which may limit the generalizability and statistical power of the nomogram model. These limitations highlight the need for larger, prospective multicenter studies to further validate the model’s predictive performance and clinical applicability.
Conclusion
This study assessed PLR’s prognostic value in patients with HER2-negative breast cancer receiving taxane–carboplatin NAC. The results showed that while baseline PLR did not predict pCR, high PLR was independently associated with worse survival post-NAC. A nomogram incorporating PLR and clinicopathological variables exhibited strong predictive accuracy for patients with diverse treatment responses, aiding in postoperative risk assessment and personalized treatment planning. Therefore, taxane–carboplatin combined with PLR assessment may be pivotal in treating HER2-negative breast cancer.
However, due to the retrospective design and limited external validation, prospective multicenter studies are warranted. Future research may also explore the integration of PLR-guided strategies into clinical decision-making algorithms to improve survival outcomes, particularly in non-pCR patients.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251369041 – Supplemental material for Platelet-to-lymphocyte ratio as a prognostic biomarker in patients with human epidermal growth factor receptor 2-negative breast cancer undergoing taxane–carboplatin-based neoadjuvant chemotherapy
Supplemental material, sj-docx-1-tam-10.1177_17588359251369041 for Platelet-to-lymphocyte ratio as a prognostic biomarker in patients with human epidermal growth factor receptor 2-negative breast cancer undergoing taxane–carboplatin-based neoadjuvant chemotherapy by Qiuyan Huang, Kai Huang, Jinxian Qian and Yinlong Yang in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.