
Abstract
Objective
Hospital management and medical treatment changed during the coronavirus disease 2019 (COVID-19) pandemic. This study investigated the impact of the COVID-19 pandemic on patients with bladder cancer.
Methods
In this multicenter retrospective study, we collected information from the electronic medical records of outpatients who underwent cystoscopy and inpatients with confirmed bladder cancer in three hospitals in Nanjing (two province-level and one county-level hospitals) in 2019 and 2020. Patients’ home addresses, treatment methods, length of stay, and pathology were compared between the periods.
Results
In total, 4048 outpatients and 1242 inpatients were included. The average number of cystoscopies decreased significantly during the lockdown. In province-level hospitals, the number of cystoscopies increased gradually as the pandemic was brought under control but remained lower than that in 2019, whereas the number grew in 2020 in county-level hospitals. The rates of recurrence and radical cystectomy were higher in 2020 than in 2019. No significant difference in the pathological grade was observed. More patients who underwent radical cystectomy were diagnosed with muscle-invasive bladder cancer during the 2020 lockdown.
Conclusion
The pandemic severely affected patients with bladder cancer, mainly in their choice of institution and treatment.
Introduction
The outbreak of the coronavirus disease 2019 (COVID-19) pandemic prompted an urgent global response, which included restricted travel, limited patient visits to hospitals, and partly closed operating rooms. 1 The impact of COVID-19 on all aspects of the urology department—a department with a high volume of operations—was unprecedented and included changes to adult and pediatric guidelines in response to the pandemic.2–4 During the COVID-19 pandemic, the European Association of Urology guidelines recommended that only high-priority and emergency patients be surgically treated and that all procedures be performed by experienced urologists with a minimum amount of staff. 5
Bladder cancer now ranks ninth among the most common cancers worldwide 6 and is characterized by a high recurrence rate and rapid progression. Cystoscopy is the gold standard for diagnosing bladder tumors and the best way to screen for recurrence. 7 According to the depth of tumor invasion, bladder cancer is divided into non-muscle-invasive bladder cancer (NMIBC) and muscle-invasive bladder cancer (MIBC). The prognosis is considerably worse for patients diagnosed with NMIBC who progress to MIBC than those with “primary” MIBC.8,9 Therefore, timely detection and treatment are vital. However, inexplicably, patients hesitate to see a doctor. For patients with NMIBC, transurethral resection of bladder tumor (TURBT), regular intravesical chemotherapy, and cystoscopic monitoring are the primary treatment options and require frequent hospital visits. 7 Although radical cystectomy (RC) is the recommended surgical treatment for patients with MIBC, the procedure negatively impacts patients’ quality of life. 10 Although many urological operations were postponed during the pandemic, Stensland et al. 11 recommended that surgeons still perform bladder cancer operations such as TURBT for suspected cT1+ bladder tumors, cystectomy for carcinoma in situ refractory to third-line therapy, and cystectomy for MIBC.
It should be noted that the effects of the pandemic have only rarely been reported to date. We analyzed the data from Jiangsu Province Hospital for four equivalent months in 2019 and 2020 and found notable differences in bladder cancer recurrence rates and pathology grades. 12 To further investigate the impact on patients with bladder cancer, we conducted a one-year multicenter retrospective analysis using electronic medical records.
Materials and methods
Study design
In this retrospective study, we collected data from electronic medical records in the urology departments of three hospitals in Nanjing: Jiangsu Province Hospital (Hospital A), a province-level comprehensive Western medicine hospital, Jiangsu Province Hospital of Chinese Medicine (Hospital B), a province-level comprehensive Chinese traditional medicine hospital, and Nanjing Gaochun People's Hospital (Hospital C), a county-level hospital. We further studied outpatients who underwent cystoscopy and inpatients who had been diagnosed with bladder cancer. We defined 23 January 2020—the day the Chinese government announced a lockdown in Wuhan that represented an all-out war on the pandemic—as the start date of the COVID-19 pandemic. We used 30 April 2020 as the mid-point to divide the period between 23 January 2020 and 31 December 2020, when the outbreak was satisfactorily controlled and most schools returned to normal operations. For comparison, we collected data from the same period in 2019, dividing the period into two parts. We collected the following clinical data: patients’ age, sex, home address, initial detection of cancer/recurrence, treatments, pathological grade/stage, time from admission to the first operation, and length of stay.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 13 Because this was a retrospective study in which information was obtained exclusively from electronic medical records, the need for approval was waived by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University. All patients provided written informed consent.
Participant characteristics
All outpatients who underwent cystoscopy were included, and inpatients with hematuria or suspected bladder tumors were eligible for this study. Inclusion criteria were 1) symptoms of hematuria or bladder mass in imaging examinations; 2) definite bladder cancer; and 3) a first round of chemotherapy or immunotherapy after diagnosis. Exclusion criteria were 1) absence of bladder tumor and 2) two or more rounds of chemotherapy or immunotherapy. The workflow is shown in Figure 1.
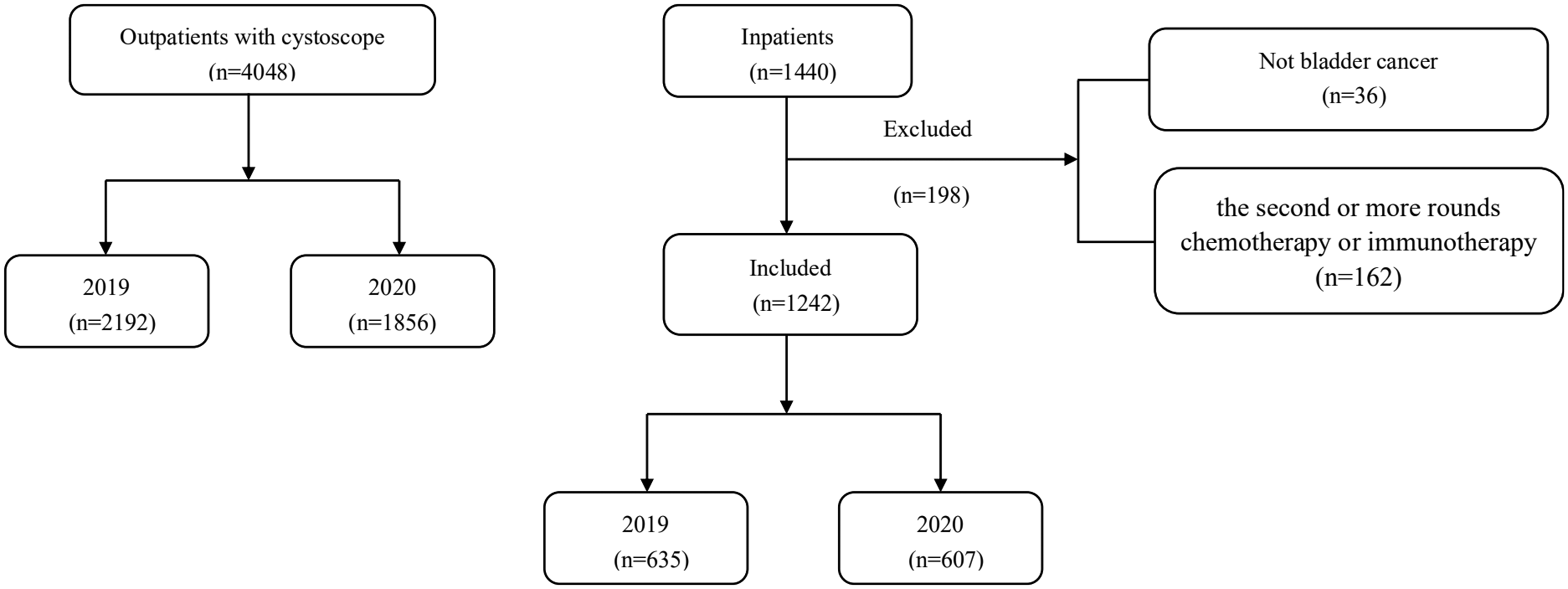
Overview of the workflow.
Statistical analysis
We used an independent-samples t-test to compare measurement data (age, time from admission to first operation, and length of stay) and the χ2 test or Fischer exact test to compare count data (sex, home address, initial/recurrence, treatment, pathological grading, and staging). Statistical significance was set at p < 0.05.
Results
Outpatients
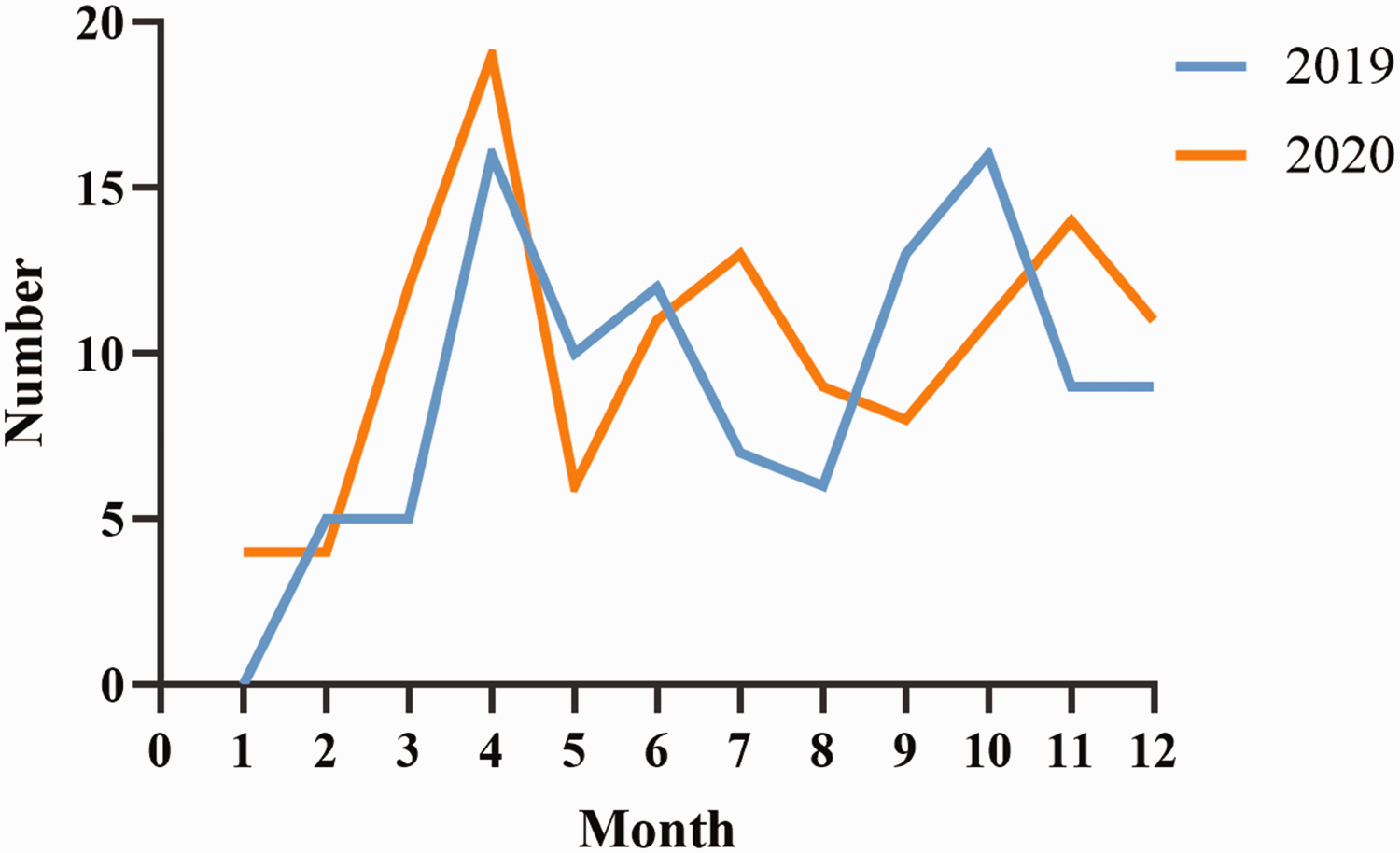
A total of 4048 patients (2192 patients in 2019 and 1856 patients in 2020) were included in the study (Table 1). An overall 15.3% decrease in patients was observed in 2020 compared with the equivalent timeframe in 2019. From 1 January to 30 April 2019, 649 patients underwent cystoscopy, whereas only 386 patients (an overall 40.5% decrease) received the examination during the COVID-19 pandemic in the same period in 2020. The results in Hospital A (46.4% decrease) and Hospital B (46.8% decrease) were consistent. However, an 18.6% increase was observed in 2020 in Hospital C, a county-level hospital. The trend is shown in Figure 2. During the 2020 lockdown, the average monthly number of cystoscopies in Hospital A decreased markedly (135.75 ± 23.96 vs. 72.75 ± 31.98, p = 0.020), whereas the number remained consistent in the control period (157.00 ± 11.84 vs. 157.88 ± 15.25, p = 0.900). The opposite trend was observed in Hospital B, which reported a similar number of cystoscopies during the lockdown and a significant decline during the control period. The details of the centers in which patients underwent cystoscopies are shown in Supplementary Tables 1–3.
Data of outpatients who underwent cystoscopy.


The number of outpatients who underwent cystoscopy in 2019 and 2020 in (a) the three hospitals, (b) Hospital A, (c) Hospital B, and (d) Hospital C.
Inpatients
A total of 1440 cases were included. After checking against the inclusion and exclusion criteria, we ultimately accepted 1242 cases (635 cases in 2019 and 607 cases in 2020). Under strict pandemic prevention and control conditions of 2020, the proportion of patients with local recurrence significantly increased (41.4% vs. 30.1%), and more patients received RC (27.0% vs. 18.1%) compared with the same period in 2019. Under the regular pandemic prevention and control period in 2020, the number of patients who received neoadjuvant chemotherapy followed by RC decreased significantly compared with the same period in 2019 (3.7% vs. 17.9%). However, over the entire year, differences were observed only with neoadjuvant chemotherapy (5.0% in 2020 vs. 19.6% in 2019). The annual RC trend is shown in Figure 3. No notable difference was observed in pathologic T staging. Data for inpatients are shown in Tables 2 and 3 and Supplementary Table 4.
The number of inpatients who underwent radical cystectomy in 2019 and 2020.
Data of inpatients (from January to April).

: some of the untreated were excluded from the statistical analysis. b: includes transurethral resection of bladder tumor, transurethral laser resection, partial cystectomy, and chemotherapy. c: no pathology was excluded from the statistical analysis.
RC, radical cystectomy; NAC, neoadjuvant chemotherapy.
Data of inpatients (from May to December).

: part of the untreated was excluded from statistical analysis. b: includes TURBT, transurethral laser resection, partial cystectomy, and chemotherapy. c: no pathology was excluded from the statistical analysis.
TURBT, transurethral resection of bladder tumor; RC, radical cystectomy; NAC, neoadjuvant chemotherapy.
In Hospital A, more local recurrences (45.5% vs. 32.3%, p = 0.038) and more RC (28.8% vs. 17.5%, p = 0.043) were observed between January and April 2020 than in the same period in 2019. Evidence of recovery was seen after 1 May 2020, with diagnoses returning to expected levels. In Hospital B, also a province-level hospital, the proportion of patients who underwent RC was higher in January to April 2020 (28.1% vs. 16.7%, p = 0.053) than in the same period in 2019, whereas the recurrence rate was similar. However, in Hospital C, a county-level hospital, no difference was observed in any outcome between the two years. The details regarding inpatients across the various centers are shown in Supplementary Tables 5–13.
Discussion
The COVID-19 pandemic spread rapidly worldwide, forcing unprecedented changes in healthcare systems. To support pandemic prevention and control, outpatients were permitted to visit a hospital only if they had no history of travel to endemic areas and no prior contact with patients who tested positive for COVID-19 in the preceding two weeks. 5 All hospitalized patients were required to have a negative COVID-19 nucleic acid test, a negative complete blood count, and C reactive protein results within one week and a negative chest computed tomography scan for virus infection within 1 month. The appropriate department was immediately notified and quarantine measures were instituted if a viral infection was suspected.
Cystoscopy is essential for screening and diagnosing bladder cancer. Because of the lockdown, the number of cystoscopic examinations in major hospitals plunged in 2020, resulting in a failure to detect bladder cancer lesions in time and an increased risk of tumor recurrence or progression. Many studies have demonstrated that the fewer invasive tests are performed, the fewer tumors are diagnosed. 14 The declines in colonoscopy and esophagoscopy led to a persistent reduction in the diagnosis and treatment of colorectal cancer15,16 and esophageal cancer, respectively. 2 Sud et al. 17 reported that delays in surgery for aggressive cancers increased mortality, observing declines in 5-year survival of more than 17% and 30% with delays of 3 and 6 months, respectively. For example, NMIBC for bladder cancer cannot be delayed by 3 to 6 months, and MIBC can progress after more than 12 weeks of delay from diagnosis or the end of neoadjuvant chemotherapy to RC.18,19 Strategic prioritization of patients for screening and diagnosis can mitigate progression attributable to delays. Although we observed that more patients were diagnosed with MIBC from May to December 2020 compared with the same period in 2019, the difference was not significant, potentially because we only included patients with RC because of the difficulty cutting down to the muscular layer in patients who underwent TURBT.
The first symptom of bladder cancer is usually hematuria, to which most patients pay little attention, especially during events such as a pandemic. TURBT combined with chemotherapy is the recommended treatment for NMIBC. Subsequently, patients must undergo cystoscopy every 3 months to monitor cancer recurrence. Compared with the same period in 2019, an overall significant increase in recurrences was observed from January to April 2020 and may have resulted from delays in hospital visits. In addition, COVID-19 infection led to delay in intravesical instillations, especially in patients treated with intravesical instillation of Bacillus Calmette–Guerin. 20 Interestingly, infusion with Bacillus Calmette–Guerin appears to protect patients from COVID-19 infection 21 and is worth further exploration. Importantly, however, patients who experience recurrence should monitor traditionally ignored symptoms such as hematuria, which reminds urological surgeons to disseminate scientific knowledge about urological cancers.
In Hospital A, recurrence and RC rates were significantly higher from January to April 2020 compared with the same period in 2019. As one of the most prestigious comprehensive Western medicine hospitals in Jiangsu Province, Hospital A serves many patients with urological cancer; the number of patients with bladder cancer reached 482 and 475 in 2019 and 2020, respectively. However, the number of cancer patients in Nanjing Gaochun People's Hospital remained at a low level (45 patients in 2019 and 43 patients in 2020). The effect of COVID-19 on cancer was modest in county-level hospitals; most cases were common urological diseases such as urinary stones. Because of the specialty of the Chinese medicine center, the number of patients who underwent surgery there was less affected than in the other centers. In summary, hospitals at different levels have differing roles and undertake distinct yet demanding duties.
RC is the primary surgical treatment for MIBC and high-risk NMIBC.7,10 We observed that more patients chose radical treatment in 2020 than in 2019. Patients must visit the hospital regularly when undergoing conservative treatment such as intravesical chemotherapy, which is inconvenient for patients because of the strict control required. In addition, chemotherapy can lower immunity and increase the risk of pneumonia. 22 However, RC has a higher rate of complications and requires that patients repeatedly visit the hospital. A randomized clinical trial that included 302 patients (150 and 152 patients in the robotic and open cystectomy groups, respectively) found that the most common complications of RC were urinary tract infection and postoperative ileus. 23 Bochner et al. 24 reported that the rates of grades 2 to 5 perioperative complications were 62% and 66% of the robot-assisted group and open cystectomy groups, respectively. Infectious complications were the most common and required patients to visit the hospital for treatment. Therefore, repeated exposure to medical institutions may also increase the risk of COVID-19 infection. A strategy for patients with bladder cancer who receive alternative therapies is worth exploring.
At the beginning of the COVID-19 pandemic, the number of visits and operations in provincial hospitals collapsed, especially in the first month, by 54.9% and 40.5%, respectively. However, these numbers remained consistent in the county hospital. Surprisingly, an increase in the number of patients who underwent cystoscopy was even observed in 2020. Provincial hospitals, which assumed more responsibility for pandemic prevention and control, were disproportionately affected by the pandemic. Balancing COVID-19 pandemic prevention and the management of patients with cancer requires further study. Boehm et al. 25 showed that 84.7% of patients preferred telemedicine during the pandemic, contributing to the further development of telemedicine. Hospital A conducted online consultations from early March 2020. In addition, during the pandemic, patients preferred nearby hospitals, which offered more opportunities for county hospitals. First, pandemic control measures made travel between towns inconvenient for many patients, leading patients to seek medical treatment in local hospitals. Second, avoiding exposure to crowds was a measure to reduce infection risk. Faced with public health emergencies, provincial-level hospitals shouldered the heavy responsibility of controlling the pandemic and county-level hospitals defended the bottom line of basic medical care. Therefore, efforts to enhance comprehensive treatment in county-level hospitals and improve the hierarchical medical system remain crucial. In addition, the application of liquid biopsy for bladder cancer screening is emerging. This rapid and non-invasive strategy may provide more opportunities for patients with bladder cancer. 26 Proton imaging could more accurately predict the grade of cancer, providing help for accurate diagnosis. 27
Our study had some limitations. First, concerning pathological T staging, we only analyzed the patients who had undergone RC. Second, the number of hospitals in the study was limited. Third, the improvement in the level of treatment level and economic strength may also have an impact on patient visits. Fourth, the data were collected using electronic medical records, which may introduce biases inherent to the retrospective design. More studies are worth exploring to inform how to properly manage patients with cancer during a pandemic.
Conclusion
The COVID-19 pandemic had a severe influence on patients with bladder cancer. Bladder cancer progresses rapidly and should be detected and treated promptly, even during a pandemic. The value of regular surveillance of bladder cancer has been demonstrated. To minimize the risk of virus infection, the concept of a non-invasive bladder cancer examination will be pursued. Sex distribution should also be considered when managing patients during a pandemic. Additionally, advancements in the hierarchical medical system and telemedicine may help provide better care for patients with bladder cancer. Increasing the effectiveness of follow-up and popularizing science for patients with tumors is gradually becoming the surgeon's responsibility.
Footnotes
Author contributions
Conception and design: Qiang Lu, Qingyi Zhu, and Wenhui Qian; data acquisition and analysis: Yong Wei, Hongru Zhu, Juntao Zhuang, Lingkai Cai, Qianying Ji, Peng Chen, and Qiang Cao; and manuscript writing: Yong Wei and Xiao Yang. All authors read and approved the final manuscript.
Data availability statement
All data generated or analyzed during this study are included in this published article and its supplementary information files. Further inquiries can be directed to the corresponding authors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research was supported by the National Natural Science Foundation of China (grants No.82072832, 82273152) and the Jiangsu Province Hospital’s (the First Affiliated Hospital of Nanjing Medical University) Clinical Capacity Enhancement Project (JSPH-MC-2021-15).