
Abstract
Background:
Biliary tract cancers (BTC) are often diagnosed after the age of 70, when comorbidities and compromised performance status (PS) are more prevalent.
Objectives:
This study compared clinical and disease characteristics and outcomes in BTC patients aged ⩽70 and >70 years.
Design and methods:
PRONOBIL-ACABI is a cohort study including 1256 BTC patients treated across 16 French centers from January 2003 to June 2021. We analyzed demographics, clinical characteristics, treatment modalities, molecular profiles, overall survival (OS) as the primary endpoint, and progression-free survival (PFS).
Results:
Among the 1256 BTC patients (53% male; median age: 64.5), 31% were aged >70. Patients >70 exhibited poorer PS (PS ⩾2, 17% vs 8%; p < 0.0001), a higher rate of comorbidities (⩾1, 89% vs 78%; p < 0.0001), and were less often proposed a molecular profile (43% vs 65%; p < 0.0001) than those ⩽70. Patients with unresectable BTC aged >70 had significantly shorter OS compared to younger patients (median OS: 14.6 vs 17.4 months, p < 0.0001), despite similar PFS (median PFS: 6.6 vs 5.8 months, p = 0.61). They were also less likely to receive first-line chemotherapy (87% vs 97%, p < 0.0001). In resected BTC, survival outcomes were comparable across age groups, with a median OS of 47.0 months in patients >70 vs 48.8 months in those ⩽70.
Conclusion:
Patients aged >70 years with unresectable BTC had a significantly shorter OS compared to those aged ⩽70, despite similar first-line PFS. In resected BTC, elderly patients achieved OS and PFS outcomes comparable to those aged ⩽70.
Introduction
Biliary tract cancers (BTCs) are rare malignant tumors with a poor prognosis; they are diagnosed at advanced and unresectable stages in 70% of cases. BTCs are subdivided into intrahepatic cholangiocarcinoma (iCCA; 20%), which are upstream of the second division of the bile ducts, extrahepatic cholangiocarcinoma (eCCA), which can be either peri-hilar (60%) or distal (20%), and gallbladder cancers (GBC). The incidence of iCCA is increasing, probably related to lifestyle changes and the increasing incidence of cirrhosis owing to metabolic syndrome.1 –3 Management of localized BTC is based on complete excision surgery, followed by adjuvant treatment with capecitabine for 6 months. 4 The treatment of advanced or metastatic BTC relies on two standards: first-line cisplatin-gemcitabine combined with immunotherapy durvalumab 5 and second-line 5-fluorouracil-oxaliplatin. 6 Nevertheless, the median overall survival (OS) of patients with unresectable cholangiocarcinoma is around 1 year, and 5-year survival does not exceed 10%. 7
Peak incidence of BTC occurs after 70 years of age, with a poorer prognosis in these patients,3,8 making the management of elderly patients with BTC a pressing oncological issue. Indeed, treatment decisions in geriatric oncology are often complex owing to the heterogeneity of the aging process. The presence of comorbidities is one of the major factors influencing ageing 9 ; it is estimated that 80% of people over the age of 65 have at least one chronic disease, and that around 60% of these patients have three or more comorbidities.10,11
The development of high-throughput sequencing techniques and the widespread use of these techniques in routine care showed the high frequency of targetable molecular alterations in BTC.12,13 In iCCA, 50% of molecular alterations are treatable with targeted therapy, including FGFR2 fusions and IDH1 mutations.14,15 HER2 amplifications are found in 10%–15% of extrahepatic cholangiocarcinoma (eCCA) and in around 20% of GBC cases. 16 Molecular profiling-guided treatment of BTC has been shown to bring clear clinical benefit to patients for unresectable disease in second-line treatment.14,15,17,18
This study aims to describe the patients and disease characteristics, treatment, molecular profiling, and prognosis of patients over 70 years of age with BTC compared with patients 70 years old or younger, 19 within a French multicenter cohort.
Methods
Study design
This was a nested, retrospective, multicenter study within an ongoing ACABI GERCOR PRONOBIL cohort (NCT04935853) conducted in 16 French secondary or tertiary centers. Patients eligible for this study were aged 18 or over, diagnosed between 1 January 2003 and 30 June 2021 with a primary BTC (iCCA, eCCA, including peri-hilar and distal CCA, and GBC). Tumors of the ampulla were a non-inclusion criterion. Ampullary tumors were a non-inclusion criterion due to their histological differentiation into intestinal, biliopancreatic, or mixed subtypes, which are considered distinct diseases with different treatment approaches and cannot be grouped with BTC. Exclusion criteria included patients under guardianship, pregnant women, or those who were unwilling to provide consent.
Data
Demographical, clinical, biological, and pathological data, along with information on therapeutic management, molecular profiles, and survival data, were collected. For this study, we categorized patients into two groups: those under ⩽70 years at diagnosis and those >70 years. Electronic case report form records (Cleanweb™) were used to compile a comprehensive dataset.
Molecular sequencing
Molecular profiling was performed for some patients in accordance with French guidelines for the management of BTC, either through panels available in participating centers or as part of therapeutic trials (the MOSCATO (NCT01566019), MATCH-R (NCT02517892), or STING (NCT0493252) trials at Gustave Roussy, Villejuif, France).
Endpoints and evaluation
The primary endpoint was the comparison of OS between the two groups (aged ⩽70 and >70 years), defined as the time between diagnosis of the disease and death or loss to follow-up. Secondary endpoints included comparison of demographics and disease characteristics between the groups, progression-free survival (PFS), overall response rate (ORR), and disease control rate (DCR). PFS was defined as the time between treatment initiation and progression of disease or death, or the date of last follow-up in patients alive without progression. Treatment response was defined using RECISTv1.1: progressive disease (PD), stable disease (SD), partial response (PR), or complete response (CR). DCR was defined as the sum of SD, PR, and CR. 6 Endpoints were described according to the subgroups of patients with resected and unresectable BTC.
In the outcome analysis, survival times (OS and PFS) were compared between the two groups of age (⩽70 and >70 years old). We also performed the same analyses on a subgroup of patients aged over 80 years.
Statistical analysis
Patient and disease characteristics were delineated using mean and standard deviation (SD), median and interquartile range, minimum, and maximum for continuous variables, and frequency and percentage for discrete variables. The comparison of demographics and disease features of patients aged >70 and those aged ⩽70 was conducted using the Wilcoxon test for continuous variables and the Chi-square test or Fisher’s exact test for discrete variables.
Patients were also described as an overall population and in the resected BTC and unresectable BTC groups.
OS, disease-free survival (DFS), and PFS were estimated using the Kaplan–Meier method and reported with median and 95% confidence interval (CI). The survival outcomes between the two age groups were compared using the log-rank test.
The association between parameters and survival was estimated using univariate Cox proportional hazard models, with hazard ratios (HR) and their 95% CIs provided. Parameters with a p-value <0.1 in the univariate analyses were included in a multivariate analysis, followed by a backward selection process, with age forced into the model. For exploratory analyses, all statistical tests were two-sided, and p-values were not adjusted for multiple testing. Statistical significance was considered at p-values <0.05. All analyses were performed using SAS software version 9.3 (SAS Institute, Cary, NC, USA) and R software version 4.1.
Ethics
The ACABI-PRONOBIL cohort was approved by the ethics committee and complies with the French MR004 methodology regarding general data protection regulation for non-interventional retrospective health research (N°ID-RCB: 2021-A00835-36).
The reporting of this study conforms to the STROBE guidelines 20 (Supplemental Table 9).
Results
Patient and disease characteristics
Demographics
In total, 1256 patients with BTC were included in the study. Of these, 665 (53%) were men, with a median age of 64.5 years. Overall, 384 patients (31%) were >70 years old, and 872 patients (69%) were ⩽70 years old. The study flowchart is presented in Figure 1.

Study flowchart.
The general condition of patients aged >70 years was poorer, with a higher proportion having a World Health Organization performance status (WHO PS) of 2 or more, compared with patients aged ⩽70 years (WHO PS ⩾2, 17% vs 8%; p < 0.0001). In addition, they were more likely to have comorbidities, with a higher proportion of patients with one or more comorbidities (⩾1 comorbidity, 89% vs 78%; p < 0.0001). In the subgroup of patients aged >80 years old, 26% of patients had a WHO PS ⩾2, which was significantly higher than patients ⩽80 years old (p < 0.0001), and 94% of patients aged >80 had at least one comorbidity, which was significantly higher than patients aged ⩽80 years (p = 0.0002). The most frequent comorbidities in patients >70 years were diabetes, a second solid cancer, and cardiovascular disease (Supplemental Table 1).
Other baseline patient characteristics were similar between the >70 years group and ⩽70 years group (Table 1).
Patient characteristics.

SD, standard deviation; WHO PS, World Health Organization performance status.
Disease characteristics
Patients aged >70 years were diagnosed more frequently with eCCA and GBC compared with patients aged ⩽70 years (18% vs 12% and 16% vs 13%, respectively, p = 0.0073). Of interest, the older group also had a less-advanced disease stage at diagnosis with less hepatic bi-lobar involvement than the ⩽70 years group (29% vs 37%, respectively, p = 0.0079). There was also a trend for less-advanced tumor–node–metastasis disease stage at diagnosis, but this was not significant (T-stage, p = 0.16; N-stage, p = 0.19; M-stage, p = 0.09). Disease characteristics are summarized in Table 2.
Disease characteristics.
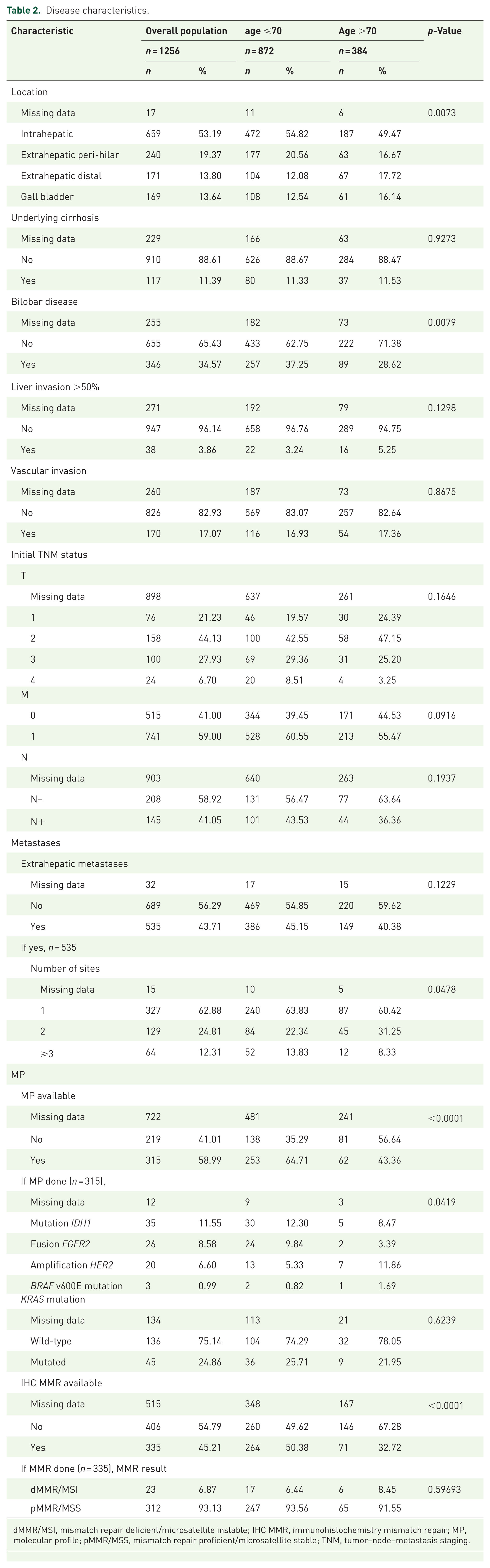
dMMR/MSI, mismatch repair deficient/microsatellite instable; IHC MMR, immunohistochemistry mismatch repair; MP, molecular profile; pMMR/MSS, mismatch repair proficient/microsatellite stable; TNM, tumor–node–metastasis staging.
For patients with resected BTC (n = 362), 247 patients (68%) were ⩽70 years old and 115 (32%) were aged >70. Disease stage was comparable between the two age groups; 100% of patients in both groups had non-metastatic disease (M0) at diagnosis. There was no lymph node involvement (N0) in 71% of the >70 age group versus 61% of patients aged ⩽70 years (p = 0.15). There was no bilobar involvement in 92% of the >70 age group versus 91% of patients aged ⩽70 (p = 0.74). T-stage was also similar between the two groups with a predominance of T2-stage (47% in patients >70 years old and 43% in patients aged ⩽70; p = 0.69; Supplemental Table 2).
For patients with unresectable BTC (n = 894), 625 patients (70%) were ⩽70 years old, and 269 (30%) were aged >70 years. Disease stage was also comparable between the two age groups. In the older group, 213 patients (79%) presented metastatic disease and 56 (21%) presented locally advanced disease versus 528 patients (84%) and 97 (16%), respectively, of patients aged ⩽70 (p = 0.054).
Therapeutic management
Among patients with resected BTC (n = 362), 143 patients (40%) received adjuvant chemotherapy, 106 patients (42%) in the ⩽70 years old group, and 37 patients (32%) in the <70 years old group (p = 0.18). In 46% of resected BTC cases, patients received capecitabine (51% of the older group vs 44% of the ⩽70 years group; p = 0.46; data not shown).
For unresectable BTC (n = 894), patients aged >70 years were less frequently treated with a first-line systemic chemotherapy (87% vs 97%, p < 0.0001). Among patients treated with first-line chemotherapy, regimens differed between the two groups. In patients aged >70 years, gemcitabine monotherapy was more often prescribed (3% vs 0.3%, p = 0.0070), while gemcitabine–cisplatin combined therapy was more often offered to patients aged ⩽70 (35% aged ⩽70 vs 31% aged >70; p = 0.0070). The use of gemcitabine–oxaliplatin combined therapy as a first-line treatment was predominant in our study and similar between the two groups (54%; Table 3).
First-line treatment characteristics.

Similarly, patients aged >70 less often received second-line systemic chemotherapy than patients aged ⩽70 (70% vs 87%, respectively (p < 0.0001)), and the older patients less often received third-line systemic chemotherapy (45% vs 64%, respectively (p = 0.0002)). In patients aged >70, the use of mono-chemotherapy (gemcitabine, 5-FU, or capecitabine) in a second-line setting was more frequent (p < 0.0001). For third-line treatment, there was no significant difference in the chemotherapy regimens used between the two groups (p = 0.24; Supplemental Table 3).
In the subgroup of patients aged >80 years, 72% of patients were treated with first-line chemotherapy, which was significantly lower than for patients aged ⩽80 (97% and 90% for patients aged ⩽70 and patients ages 71–80, respectively, p < 0.0001; Supplemental Table 4). If patients did receive first-line treatment, gemcitabine monotherapy was used for 12% of patients in the >80 years subgroup (vs 0.3% and 1.5% for patients aged ⩽70 and patients aged 71–80, respectively, p = 0.0013).
Molecular profiling
Overall, molecular profiling was less frequent in patients aged >70 years than in patients aged ⩽70 (43% vs 65%, respectively, p < 0.0001; Table 2). The proportions of targetable alterations were significantly different, with more HER2 amplifications, fewer IDH1 mutations, and FGFR2 fusions in patients aged >70 than those aged ⩽70 (p = 0.042; Table 2 and Supplemental Figure 1).
Outcomes
Resected BTC
In the resected BTC group (n = 362), DFS after surgery was similar between patient groups: 15.5 months (95% CI: 10.2–19.6) in patients aged >70 versus 13.8 months (95% CI: 11.9–17.1) for patients aged ⩽70 (p = 0.8836; Figure 2). OS after resection was also similar for both groups of patients: median OS was 47.0 months (95% CI: 37.8–71.9) for patients aged >70 versus 48.8 months (95% CI 41.4–57.3) for patients aged ⩽70 (p = 0.6169; Figure 2). In the multivariate analysis, the HR was 1.18 (95% CI: 0.86–1.62) for OS and 1.03 (95% CI: 0.79–1.34) for DFS, respectively (see Supplemental Tables 5 and 6).

Disease-free survival after resection (a) and overall survival (b) in the resected BTC group.
Unresectable BTC
In the unresectable BTC group, median OS was significantly shorter in patients aged >70 years than patients aged ⩽70 (14.6 months (95% CI 12.7–16.5) versus 17.4 months (95% CI 16.1–18.9), respectively, p < 0.0001; Figure 3). The OS of patients >70 years who received first-line chemotherapy was 15.5 versus 17.5 months for patients aged ⩽70 (p < 0.0001; Supplemental Figure 2). PFS following first-line chemotherapy treatment did not differ between the two groups (median PFS: 6.6 months (95% CI 5.5–7.2) for patients aged >70 years versus 5.8 months (95% CI, 5.3–6.2) for patients aged ⩽70, p = 0.61; Figure 3). In the multivariate analysis, the HR was 1.33 (95% CI: 1.10–1.58) for OS and 0.98 (95% CI: 0.82–1.17) for PFS, respectively (see Supplemental Tables 7 and 8). ORR was 17% and DCR was 49% in patients aged >70 years, and there was no significant difference for patients aged ⩽70: ORR was 22% and DCR was 56% (p = 0.13). In the subgroup of patients aged >80 years, the median OS was significantly lower: 10.5 months (95% CI 9.3–16.7), compared with 15.5 months (95% CI 13.1–17.1) for the patients aged 71–80 years and 17.4 months (95% CI 16.1–18.1) for patients aged ⩽70 (p = 0.0002; Supplemental Figure 3). In the >80 years subgroup, the median PFS following first-line treatment was 6.7 months (95% CI 4.3–7.8) versus 6.6 months (95% CI 5.4–7.6) for patients aged 71–80 years and 5.8 months (95% CI 5.3–6.2) for patients aged ⩽70 (p = 0.87; Supplemental Figure 3).

First-line progression-free survival (a) and overall survival (b) in the unresectable BTC group.
Tolerance
No excessive toxicity was found in patients aged >70 years who received first- and second-line systemic chemotherapy in comparison with patients ⩽70 years old (Table 3 and Supplemental Table 3). Likewise, there was no discontinuation or postponing of treatment due to poor tolerance (Table 3 and Supplemental Table 3). The primary reason for first-line treatment discontinuation was disease progression in nearly 70% of cases, with no significant difference between the two age groups (Table 3).
Discussion
Our study uses the largest cohort to date to specifically examine the management of elderly patients with BTC and is the first with available molecular data for this specific population. In our study, 31% of patients were over 70 years old. These patients exhibited poorer general condition and a higher burden of comorbidities than their younger counterparts. Our investigation identified specific characteristics of BTC in elderly patients. In patients aged >70 years, we observed an overrepresentation of eCCA and GBC, and therefore more frequent HER2 amplification, which is more common in GBC, consistent with the literature.21,22 Also in this older population, we noted a trend of the tumor having a less-advanced stage at diagnosis, which could be explained by less-aggressive disease or perhaps more incidental diagnoses made on imaging performed for another reason.
In patients with resected BTC, RFS and OS were similar between the two groups. This implies that age did not significantly affect prognosis in well-selected patients deemed suitable for surgery. There is little data available in the literature, but older age does not seem to be associated with a worse prognosis for resected BTC. 23 We observed a trend toward more frequent adjuvant chemotherapy in the ⩽70 years old group; this difference was not statistically significant. The trend may be partly due to a generally less favorable postoperative condition among elderly patients, which could reduce their suitability for adjuvant therapy. In addition, the therapeutic impact of adjuvant capecitabine remains modest, 4 making adjuvant therapy a cautiously applied approach. Moreover, elderly patients who undergo surgery are carefully selected, possibly more rigorously than younger patients, in terms of resectability and operability, which may explain the comparable survival outcomes between ⩽70 and >70 years old patients with a resected BTC.
For patients with unresectable BTC, we found that patients aged >70 were less likely to receive first-line systemic chemotherapy and molecular profiling than younger patients. Specifically, the OS of patients aged >70 who had first-line therapy was 15.5 versus 17.5 months for patients aged ⩽70 years. Some factors may explain this result: first, competitive mortality increases with age, with deaths from other causes potentially occurring. Second, a more fragile overall condition in older patients reduces access to second- and third-line chemotherapy, as observed in our study, with death occurring more rapidly following the first line of treatment. However, no significant difference was observed in terms of treatment-related toxicity or dose intensity that could have explained this result. The identical PFS following first-line treatment in the two groups supports the reasoning that, for a well-selected elderly patient population, treatment with chemotherapy is justified and has a benefit comparable to that of younger patients. Our results are consistent with the literature.21,22 In our study, molecular profiling was less frequently performed in patients aged >70 years than in patients aged ⩽70. When it was done, approximately 25% of patients in the >70 years old group had a BTC with a targetable molecular alteration, including 11.9% with HER2 overexpression. As the recruitment period occurred before the availability of targeted therapies in routine clinical practice, it may have impacted molecular profiling completion, particularly elderly patients, who are less often included in therapeutic trials. However, several targeted therapies are now available in current practice,14,15,24,25 in this tumor type with a poor prognosis and a high rate of targetable molecular alteration. Over the past decade, the availability of molecular profiling has expanded with the development of high-throughput sequencing,17,26,27 enabling its recommendation as early as the first line of therapy 3 in patients eligible for a specific treatment and should not be conditioned by age.
With a median age at diagnosis of 76 years in France, 8 BTC is a notable geriatric concern. The population of elderly patients is very heterogeneous and often excluded from therapeutic trials. Because of age-associated comorbidities, general condition, and social factors, standard treatment may not be appropriate. Geriatric assessment and management have clear value in preventing the occurrence of grade 3, or higher, adverse events and in predicting the risk of death,28 –30 particularly in patients with advanced digestive cancers. In addition, it has been shown that there is greater heterogeneity in the management of elderly patients with advanced digestive cancer, and a lack of consistency with recommendations. 31 Geriatric assessment can help to standardize practices, to adapt the management of a “frail” patient, and to avoid under-treatment of “fit” patients. The involvement of a specialized team for geriatric assessment and management is important to ascertain the most appropriate specific treatment and comprehensive patient care. 32 For elderly patients who are not eligible for standard treatment, therapeutic adaptations are required, and the treatment path may result from a discussion between the patient, the geriatrician, and the oncologist. More therapeutic trials specific to this population would enable the production of much-needed guidelines. 33
In our cohort, all ages combined, a striking 94% received first-line systemic chemotherapy. A French study, based on data from the comprehensive “Programme de Médicalisation des Systèmes d’Information” (PMSI) system, indicated that roughly 65% of patients with advanced iCCA never underwent first-line systemic treatment. 34 A major difference in the accessibility of first-line chemotherapy is evident between these findings and our study’s results. A selection bias was introduced in our study because the participating centers in our research were secondary and tertiary centers specializing in the management of BTC; in addition, patients initially treated with best supportive care are less frequent in specialist centers. The data reported by Neuzillet et al. 34 reflect real-life scenarios derived from a PMSI database. Similarly, this selection bias may explain the 30% proportion of patients aged >70 observed in our cohort, which is lower than the approximately 40% typically reported in studies in non-specialist centers. 34 It reflects the highly selective nature of patient recruitment in tertiary centers, where younger and fitter patients are more frequently referred. Consequently, while our findings provide valuable insights into treatment outcomes in well-selected elderly patients, they may not be fully representative of the general population. Furthermore, the low proportion (17%) of patients in the >70 age group with a WHO PS of >2 may also be attributed to this bias, considering that the literature reports a prevalence of approximately 50%. 35
Our study presented some other limitations. It was a retrospective, multicenter study, with the associated information bias and missing data. The recruitment period was long, which can lead to a time-related bias (Supplemental Figure 4). Also, our study was conducted before the era of immunotherapy and targeted therapies in BTC, which may limit the direct applicability of our findings to current treatment practices. These treatments have slightly improved the prognosis of patients today. Our observations regarding molecular tumor profiling to remain relevant, as they provide insight into real-world clinical practices during the study period, and as highlighted above, we believe there is significant value in performing molecular profiling for all patients, including elderly patients. Last, we have few geriatric data regarding our patients, notably no G8 score or geriatric assessment. This highlights the need to set up specific prospective geriatric studies where geriatric assessments would be carried out.
Conclusion
OS was significantly lower in patients >70 years old with unresectable BTC compared to younger patients, highlighting a poorer prognosis in this population. However, the similar first-line PFS suggests that well-selected elderly patients can still benefit from disease-specific treatment, provided they are fit for therapy, ideally with the input of an oncogeriatric team.
For resectable BTC, our study confirms that carefully selected elderly patients achieve survival outcomes comparable to younger patients. Therefore, surgery should remain a treatment option for patients >70 years old after thorough resectability and operability assessment.
Beyond systemic therapy, molecular profiling should be more frequently considered in elderly patients eligible for second-line treatment, as targeted therapies may offer an improved benefit–risk profile compared to chemotherapy.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251344013 – Supplemental material for Management of biliary tract cancers in elderly patients: a French multicenter retrospective study (PRONOBIL-ACABi)
Supplemental material, sj-docx-1-tam-10.1177_17588359251344013 for Management of biliary tract cancers in elderly patients: a French multicenter retrospective study (PRONOBIL-ACABi) by Marine Valery, Julien Edeline, Julie Henriques, Leony Antoun, Heloise Bourien, Antoine Lebeaud, Nadim Fares, Christophe Tournigand, Thierry Lecomte, David Tougeron, Vincent Hautefeuille, Angelique Vienot, Nicolas Williet, Jean-Baptiste Bachet, David Malka, Cristina Smolenschi, Antoine Hollebecque, Jane-Rose Paccard, Maxime Frélaut, Pascal Hammel, Anthony Turpin and Alice Boileve in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank all of the members of the PRONOBIL-ACABI group, the participating patients, and their families.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.