
Abstract
Objective
To assess the neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR) and systemic immune-inflammatory index (SII), as diagnostic markers for neonatal sepsis.
Methods
This retrospective study involve neonates with sepsis and healthy neonates as controls. NLR, PLR, and SII were compared between groups.
Result
In total, 60 neonates with sepsis and 60 healthy controls were involved in the study. Compared with controls, the sepsis group had higher values for NLR, PLR and SII. Logistic regression analysis suggested that the NLR, PLR and SII were independent risk factors for neonatal sepsis. In addition, receiver operating characteristic (ROC) curve analysis indicated that the NLR, PLR and SII were reliable predictors of neonatal sepsis and SII had the best predictive value.
Conclusions
NLR, PLR and SII appear to be useful indicators for predicting neonatal sepsis.
Keywords
Introduction
Neonatal sepsis is a systemic inflammatory response syndrome (SIRS) induced by viral, bacterial, or fungal infection, and is a major cause of morbidity and mortality in neonates.1,2 Despite significant advances in neonatal care in developed countries, many infants with sepsis die or suffer from a major disability. 3 The current gold standard for diagnosis of neonatal sepsis is the presence of positive blood culture and systemic signs and symptoms of infection. 4 However, blood culture results typically have a 48–72 h turnaround time after collection, and, are positive in only 60–80% of newborns with sepsis.4–7 In addition, its non-specific clinical signs and symptoms makes early diagnosis of sepsis challenging. 8 Therefore, there is a need for an accurate and sensitive diagnostic tool to confirm the diagnosis of neonates with sepsis at an early stage and so save lives.
The neutrophil to lymphocyte ratio (NLR), the platelet to lymphocyte ratio (PLR) and the systemic immune-inflammatory index (SII; an index for evaluating inflammation based on neutrophil, lymphocyte, and platelet counts) have been used as early diagnostic indicators and prognostic predictors for acute and chronic inflammatory diseases9–11 In addition, several studies have suggested that NLR and PLR have predicted value for early onset neonatal sepsis.12–16 However, to our knowledge, limited data exist on the value of all three biomarkers (i.e., SII, NLR and PLR) in identifying neonates with sepsis. 17 Therefore, the aim of this retrospective, controlled, study was to evaluate the value of NLR, PLR and, SII in the diagnosis of sepsis in newborns, to help identify sepsis, and facilitate intervention in a timely manner.
Methods
This retrospective study involved neonates with early or late onset neonatal sepsis and healthy control neonates who were admitted to the First People's Hospital of Linping District, Hangzhou from January 2017 to January 2024. Diagnosis of sepsis was determined by clinical manifestations, positive blood culture, or positive cerebrospinal fluid (CSF), or other sterile cavity fluid culture. 18 Therefore, inclusion criteria for neonatal sepsis were one of the following: white blood cell (WBC) count ≥30 × 109/l at 6 hours to 3 days after birth; CSF positive for bacterial meningitis; DNA of the causative organism detected in blood. Neonates with congenital anomalies or genetic metabolic abnormalities, and/or severe asphyxia, were excluded from the study.
The following data were obtained from hospital records: mode of conception; presence of premature rupture of membranes (PROM); gestational age (GA); birth weight; sex; Apgar score; early or late onset sepsis (based on sepsis occurring before or after 7 days). The NLR, PLR, and SII (i.e., neutrophil count × platelet count/lymphocyte count) were calculated based on complete blood count obtained at the time of hospital admission.
The study was approved by the medical ethics committee of the First People's Hospital of Linping District (Approval number: 2024048). The subjects’ requirement for informed consent was not needed because of the retrospective nature of the study. All data were collected and retained anonymously. The reporting of this study conforms to STROBE guidelines. 19
Statistical analysis
Statistical analysis was performed using SPSS software (version 26.0 for Windows®; IBM Corp, Armonk, NY, USA). A P-value <0.5 was considered to indicate statistical significance. Normally distributed variables were expressed as the mean ± standard deviation (SD) and t-test for two independent samples was used for comparison between groups. To investigate the possible predictors of sepsis, several parameters were included in a multivariate Cox proportional hazards regression analysis. The results were presented as odds ratio (OR) and 95% confidence intervals (CIs). Receiver operating characteristic (ROC) curves were used to calculate area under the curve (AUC) values to assess the predictive ability of NLR, PLR and, SII for neonatal sepsis. Cutoff points were calculated by obtaining the best Youden index (sensitivity + specificity −1).
Results
In total, 120 neonates were included in the study (60 with sepsis and 60 healthy controls) and approximately 50% of the subjects were male. With the exception of PROM, there were no differences between the sepsis and control groups (Table 1). The groups had similar modes of conception, gestational age, birth weight, and Apgar scores. However, significantly more neonates in the sepsis group compared with the control group had births complicated by PROM (P < 0.05). The sepsis group included early (n = 10) and late-onset neonatal sepsis neonates (n = 50). Of these neonates, 40 (67%) had positive blood cultures (i.e., Escherichia coli, 25 [63%]); Streptococcus pneumoniae, 7 [12%]; Klebsiella pneumoniae, 8 [13%]).
Clinical characteristics.
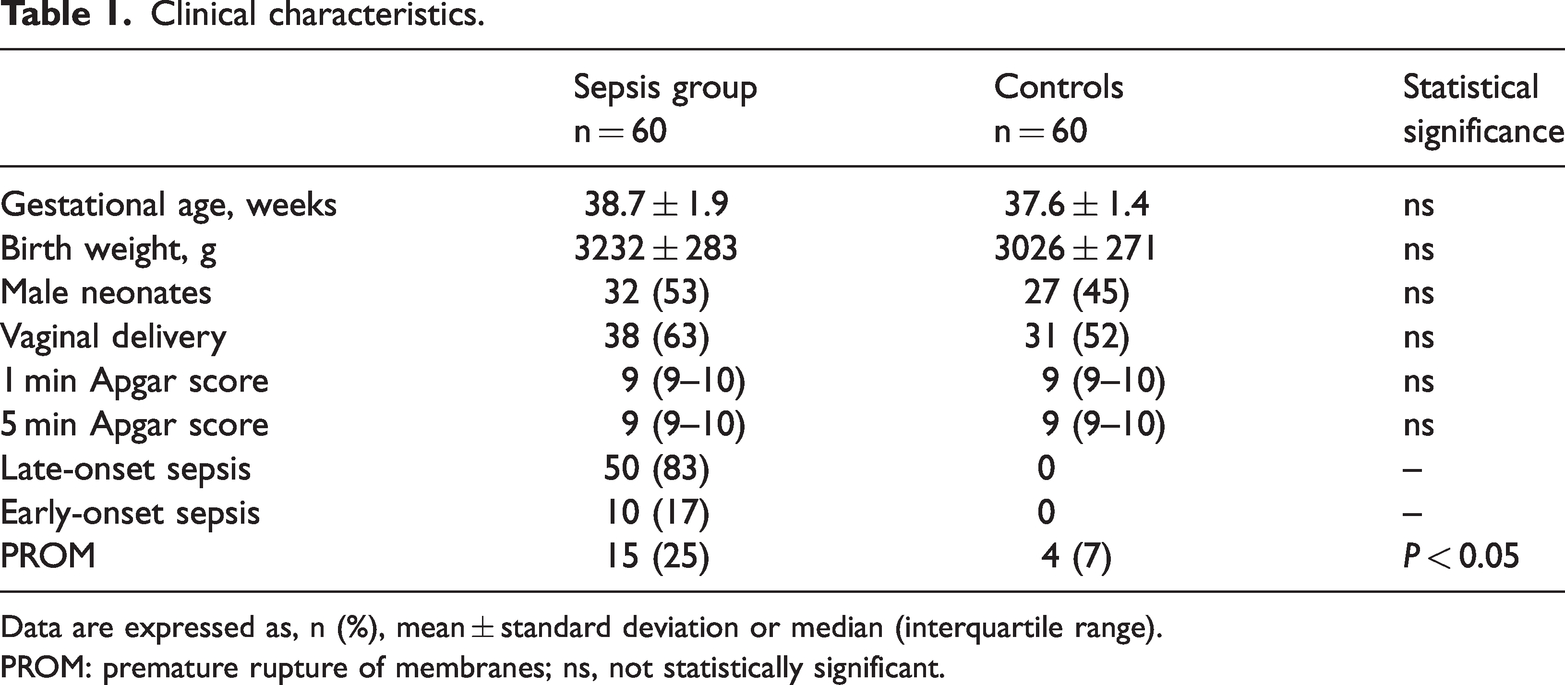
Data are expressed as, n (%), mean ± standard deviation or median (interquartile range).
PROM: premature rupture of membranes; ns, not statistically significant.
Compared with controls, neonates in the sepsis group had significantly higher WBC and neutrophil counts and lower platelet counts (Table 2). Accordingly, compared with controls, neonates with sepsis had significantly higher NLR and SII values whereas PLR values were markedly lower (Table 2). Multivariate logistic regression showed that WBC, NLR, PLR and SII were significant independent factors for sepsis (P < 0.05; Table 3).
Laboratory variables.

Data are expressed as mean ± standard deviation.
WBC, white blood cells; NLR: neutrophil to lymphocyte ratio; PLR: platelet to lymphocyte ratio; SII: Systemic immune-inflammatory index; ns, not statistically significant.
Logistic regression analysis for independent predictors of sepsis.

OR, odds ratio; CI, confidence interval; WBC, white blood cells; NLR: neutrophil to lymphocyte ratio; PLR: platelet to lymphocyte ratio; SII: Systemic immune-inflammatory index; ns, not statistically significant.
ROC curves of the predictive ability of NLR, PLR and SII for sepsis, are shown in Figure 1. Of the three variables, AUC values were highest for SII (0.82) with optimal cut off concentrations of 936, and sensitivity and specificity of 78% and 87%, respectively (Figure 1 and Table 4). For NLR, AUC value was 0.74 with optimal cut off concentrations of 4.2, and sensitivity and specificity of 75% and 72%, respectively. For PLR, AUC value was 0.66 with optimal cut off concentrations of 59.6, and sensitivity and specificity of 73% and 63%, respectively.

Receiver operating characteristic (ROC) curve analysis showing the predictive ability of NLR, PLR and SII for neonatal sepsis. Abbreviations: NLR: neutrophil to lymphocyte ratio; PLR: platelet to lymphocyte ratio; SII: systemic immune-inflammatory index.
Receiver operating characteristic (ROC) curve analysis to assess the predictive ability of NLR, PLR and SII for diagnosis of neonatal sepsis.

AUC: Area under curve; NLR: neutrophil to lymphocyte ratio; PLR: platelet to lymphocyte ratio; SII: Systemic immune-inflammatory index.
Discussion
Neonatal sepsis is a leading cause of neonatal morbidity and mortality especially in developing countries. 20 Prompt diagnosis and treatment of sepsis would certainly prevent deaths but because of its non-specific clinical presentation, and, problems with specific diagnostic indicators, such as a positive blood culture, early diagnosis of neonatal sepsis remains a major challenge. For example, in our study, only 67% neonates with sepsis had positive blood culture results. Therefore, there is a need for new biomarkers that offer early specific and reliable identification of the neonate at risk of serious infection. 21
Similar to results from previous studies, we found that NLR and PLR were independent risk factors for neonatal sepsis.12–17 NLR appears to be more useful as a marker of inflammation than neutrophilia or lymphocytopenia alone, especially in detecting bacterial infection. Moreover, it can be used to predict disease prognosis and survival rates in diseases with systemic inflammation, particularly in some bacterial and bloodstream infections.12,22,23 Platelets play a crucial role in inflammation and host defence, and many researches have shown that thrombocytopenia is a common finding during neonatal sepsis. 24 Consistent with previous findings, we observed that the platelet count was significantly lower in the sepsis group compared with control group.
Previously, SII has been used as marker of inflammation in hepatocellular cancer. 25 Neonatal sepsis is clinical condition with a high risk of inflammation, and so we aimed to determine the predictive value of SII in the diagnosis of this condition. According to results from our ROC curve analysis, we found that SII had a greater predictive ability for sepsis than NLR or PLR (i.e., AUC was 0.82, 0.74, 0.66 for SII, NLR, and PLR, respectively).
Our study had several limitations. For example, our patient population was small and, the study was retrospective. Moreover, it was challenging to ensure consistency of the data because patients had been treated by different physicians. Future large, controlled, multicentre studies are required to confirm our results. Nevertheless, our study provides evidence for the usefulness of NLR, PLR, and SII in the diagnosis of neonatal sepsis. In combination with classical parameters, these biomarkers may be useful as new indicators in the early diagnosis and management of neonatal sepsis.