
Abstract
Purpose:
To analyze the profile of annual recurrence rate (ARR) of patients with early breast cancer (BC) in Tunisia.
Patients and methods:
We classified 293 patients with histologically confirmed early BC relapsing after 1 year of follow up into three subgroups: hormone receptor (HR)+ ‘HR’ [estrogen receptor (ER)+ or progesterone receptor (PR)+ and human epidermal growth factor receptor 2 (HER2)–], triple negative ‘TN’ (ER–, PR– and HER2 score 0/1 or fluorescence in situ hybridization (FISH)/chromogenic in situ hybridization negative) and HER2 overexpression ‘HER2’ (HER2+). ARR was restricted to follow-up contribution of each specified time interval. The HR group was the reference group for comparison.
Results:
A higher proportion of patients who were up to 35 years old (18% versus 10%, p = 0.04), and patients with obesity (46% versus 26%, p = 0.045) was seen in the TN group. Median time to relapse (MTR) was shorter in TN and HER2 groups than in HR patients (20 and 29 months compared with 56 months, respectively, p < 0.001). In the HR group, the ARR was 22%, 16% and 10% at 3, 4 and 5 years respectively, becoming less than 3% at 7 years. In the TN group, 71% of patients relapsed during the first 2 years and the ARR declined rapidly to less than 1.5% after 4 years. In the HER2 group, the ARR peaked at 2 years (29%) and decreased significantly to 7% and 3% at 5 and 7 years respectively. Adjuvant trastuzumab delayed the MTR from 24 to 34 months (p = 0.022).
Conclusion:
The relapse risk in Tunisian patients is higher in young women and patients with HER2+ and TN tumors. A long and close follow up is recommended for patients with HR and HER2. Conversely, we suggest that follow up in patients with TN could be spaced after 4 years (ARR being <1.5% after this period).
Keywords
Introduction
Breast cancer (BC) is the most common female malignancy worldwide, as well in Tunisia, where its incidence is still growing like in other Arab Countries. Most of occidental cases are detected at infraclinical and small-sized stage thanks to mammographic screening: in Tunisia and emerging countries, BC remains diagnosed at the clinically palpable stage [Chouchane et al. 2013]. Clinical size greater than 2 cm and age up to 35 years, as well as axillary node invasion, grade, hormone receptors (HRs) and human epidermal growth factor receptor 2 (HER2) status are the most important parameters to evaluate relapse risk and to indicate adjuvant therapies according to the international consensual guidelines for early BC [Goldhirsch et al. 2013]. The available statistical models predict relapse risks varying from less than 10% for N–/HR+/HER2– to over 30% for N+/HER2+ and triple negative (TN) tumors [Cardoso et al. 2010]. Saphner and colleagues, in their pivotal multicentric retrospective study concerning early BC cases, treated in the 1990s by anthracycline-based chemotherapy and tamoxifen, reported the annual relapse profile of these patients and their work may be considered as a good historical reference [Saphner et al. 1996]. In 2000, Perou and colleagues proposed a new molecular classification based on microarray gene expression of BC: basal like, HER2 enriched, normal breast like and luminal divided subsequently into luminal A and luminal B [Perou et al. 2000; Zepeda-Castilla et al. 2008]. In 2011, the four subtypes were included in treatment guidelines by the St Gallen International Expert Consensus group [Goldhirsch et al. 2011]. The highest correlation between gene expression patterns and immunohistochemical (IHC) phenotype is observed in HR and basal like BC (73–100%), and lower in HER2 BC (41–69%) [Guiu et al. 2012; Spitale et al. 2009]. A strong relationship between IHC markers and responsiveness to systemic therapy has also been demonstrated, however only few studies investigated BC according to Perou subtypes and their relapse profile, particularly in North African and Arab patients.
In the present study we aimed to report clinicopathological aspects of BC relapse according to IHC classification, to describe recurrence profile and to suggest a personalized long-term follow up.
Patients and methods
We analyzed a cohort of 1400 cases of histologically confirmed early BC treated with curative intent in the period 1999–2010. All patients had complete workup, including chest X-ray, abdominal ultrasound and bone scan. We identified 324 patients who relapsed during follow up (between 2001 and 2012); both locoregional and distant relapses were considered. Diagnosis of distant and local/regional relapses was based on clinical, radiological and histological findings. Data concerning age, menopausal status, obesity, TNM stage, histological findings (grade, pN) were collected. Three BC subtypes were defined according to IHC profile collected from pathology reports. We excluded patients relapsing during the first 12 months after diagnosis, secondary cancers, controlateral BCs, lobular carcinomas and male sex.
Management of BC in Tunisia follows international (French/European Society for Medical Oncology/National Comprehensive Cancer Network) guidelines adapted to the available drugs in the country. Patients received anthracycline-based chemotherapy in the adjuvant or neoadjuvant settings until 2004, then sequential anthracycline and taxane chemotherapy became the standard of care. Trastuzumab has been used in the adjuvant or neoadjuvant setting since 2010. Tamoxifen was the only available endocrine therapy in the adjuvant setting. The aromatase inhibitors letrozole, anastrozole and exemestane, in the frontline or in switch approach, were introduced in 2009.
After completion of the adjuvant chemotherapy and radiotherapy patients had regular visits every 3–4 months in the first 2 years, every 6 months from years 3 to 5 and annually thereafter. At each visit patients had a physical examination and were checked for symptoms. Mammography was performed annually; chest X-ray and abdominal ultrasound were performed every 6 months for high-risk patients. A lipid blood test was performed for patients on aromatase inhibitors and an annual gynecological examination was carried out for patients on tamoxifen.
This study had ethical approval of the local committee. At the moment of diagnosis, all patients were informed about their disease, prognosis, risk of relapse and possible publication of their case. All the patients gave their consent.
Definition of breast cancer subtypes
IHC analysis was performed on the primary tumor of 293 specimens of primary BC (biopsy or surgical resection). We individualized three subgroups: TN defined as estrogen receptor (ER)–, progesterone receptor (PR)– and HER2–, hormonal receptor (HR)+ defined as ER+ or PR+ and HER2–, and HER2 overexpressed (HER2) defined as HER2+.
Annual recurrence rate (ARR) and median time to relapse (MTR) were studied in the following subgroups: age (⩽35 years, >65 years), menopausal status, obesity (body mass index < 30 versus ⩾ 30), histological nodal involvement (positive versus negative), grade (I versus II/III) and trastuzumab administration. HER2 antibody type Novocastra NCL-HER clone NCL-N-CB11 was used. Only membrane staining was scored according to standard criteria. HER2 positivity was assessed using the following scoring system: 0, no membrane staining or less than 10% of cells; 1, partial membrane staining in more than 10% of cells; 2, weak, circumferential membrane staining in more than 10% of cells or intense membrane staining in less than 30% of cases; 3, intense membrane staining in more than 30% of cells. Protein overexpression was considered present if IHC score was 3. Specimens with a score of 2 were selected for chromogenic in situ hybridization (CISH) analysis. HER2+ tumors were either scored 3 by IHC or HER2 amplified on the basis of CISH. HR status was evaluated using Novocastra NCL-ER-6F11 and NCL-PR-312. HR was considered positive if greater than 10% of IHC staining was observed.
Statistical analysis
MTR was defined as the interval between the date of first therapeutic action and relapse occurrence. ARR was defined as the fraction of followed patients that had recurring disease in a 1-year period restricted to follow-up contribution of each specified time interval. ARR was calculated for each IHC BC subtype. Log-rank test was used to compare subgroups with statistical significance if p was less than 0.05. We compared different variables between groups considering HR as the reference group.
Population
With a median follow up of 67 months (5.7 years) during the period 1999–2012 for a cohort of 1400 early BC cases, 324 patients (23%) relapsed. Median age was 48 years (range 23–85). We observed 12% were up to 35 years old, 82% were between 35 and 70 years old and 6% were over 70 years. A total of 60% (193) were menopausal. Obesity (BMI ⩾ 30) was seen in 44% (142) with 15% (49) having morbid obesity (BMI > 40). Among patients with obesity 11% were under the age of 35 years. Mean age was not statistically different between patients who were obese and nonobese (44 versus 48 years, p = 0.9). Mean clinical tumor size was 34 mm (range 10–150 mm). T1 and T2 tumors represented 14% and 54% of cases, T3 and T4 represented 17% and 14% of cases, 8% had an inflammatory BC. All patients had systemic therapy (chemotherapy or hormonal therapy). First treatment was neoadjuvant chemotherapy in 27% (88 patients) and surgery in 73% (236). In HR patients, 12.4% received only tamoxifen adjuvant therapy. The first anatomic site of relapse was visceral in 48% (149), bone in 28% (91) and local in 18% (59) of cases (Figure 1).
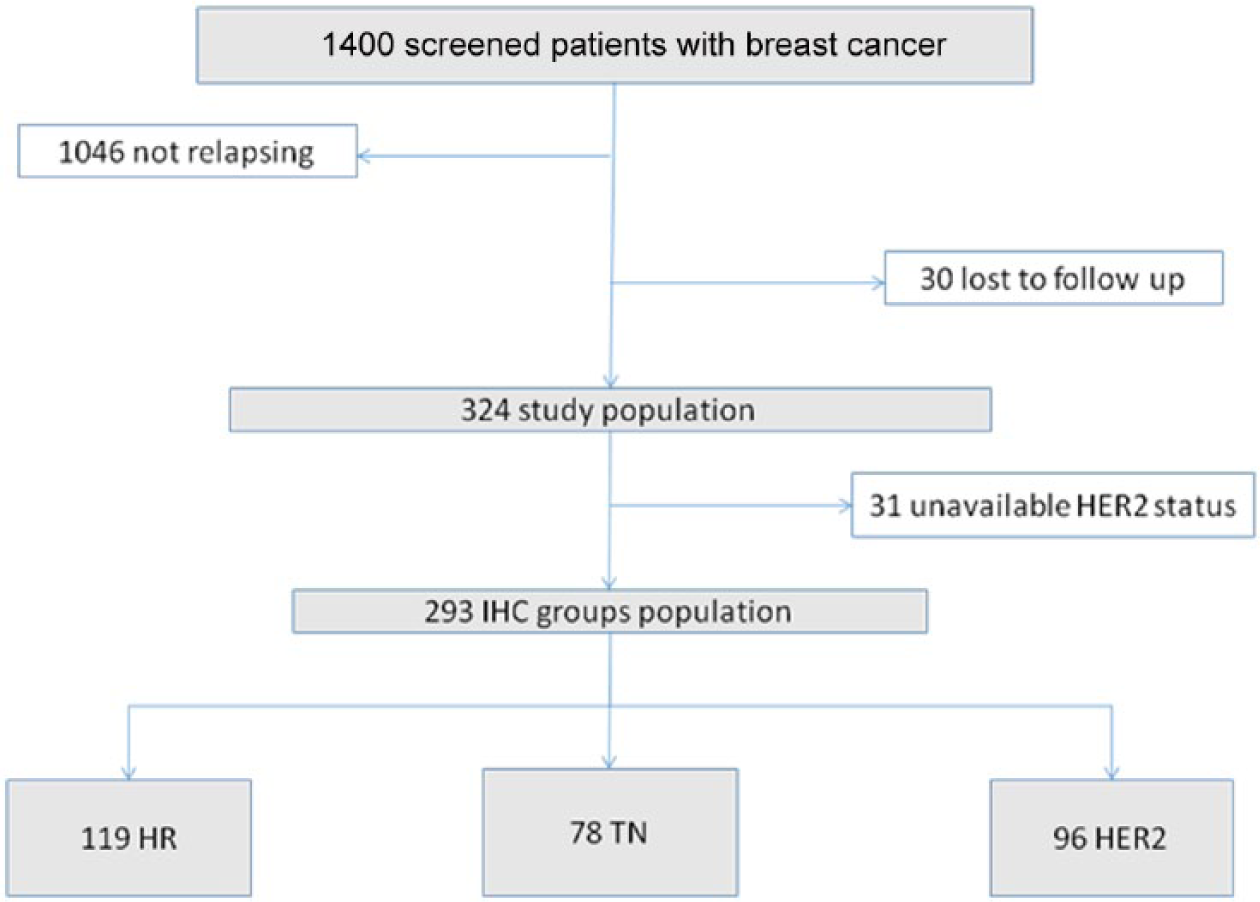
Flow diagram of the screened population. HER2, human epidermal growth factor receptor 2; HR, hormone receptor; IHC, immunohistochemical; TN, triple negative.
Results
Within the 324 relapses, IHC was performed in 293 cases. We observed 41% HR (119), 33% HER2 (96) and 26% TN patients (78). Median tumor size, percentage of inflammatory BC, type of surgery, grade and nodal status were comparable in the three groups. HER2 patients were younger but without statistical significance (p = 0.51). The proportion of very young patients (⩽35 years) was higher in the TN group (18% versus 10%, p = 0.04). We observed fewer older patients (>65 years) in the HER2 group (8% versus 19%, p = 0.02). T4 tumors were more frequent in the TN (24%) and HER2 groups (20%) compared with the HR group (7%, p < 0.05). More patients with obesity were observed in the TN (46%) and HER2 (39%) groups compared with the HR group (26%, p < 0.05). The first anatomic site of recurrence was more frequently bone in HR patients (46%) compared with TN (14%) and HER2 (30%), with p < 0.05. No difference was seen in terms of visceral and local recurrences within the three groups. We observed more brain relapses in the TN and HER2 groups (10% versus 2%, p < 0.05) (Table 1).
Patient’s characteristics according to immunohistochemistry subgroups: HR, TN, HER2.

BC, breast cancer; BMI, body mass index; HER2, human epidermal growth factor receptor 2; SBR, Scarff-Bloom-Richardson HR, hormone receptor; R, reference group for comparison; TN, triple negative.
Bold figures in the last column are the statistically significant results.
The second R is given in the last line of the table is the reference group for comparison.
Median follow up was 76 months in the HR group, 49 months in the TN group and 56 months in the HER2 group. MTR for the overall population was 47 months. Compared with HR patients, MTR was statistically significant earlier in the TN and HER2 groups, 20 and 29 months versus 56 months (p < 0.001).
ARR of the overall population and among IHC subgroups is represented in Figure 1. In the HR BC group, 20% relapsed within the first 2 years, ARR peaked at 3 years (22%), remaining high with 16.8% and 10.8% at 4 and 5 years respectively. It became less than 3% after 7 years. In the TN group, 71% of patients relapsed within the first 2 years, ARR peaked at the first second year interval (42%), ARR declined rapidly thereafter becoming less than 1.5% after 4 years. In the HER2 group, 44% relapsed within the first 2 years, ARR peaked at 2 years (29.2%); however, it decreased significantly to 7% and 3% at 5 years and 7 years (Figure 1).
In a subgroup analysis, MTR was statistically significantly shorter in patients who were node positive compared with those who were node negative (41 versus 59 months, p = 0.04). At 2 years, 38% of patients who were node positive relapsed. Compared with patients who were HR+, those who were HR– had an earlier and a higher ARR; 41% relapsed between the first and the second year. MTR was also shorter in patients who were HR– (28 versus 59 months, p = 0.003). MTR was longer in patients without obesity (39 versus 50 months, p = 0.001). We observed 30% ARR at 2 years. We did not observe a difference in MTR between menopausal and nonmenopausal women (49 versus 44, p = 0.3) and also between grade I tumors and grade II/III tumors (51 versus 46, p = 0.051). We did not observe a statistical difference in MTR in patients who received neoadjuvant therapy (78) compared with those who received adjuvant therapy (215) (45 versus 47 months, p = 0.7). In the HER2 group, only 43% (42 patients) received trastuzumab. Mean age (41 versus 39, p = 0.6), tumor size (32 versus 34, p = 0.7) and grade were comparable between patients who received trastuzumab and those who did not respectively. Patients who received trastuzumab were more likely to receive taxanes (67% versus 33%, p = 0.04). Trastuzumab delayed MTR by 10 months (24 versus 34 months, p = 0.022) (Figure 3).
Discussion
Our early BC relapsing series is representative of BC presentation in Tunisia, where in the absence of mammographic screening, BC is frequently ‘bulky’ with palpable tumors and a mean clinical tumor size greater than 4 cm [Mook et al. 2010]. Most of the patients in Tunisia are within the intermediate and high relapse risk categories of St Gallen [Goldhirsch et al. 2011]. These unfavorable parameters explain the high relapse rate of 23% (324/1400) observed in our series. Our rate is higher than that reported in the historical series of Saphner in the 1990s concerning first relapse profile of early BC treated during the period of adjuvant anthracyclines based chemotherapy and tamoxifen [Saphner et al. 1996]. This is explained by the young age at diagnosis (48 years, 10–15% being ⩽35 years), 10 years younger than in Europe and the USA [Chouchane et al. 2013]. Age is reported by some authors as an independent prognostic and predictive factor of early recurrence [Najjar and Easson, 2010]. In addition, 7% of our patients presented with inflammatory BC, which is known to be more aggressive than ‘classical’ BC with a high risk of locoregional and high distant relapse rate with poor survival. Tunisian data reported by Boussen and colleagues showed a 5-year survival of 8.5% in the anthracyclines era before taxanes and trastuzumab [Boussen et al. 2010]. We also observed that obesity was associated with an earlier median relapse time. As reported in the literature, this parameter is a risk factor but also a survival indicator in women diagnosed with BC. These data were confirmed by a meta-analysis published in 2010 [Protani et al. 2010; Goodwin et al. 2002]. The high mean tumor size (34 mm) and N+ (60%) observed in our population are also known major negative predictive factors. Local or regional recurrence for early BC occurs in approximately 5% of cases at 5 years [Eikhuizen et al. 1998], higher in HER2 and basal subtypes compared with luminal A BC [Wallgren et al. 2003]. However, in our series, we noted a relatively high proportion (18%) of local recurrence but without statistical difference. This fact could be attributed to the high proportion of T4 stage [Carreño et al. 2007] as well as young age.
Our series is a mixture of ‘Saphner-like’ patients and anthracycline–taxanes–trastuzumab patients. As noted in Figure 2, the introduction of trastuzumab modified the relapse profile by decreasing and delaying the peak intensity by more than 10 months. In the pivotal HERA trial, adjuvant trastuzumab clearly improved overall and disease-free survivals [Untch et al. 2008]. The pattern of recurrence in the HER2 population was that of a peak hazard of recurrence of 29.2% during the second year of follow up, followed by a steady decrease in the annual hazard of recurrence until year 6. Beyond that time, the hazard of recurrence slowly declined and averaged 3%.

Annual recurrence rate per year interval of the entire population and immunohistochemical subgroups. HER2, human epidermal growth factor receptor 2; HR, hormone receptor; TN, triple negative.
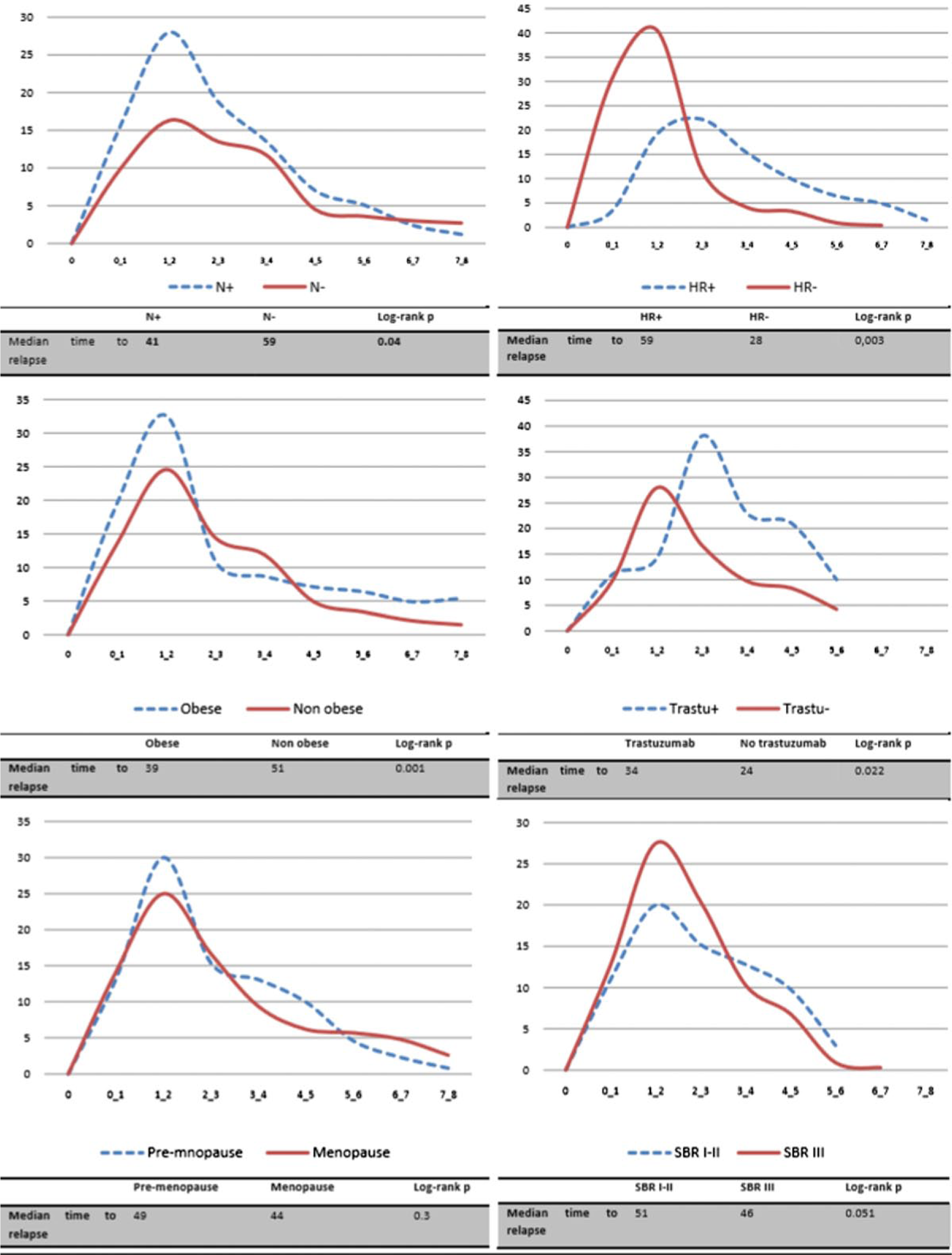
Annual recurrence rate per year interval of subgroup analysis.
Thanks to the introduction of new drugs into the continuum of care of BC, the relapse profile modification was similarly reported by Jatoi and colleagues, showing hazard curves for BC death that peaked between 2 and 3 years after initial diagnosis and declined sharply afterwards [Jatoi et al. 2011]. In their study, the annual hazard rate for all cases peaks near 3% per year between the second and third years after diagnosis and decreased to 1–2% per year by the sixth through eighth years. The hazard rates for ER– and ER+ tumors peak at approximately 6.5% and 2% per year respectively between the first and third years. Notably, ER– to ER+ hazard rates cross between the seventh and eighth years, after which women with ER– tumors have a lower rate of BC death than those with ER+ tumors.
Our graphs showed that TN BC has the highest and earliest risk of recurrence, less than two-thirds of patients relapsing during the 4 years of follow up. Dent and colleagues also reported a recurrence peak at 12 months, remaining high for the first 4 years and decreasing rapidly thereafter. We believe that women with TN BC who do not relapse in the first 4 years are at low relapse risk [Dent et al. 2007].
HR patients had the latest ARR peak with a remaining risk beyond year 6. Saphner and colleagues reported a higher hazard of recurrence in patients who were ER– during the first years of follow up. However, beyond 5 years the hazard was higher for patients who were ER+. They suggested that the hazard of recurrence for patients who were ER+ was relatively constant, while the hazard of recurrence for patients who were ER– decreased significantly with time [Saphner et al. 1996].
In Tunisia, the available initial workup for metastases detection is based on conventional chest X-ray, abdominal ultrasound and bone scan, revealing more than 10% of patients who are metastatic at diagnosis. Infraclinical metastatic disease is better detected with fluoro-2-deoxyglucose positron emission tomography (FDG-PET) (not yet available in Tunisia). It has been clearly proved as more sensitive than conventional imaging procedures for detection of distant BC metastases and particularly in our intermediate to high risk population with 60% of node-positive cases [Heusner et al. 2010; Maalej et al. 2008].
In patients with HER2 and HR BC we suggest long and close follow up, beyond 5 years; however, we suggest that follow up for patients with TN BC could be spaced after 4 years since, in our series ARR was less than 1.5% after that period.
Many models of risk prediction have been developed and are available online to help oncologists in the selection of patients who could benefit from adjuvant chemotherapy and hormone therapy. Initial tools such as adjuvant online were based on traditional clinicopathological factors and the more recently used biomolecular/genomic parameters like Oncotype DX or MammaPrint, but they remain suboptimal for patients under 40 or over 65 years old [Mook et al. 2010; Dowsett et al. 2013]. Adjuvant online evaluation risks an overestimation of overall survival by 20% and the use of Mammaprint classified 20% more patients in the high-risk group. Most of the validation studies are retrospective and performed in heterogeneous populations, making the assumption that currently available risk prediction models are clinically valid too weak. Moreover, ethnic variations between occidental and Asian populations have been reported for the different prediction models, maybe explained by gene disparities [Engelhardt et al. 2014]. There are no available data concerning those risk prediction models considering Arab or African populations.
Conclusion
This is the first study about the early BC relapse profile in North African and Arab patients when considering an intermediate to high risk St Gallen population. As expected, the cohort is in line with the specific Tunisian BC anatomoclinical characteristics in terms of young median age, high clinical/histological tumor volume and poor histological features impacting negatively and explaining the high rate of relapses. However, we noted that modifications of treatment protocols during the study period induced a transition in relapse profile within recently treated patients by sequential anthracycline, taxanes and trastuzumab that presented a delayed and decreased relapse peak. Relapse risk of early BC in Tunisian patients seems to be higher in young women with a high proportion of HER2 tumors. Long and close follow up is recommended in patients with HR (6 years) and HER2 (7 years) BC, after which the recurrence rate becomes less than 3%. Adjuvant trastuzumab delayed recurrence time in this group. We suggest that follow up for patients with TN BC could be spaced after 4 years (ARR becoming <1.5%).
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work did not receive any grant.