
Abstract
Bladder preservation (BP) has emerged as a clinical alternative to radical cystectomy (RC) for alleviating the substantial physical and psychological burden imposed on localized bladder cancer patients. Nevertheless, disparities persist in the comparative evaluations of BP and RC. We aimed to address the disparities between BP and RC. An umbrella review and meta-analysis were conducted to explore these disparities. We extracted data from meta-analyses and randomized controlled trials (RCTs) selected after searching PubMed, Embase, Web of Science, and the Cochrane Database of Systematic Reviews. Review Manager 5.4.0 and R x64 4.1.3 were used to evaluate the collected data. Our study included 11 meta-analyses and 3 RCTs. In terms of progression-free survival, all the meta-analyses reported that patients with localized bladder cancer who underwent BP exhibited outcomes comparable to those who underwent RC. Meta-analyses regarding the outcomes of cancer-specific survival (CSS) and overall survival (OS) are controversial. To solve these issues, we conducted a pooled analysis of CSS data, which supported the similarity of CSS between BP and RC with no significant heterogeneity [odds ratio (OR): 1.2; 95% confidence interval (CI): 0.71–2.02; I2 = 26%]. Similarly, the pooled OS results extracted from three RCTs indicated the comparability of OS between BP and RC with no significant heterogeneity (OR: 1.12; 95% CI: 0.41–3.07; I2 = 33%). A combination of umbrella review and meta-analysis results suggested that BP had survival rates comparable to those of RC. We suggest that BP may be a more eligible therapy than RC for patients with localized muscle-invasive bladder cancer. This conclusion warrants further validation through randomized controlled trials.
Introduction
As the sixth most common cancer, bladder cancer is the ninth leading cause of cancer death in men.1,2 In China, bladder cancer accounts for over 30,000 annual fatalities. 3 Based on the depth of invasion, bladder cancer is classified into non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC). 4 NMIBC accounts for approximately 70% of newly diagnosed bladder cancer cases. 5 However, approximately 30% of patients diagnosed with NMIBC experience recurrence within 12 months of transurethral resection of bladder tumors and Bacillus Calmette-GuÉRin (BCG) instillation. 6 Patients with NMIBC with frequent recurrence after intravesical instillation are commonly recommended to undergo radical cystectomy (RC). 7 Moreover, both NMIBC and MIBC patients will suffer poor survival outcomes, despite undergoing RC and adjuvant therapy.4,8 Meanwhile, RC causes heavy mental and physical harm to patients who undergo this procedure. 9 Consequently, researchers are striving to find alternatives to mitigate these challenges via various approaches.10,11
Bladder preservation (BP) has been an ongoing practice since the last century and targets patients who either decline RC or are unable to undergo RC due to physical constraints.12,13 Therefore, most studies have selected patients with localized MIBC as the target population. Currently, several treatments are available to achieve BP, including trimodal therapy (TMT), radiation, and chemotherapy alone.14,15 These therapies have demonstrated both efficacy and safety in numerous reports. 16 BP is increasingly used in clinical practice and has garnered positive feedback. Recently, immune checkpoint therapies have shown remarkable efficacy in the management of MIBC. 17 Ongoing RCTs are investigating the integration of immunotherapy with localized MIBC.18 –20 However, discrepancies persist in comparative analyses of survival outcomes between patients with BP and RC. In 2022, Kobayashi et al. 21 reported no statistically significant differences in cancer-specific survival (CSS) or overall survival (OS) between RC and BP based on data from a phase II study. However, in 2021, Zhao et al. 22 demonstrated that patients undergoing RC had significantly better OS and CSS than those receiving BP based on the results of pooled analyses. Furthermore, concerning the comorbidity outcomes, there are some unresolved controversies regarding the relationship between BP and RC. For instance, two meta-analyses23,24 reported a significant association between BP and a higher incidence of grade 3–4 general toxicity. However, Huddart et al. 25 found contrasting results in a multicenter randomized controlled trial (RCT), suggesting a lower incidence of grade 3–4 general toxicity with BP.
In this study, we aimed to address concerns regarding the efficacy of BP for bladder cancer by conducting an umbrella review. Furthermore, we performed a pooled analysis utilizing data from RCTs to reconcile discrepancies noted across different meta-analyses.
Materials and methods
The study was registered with PROSPERO (International Prospective Register of Systematic Reviews, registration number: CRD42023438393) for an umbrella review of meta-analyses comparing the efficacy of BP versus RC, adhering to the Preferred Reporting Items for Systematic reviews and Meta-Analyses guideline. 26 In addition, conflicting results may arise among different meta-analyses. Therefore, we conducted a meta-analysis to reconcile the persisting discrepancies in the comparisons between BP and RC based on the data of RCTs, providing valuable insights into contentious issues. Thus, we synthesized data from RCTs to reconcile disparities observed across various meta-analyses.
Literature search
A systematic search was conducted using PubMed, Embase, Web of Science, and the Cochrane Database of Systematic Reviews to identify pertinent systematic reviews, meta-analyses, and RCTs published until February 2024 (the last update). According to the Scottish Intercollegiate Guidelines Network’s guidance, 27 we conducted a comprehensive literature search on BP by employing a combination of Medical Subject Headings terms, keywords, and various text word variations across multiple databases: (bladder preservation OR chemoradiotherapy OR trimodal therapy OR bladder-sparing strategies OR multimodal therapy) AND (bladder tumor). First, titles and abstracts retrieved from the databases were separately screened by two authors (DXL and DCF). Subsequently, through full-text reading, the two authors selected meta-analyses and RCTs that met the inclusion criteria. Discrepancies in literature screening were resolved by a third author (RCW). Meanwhile, to prevent the omission of relevant literature, a manual search was conducted by a fourth author (QXY) to assess the references of all selected studies.
Study selection
We assessed the comparative efficacy (main survival outcome) between the BP and RC groups. The systematic reviews and meta-analyses included in this study were required to meet the following criteria: they should include RCTs or cohort studies, case–control studies, or cross-sectional studies that compared the efficacy of BP and RC. The RCTs included in this study were also required to meet the following criteria: (a) compared BP and RC, (b) had accurate and available survival benefit data, and (c) the study design was an RCT, with the full text available. Non-English language studies as well as animal and cell culture studies were excluded.
Data extraction
Two reviewers (DXL and DCF) independently extracted the following information from included studies: (a) first author’s name, (b) publication year, number of included studies and patients, estimated summary effect [risk ratio, odds ratio (OR), hazard ratio] with 95% confidence intervals (CIs), and heterogeneity (I²) in (c) survival outcomes [including progression-free survival (PFS), CSS, OS]. Discrepancies were resolved by a third author (RCW). Two reviewers (DXL and DCF) independently extracted the following information from included RCTs: (a) first author’s name and publication year, (b) country of the study, (c) type of BP, (d) phase of RCT, (e) clinical stage of each study, (f) patient numbers for BP and RC, (g) follow-up duration, (h) adjuvant medication in each study, and survival outcomes (including CSS and OS). When an RCT was published both as an article and a conference paper, data from the most recent publication were prioritized for inclusion. Discrepancies were resolved by a third author (RCW).
Quality assessment of methods and evidence
Two reviewers (DXL and DCF) utilized the Risk of Bias in Systematic Reviews (ROBIS) tool 28 to assess the methodological quality of the included meta-analyses. The tool consists of three phases and assigns ratings of low, high, or unclear based on ROBIS criteria. In the final phase, an overall assessment was conducted, categorizing the results of phase II as low risk only if all four domains were classified as low risk; otherwise, it was classified as high risk. In addition, the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) 29 framework was employed to evaluate each outcome and assign a quality grade of ‘high,’ ‘moderate,’ ‘low,’ or ‘very low’.
The Revised Cochrane risk-of-bias tool for randomized trials (RoB 2) tool 30 was employed by two reviewers (DXL and DCF) to assess the quality of the included RCTs. Based on the results, the studies were classified into one of three levels: low risk of bias, some concerns, or high risk of bias. Any disagreements were resolved by a third author (RCW).
Statistical analysis
The data in our study were evaluated using Review Manager 5.4.0 (Cochrane lnformatics & Technology (lT) Services) and R x64 4.1.3 (Vienna University of Economics and Business). We used the mean difference to assess continuous outcomes with 95% CI. Meanwhile, we employed OR to assess dichotomous outcomes with a 95% CI. The p-value of the Q test assessed homogeneity among studies, where a p-value >0.1 and an I² <50% signified no significant heterogeneity. Furthermore, an adjusted profile-restricted maximum likelihood estimator was utilized to calculate the heterogeneity variance tau square (τ²). This metric was preferred because of potential bias in the heterogeneity statistic I² in meta-analyses with small sample sizes.31,32
Results
After removing duplicates, a total of 6609 studies were retrieved from the databases. Following the initial screening, 521 candidate-eligible meta-analyses and 7054 candidate-eligible RCTs were identified. Ultimately, our study included 11 eligible meta-analyses and 3 eligible RCTs (Figure 1).
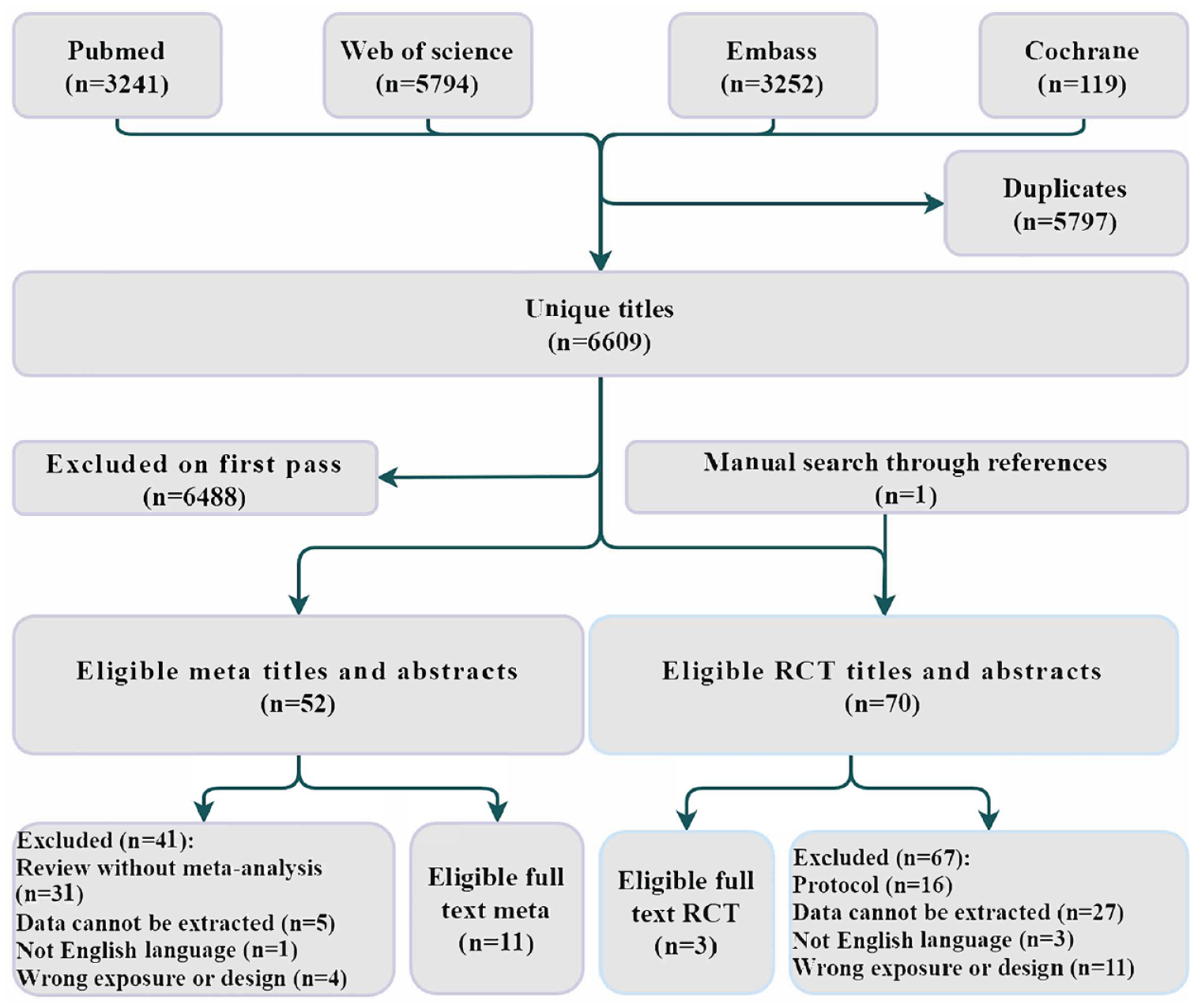
Workflow diagram.
The characteristics of eligible studies and risk of bias assessment
Due to the limited availability of RCTs, all 11 meta-analyses incorporated retrospective studies.22 –24,33 –38 One of the eligible meta-analyses assessed the BP of NMIBC, 37 and the specifics of the 11 meta-analyses are provided in Table 1. The characteristics of eligible RCTs12,21,39 are presented in Table 2. They were conducted in Italy, Egypt, and Japan, respectively. Two trials employed chemoradiotherapy as the intervention for BP, while one utilized methotrexate, vinblastine, doxorubicin, and cisplatin.
Summary of included meta-analyses and outcomes.

BP, bladder preservation; CMT, combined modality treatment; MIBC, muscle-invasive bladder cancer; NRCT, non-randomized controlled trial; RC, radical cystectomy; RCT, randomized controlled trial; TMT, trimodal therapy.
The characteristics of included RCTs.
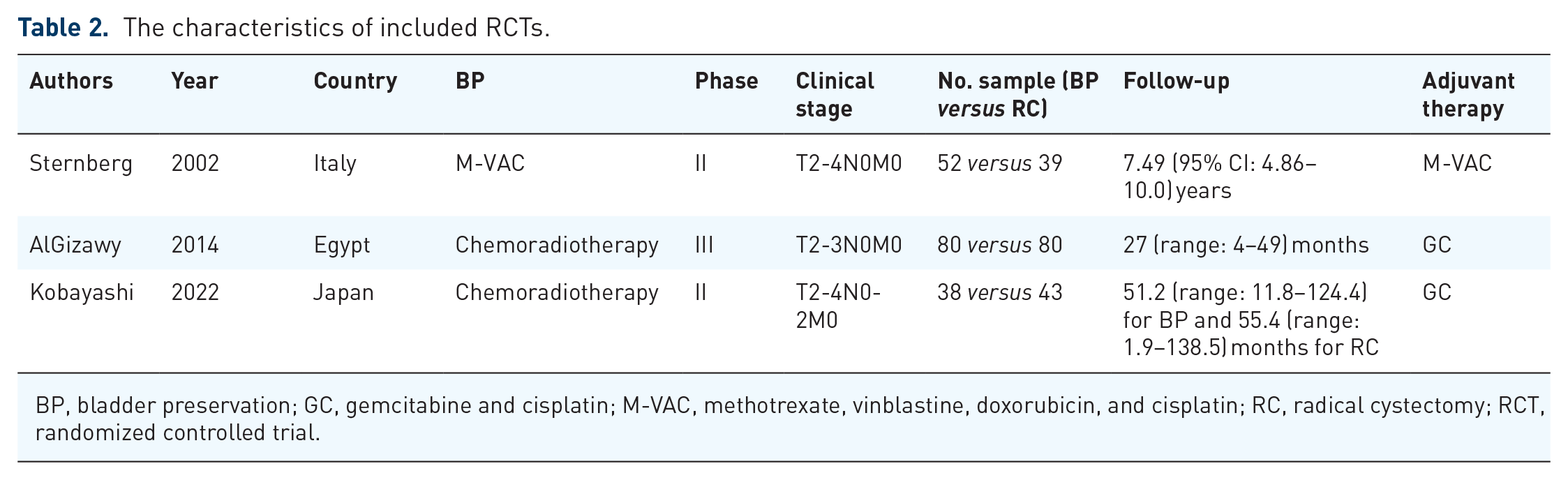
BP, bladder preservation; GC, gemcitabine and cisplatin; M-VAC, methotrexate, vinblastine, doxorubicin, and cisplatin; RC, radical cystectomy; RCT, randomized controlled trial.
Referring to the results of ROBIS, only 5 of 11 (45.5%) meta-analyses were low risk, while the remaining 6 studies (54.5%) were categorized as high risk due to various reasons (Supplemental Table 1). In terms of RCTs, the RoB 2 assessment revealed bias in all three studies, primarily due to the inability to blind the surgical procedure [Figure 2(a)].

Quality assessment of included RCTs (a) and outcomes of CCS and progression-free survival (b).
BP has worse comorbidity and comparable PFS than RC
In this study, all eligible meta-analyses received low or very low grades according to the GRADE results. This was primarily due to the absence of meta-analyses exclusively comprising RCTs. Three studies23,40,41 compared the Charlson Comorbidity Score between BP (which was TMT) and RC. Their pooled outcome revealed that patients who accepted TMT had comparable or worse comorbidity than RC [Figure 2(b)]. In terms of PFS, NMIBC patients treated with BP showed comparable outcomes to those undergoing early RC. Similarly, for MIBC, TMT, and radiation therapy also demonstrated comparable PFS to RC [Figure 2(b)].
BP has a comparable CSS to RC
Divergent findings emerged from different meta-analyses regarding CSS. While all meta-analyses comparing TMT and RC consistently favored RC in terms of CSS, as illustrated in Figure 3(a), Bos et al. 33 also observed superior CSS with RC compared to radiation alone for patients with MIBC. Conversely, Vashistha et al. identified that CMT could offer comparable CSS to patients with MIBC compared to RC. 35 They reported that CMT and RC could bring similar 5- and 10-year CSS. In the context of NMIBC, BP was found to be non-inferior to RC. Shen et al. 37 also reported similar 5- and 10-year CSS rates for BP and early RC in NMIBC patients. Consistently, a meta-analysis 40 indicated that patients who received RC were associated with a better 5- and 10-year CSS compared with those who accepted TMT. We aimed to resolve this dispute by pooling CSS data from RCTs. The pooled results, encompassing two studies that employed TMT as the BP method, indicated similarity in CSS between TMT and RC, with no significant heterogeneity [Figure 3(b); OR: 1.2; 95% CI: 0.71–2.02; I2 = 26%].

The cancer-specific survival results of meta-analyses (a) and the pooled result of cancer-specific survival (b).
BP has a comparable OS to RC
In terms of OS, discrepancies among different meta-analyses were notable. Four studies favored RC over TMT for patients with MIBC,23,38,40,41 while García-Perdomo et al. 36 did not find a significant difference [Figure 4(b)]. Conversely, Arcangeli et al. 34 suggested that TMT might be associated with significantly improved OS compared to RC. In addition, radiation alone appeared to confer better OS compared to RC. Notably, Ding et al. 23 found no significant difference in 5-year OS between TMT and RC, contrary to their pooled OS results. Similarly, another study reported no significant difference in 5- and 10-year OS. 35 Arcangeli et al. 34 reported consistent findings with their pooled OS, suggesting that TMT might be superior to RC for 5-year OS. Zhao et al. 22 suggested that BP might be inferior to RC in terms of 5-year OS, although no such difference was observed in 10-year OS. In another meta-analysis, Al-Qudimat et al. 40 reported that patients who received RC had significantly better 5- and 10-year OS than those who accepted BP. To solve this dilemma, we conducted a pooled analysis of OS data extracted from RCTs, indicating the comparability of OS between BP and RC with no significant heterogeneity [Figure 4(b); OR: 1.12; 95% CI: 0.41–3.07; I2 = 33%]. The GRADE results for each comparison are presented in Supplemental Table 2.
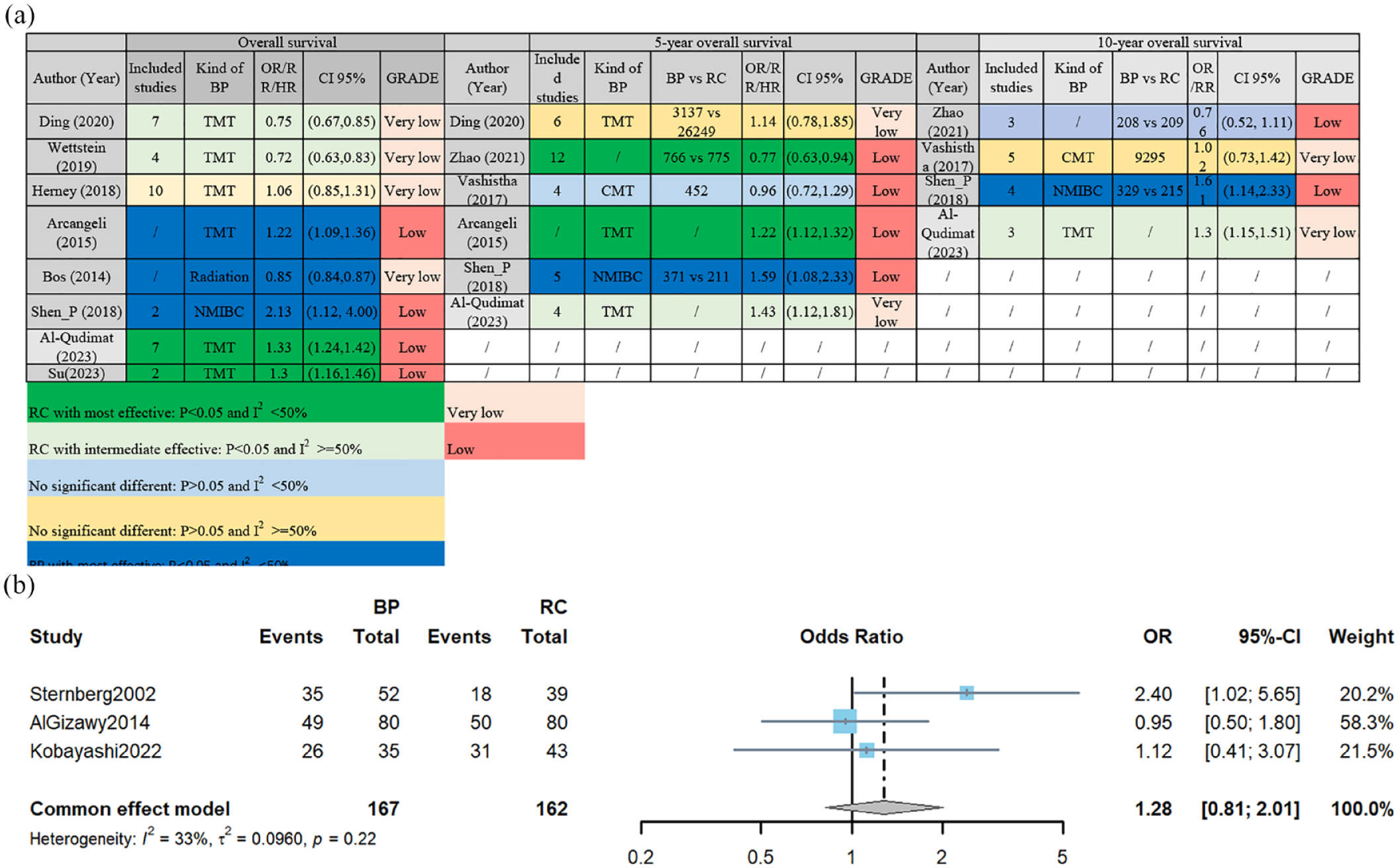
The overall survival results of meta-analyses (a) and the pooled result of overall survival (b).
Discussion
The investigation of BP has persisted since the last century, even though RC is widely established as the standard treatment for MIBC. 12 Divergent findings across studies on BP have resulted in discrepant efficacy outcomes, hindering its smooth integration into clinical practice. 42 In this study, we, for the first time, demonstrated that BP yielded survival outcomes comparable to RC through a combination of umbrella review and meta-analysis.
In terms of comorbidity, Huddart et al. 25 found that patients receiving radiotherapy after neoadjuvant chemotherapy (NAC) had a significantly lower percentage of grade 3–4 general toxicity. Conversely, for TMT, patients undergoing BP were positively associated with grade 3–4 genitourinary toxicity rates. 39 Pooled results from included meta-analyses indicated a significantly higher percentage of grade 3–4 general toxicity among patients undergoing TMT.23,24 Although BP, including TMT, CMT, and radiotherapy alone, may demonstrate inferior efficacy compared to RC, its safety profile is generally considered acceptable. Patients receiving BP tend to have a better health-related quality of life, 43 a finding also supported by included meta-analyses. 24 In addition, BP is associated with fewer social burdens compared to potential adverse effects resulting from RC. Therefore, while a high occurrence rate of grade 3–4 general toxicity should not solely deter the consideration of BP, this drawback should be weighed when formulating personalized treatment plans.
For patients with bladder cancer, survival outcomes are of paramount importance. 44 A variety of treatments have been developed and implemented to prolong the patient’s lifespan, including those targeting genes, 45 materials, 46 single-cell sequencing, 47 natural products, 48 and so on. As society progresses, there is an increasing focus on improving quality of life. BP has emerged as a treatment option for NMIBC and MIBC, offering potential improvements in quality of life and reduced social burdens compared to RC. Particularly in NMIBC, patients often choose BP even after experiencing recurrent episodes or being diagnosed with histological variants.49 –51 Thus, BP could serve as an excellent treatment alternative if it demonstrates comparable survival outcomes to RC. However, the clinical adoption of BP has been hindered by discrepancies in efficacy outcomes observed across different studies. 14
In PFS results, all included meta-analyses consistently reported similar progression rates between patients receiving BP or RC. This finding holds particular significance for patients with NMIBC, as progression to MIBC often necessitates RC, imposing a significant psychological burden. 5 Hence, several RCTs have aimed to evaluate the efficacy of immunotherapies in NMIBC patients with BCG failure, seeking to avoid the need for immediate RC. 18 Fortunately, existing evidence supports the consideration of BP as an initial treatment option for NMIBC patients before contemplating immediate RC. Regarding CSS, four meta-analyses favored RC over BP (including TMT and radiation therapy alone), except for the meta-analysis focusing specifically on NMIBC. Only Vashistha et al. 35 reported that BP was non-inferior to RC in terms of 5- and 10-year CSS. Consistent with these findings, our pooled analysis of RCT data also supported similar CSS outcomes between patients receiving BP and RC. However, it is important to note that Kobayashi et al. 21 included patients who underwent RC simultaneously in their hospital as a control group, which may introduce bias in the results. Therefore, our pooled analysis cautiously suggests the potential efficacy of TMT as a treatment option for localized MIBC.21,39 In terms of OS, the disparity among different meta-analyses was more evident. However, our pooled analysis indicated no significant difference in OS between BP and RC. Notably, Sternberg et al. 12 stratified patients into BP or RC groups based on their response to chemotherapy, potentially introducing bias into the results. Nevertheless, the remaining two studies also reported similar OS outcomes between patients receiving BP and RC. Currently, several RCTs (NCT02710734, NCT01093066) are underway to evaluate the efficacy of BP in localized MIBC. In addition, it is important to highlight the significance of ongoing RCTs (NCT03558087, NCT03775265, SWOGS1806) investigating the integration of immunotherapy with localized MIBC.
Several limitations must be acknowledged. First, subgroup analysis was not feasible due to insufficient data from RCTs, which would be improved in the future when data are enough. Nonetheless, we were able to determine that BP yields comparable survival outcomes to RC. Second, the economic burden comparison between BP and RC could not be conducted due to data limitations. This aspect may warrant further investigation in future studies as more data become accessible.
Conclusion
Combining umbrella review and meta-analysis, the results indicate that BP yields comparable survival outcomes to RC. This suggests that BP may be a viable therapeutic option for patients with localized MIBC compared to RC. However, further validation of this conclusion is warranted through future RCTs.
Supplemental Material
sj-docx-1-tam-10.1177_17588359241249068 – Supplemental material for Efficiency of bladder-sparing strategies for bladder cancer: an umbrella review
Supplemental material, sj-docx-1-tam-10.1177_17588359241249068 for Efficiency of bladder-sparing strategies for bladder cancer: an umbrella review by Deng-xiong Li, Qing-xin Yu, Rui-cheng Wu, Jie Wang, De-chao Feng and Shi Deng in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359241249068 – Supplemental material for Efficiency of bladder-sparing strategies for bladder cancer: an umbrella review
Supplemental material, sj-docx-2-tam-10.1177_17588359241249068 for Efficiency of bladder-sparing strategies for bladder cancer: an umbrella review by Deng-xiong Li, Qing-xin Yu, Rui-cheng Wu, Jie Wang, De-chao Feng and Shi Deng in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.