
Abstract
Background:
Lung cancers are common worldwide. First-line targeted therapy and chemotherapy are both standard treatments in the current guidelines. With the development of new anticancer therapy, the lifespan of patients with late-stage lung cancer has increased. Cardiovascular events can occur during cancer treatment. This observational study aimed to report the incidence of major adverse cardiovascular events (MACE) after cancer treatment using real-world data.
Objectives:
Patients diagnosed with advanced-stage lung cancer between January 2011 and December 2017 were enrolled. Data were collected from the Chang Gung Research Database (CGRD).
Design:
Retrospective cohort study.
Methods:
Baseline characteristics, clinical stages, pathologies, and outcomes were retrieved from the CGRD.
Results:
We identified 4406 patients with advanced lung cancer, of whom 2197 received first-line epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) therapy and 2209 received first-line platinum-based chemotherapy. Most patients in the first-line EGFR-TKI group were never-smokers (74.9%), whereas those in the first-line chemotherapy group were ever-smokers (66.0%). The incidence of MACE was not significantly different between the two groups (12.0% versus 11.9%, p = 0.910). However, the incidence of ischemic stroke was higher in the first-line EGFR-TKI group than in the first-line chemotherapy group (3.9% versus 1.9%, p < 0.001).
Conclusion:
MACEs are common in patients with advanced-stage lung cancer during treatment. The incidence of MACE was similar between the first-line EGFR-TKI therapy and first-line chemotherapy groups. Although more patients in the EGFR-TKI group were female and never-smokers, the risk of ischemic stroke was higher in patients who received first-line EGFR-TKI therapy than in those who received first-line chemotherapy.
Introduction
Lung cancers are common worldwide and sensitive to epidermal growth factor receptor (EGFR) mutations. The prevalence rates of EGFR mutations range from 12.8% to 49.1%. 1 Targeted therapy is the current gold standard for patients harboring EGFR mutations. 2 Gefitinib was found to be better than traditional chemotherapy in large randomized clinical trials.3,4 Targeted therapies, such as erlotinib and afatinib, are the current first-line treatments for patients with lung adenocarcinoma with EGFR mutations.5,6 The third-generation epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI), osimertinib, showed superior efficacy to first-generation EGFR-TKIs in patients with exon 19 deletion and the p.Leu858Arg mutation. 7 In patients with non-small-cell lung cancers (NSCLCs) without driver mutations, immune checkpoint inhibitors, systemic chemotherapy, or combinations are the first-line treatment according to ESMO clinical practice guidelines. 8
In the era of targeted therapy, the life span of patients with late-stage NSCLC has greatly improved. 9 Cardio-oncology is a new field focusing on the detection and treatment of cardiovascular diseases during cancer treatment, while cardio-immuno-oncology focuses on the cardiovascular toxicity of immunotherapy treatments for cancer.10,11 For example, hyperlipidemia is a well-known side effect in patients treated with lorlatinib, an anaplastic lymphoma kinase TKI. 12 Major adverse cardiovascular events (MACE) have also been noted in patients receiving hormonal or immune checkpoint inhibitor therapy.13–15 Patients may have a life-threatening outcome, or their cancer treatment may be withheld if cardiovascular events develop. 16 The European Society of Cardiology (ESC) guideline summarized the potential cardiovascular adverse effects induced by EGFR-TKIs. 17 The guideline recommends baseline cardiovascular risk should be assessed before EGFR-TKI therapies. In the animal study, EGFR-TKIs may cause pathological heart dysfunction and reduce contractility in female mice. 18 The other possible mechanism is related to human epidermal growth factor receptor 2 (HER2), the human epidermal growth factor receptor family. 19 HER2 pathway plays a role in normal cardiac function, and HER2 downstream pathways are important for the survival of heart muscle cells. 20 The cardiovascular adverse events in patients receiving EGFR-TKI may impact heart function by inhibiting the HER2 pathway. 21 Osimertinib is associated with an increased risk of left ventricular ejection fraction reductions. 22 Afatinib targets multiple receptors, including EGFR and HER2. However, the data from clinical trials showed afatinib are not related to cardiac failure. 23 The rationale for major adverse cardiovascular events (MACE) in patients receiving these targeted therapies is not fully understood.
Tammemagi and his colleague found that several comorbidities, such as neurologic disease, congestive heart failure, and peripheral vascular disease were associated with survival in patients with lung cancer. 24 With increasing overall survival of patients with advanced lung cancer, further characterization of major adverse cardiovascular events is needed. This observational study aimed to report the incidence of MACE after advanced-stage lung cancer treatment using a real-world database.
Methods
We conducted a retrospective cohort study at Chang Gung Memorial Hospital, following the Strengthening the Reporting of Observational Studies in Epidemiology.
Subjects
We conducted a retrospective cohort study at Chang Gung Memorial Hospital, following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Conducting a retrospective cohort study using the Chang Gung Research Database (CGRD) allows us to analyze medical data from a large pool of patients treated at several branches of Chang Gung Memorial Hospitals in Taiwan. The CGRD is a valuable resource for researchers as it provides access to de-identified electronic medical records from multiple institutions, enabling a broader scope of investigation (https://www.changgung.hospital/en/about.aspx?id=11&bid=1).25–27 Patients aged >20 years who were diagnosed with advanced-stage (stages IIIB and IV) lung cancer between January 2011 and December 2017 were enrolled in this study. The patient had no history of malignancy. The International Classification of Diseases for Oncology, 3rd edition (ICD-O-3) code for lung cancer is C34 from the Cancer Registry Database of the CGRD. Baseline characteristics, including age, sex, body mass index, smoking history, clinical stage, pathology, performance status, comorbidities, and previous medications, were retrieved from the medical records in the CGRD. Patients who received platinum-doublet chemotherapy and EGFR-TKIs were included in the study. Patients who received targeted therapy other than EGFR-TKIs or single-agent anticancer therapy without platinum were excluded. Patients who did not receive first-line therapy or who used TKI for less than 14 days were excluded. Patients lost to follow-up within 30 days were also excluded. The last follow-up time point included in the study was December 2020. This study was approved by the Institutional Review Board of the Chang-Gung Medical Foundation (CGMH IRB No. 202101057B0C601), and the need for informed consent was waived.
Medication exposure
The index date, also known as the reference date, was defined as the date of initial prescription of the targeted therapy or chemotherapy. Patients were excluded if the difference between the date of medication prescription and the date of lung cancer diagnosis was >3 months. Previous use of cardiovascular medications was assumed whenever there was an order for a prescription of more than 28 days before the index date.
Covariates and outcomes
The patients were divided into two groups: (a) first-line EGFR-TKI therapy and (b) first-line platinum-based chemotherapy (cisplatin or carboplatin). The follow-up period was from the index date until the first occurrence of any of the study outcomes, death, or the end of follow-up (31 December 2020). Covariates for chronic comorbidities were collected from the year before the index day. Comorbidities obtained from the CGRD included atrial fibrillation, hypertension, diabetes, hyperlipidemia, gout, kidney disease, liver disease, chronic obstructive pulmonary disease (COPD), thyroid disease, and cerebrovascular diseases (CVA). Medications for cardiovascular diseases, such as antihypertensive drugs, digoxin, statins, non-vitamin K oral anticoagulants, warfarin, aspirin, clopidogrel, ticagrelor, and diuretics, were included in this study. The primary outcomes, MACE, were cardiovascular (CV) death, myocardial infarction, heart failure, stroke, and arrhythmia. The second outcome was all-cause mortality during the follow-up period. The study outcomes were retrieved from the principal discharge diagnoses and the National Death Registry in Taiwan. The previous studies that have already validated the diagnostic codes for outcomes provide an added level of confidence in the accuracy of the data. 26 The 5-year survival rate for patients with advanced lung cancer is approximately 10% generally. In our opinion, the 6-year follow-up period is sufficient for the detection of the vast MACE.
Statistical analyses
Continuous variables, such as age or body mass index (BMI), were expressed as the mean and standard deviation. To analyze continuous variables, we used the Student’s t-test. Categorical variables were expressed as frequency and percentage and were analyzed using the chi-squared test. The cumulative incidence rates of MACE were plotted using the Fine and Gray method, accounting for the competing risk of non-cardiac death. The Kaplan–Meier method was used to calculate all-cause mortality, and the log-rank test was used to compare between-group differences in the curves. Both the Cox proportional hazards model and the Fine and Gray subdistribution hazard model 28 for the competing risk of non-cardiac death were used to compare the risk of different outcomes between the two groups. The hazard ratios (HRs) of the study outcomes in the first-line chemotherapy group relative to the first-line EGFR-TKI group and the 95% confidence intervals (CIs) were calculated according to the Cox model and Fine and Gray model. The HRs were adjusted by age, sex, BMI, smoking, clinical stage, pathology, Eastern Cooperative Oncology Group (ECOG) performance status, radiation therapy, comorbidities, laboratory data, and previous medication. The purpose of the study is to report the incidence of MACEs using real-world data, and study size calculation is not needed. In the study, statistical significance was defined as a p-value less than 0.05. All the analyses in the study were performed using SAS version 9.4 (SAS Inc., Cary, NC, USA).
Results
During the study period, 4406 patients with advanced lung cancer were identified from the CGRD (Figure 1). Among these patients, 3994 patients (90.6) had NSCLC and 412 patients (9.4%) had small cell lung cancer. We divided the patients into two groups, 2197 received first-line EGFR-TKI therapy (gefitinib, erlotinib, or afatinib), and the other 2209 received first-line platinum-based chemotherapy (cisplatin or carboplatin). The baseline patient characteristics are shown in Table 1. In the EGFR-TKI group, 60% were female and 40% were male. Most patients (85.4%) had stage IV lung cancer. In the EGFR-TKI group, 74.9% of patients were never-smokers. On the other hand, in the chemotherapy group, 66% of patients were ever-smokers. The comorbidities and previous medications of the patients are shown in Table 1. Patients in the EGFR-TKI group had a higher prevalence of hypertension than those in the chemotherapy group (33.9% versus 28.8%). By contrast, more patients in the chemotherapy group had COPD than those in the EGFR-TKI group (15.1% versus 7.8%).

Flow diagram of the study patients.
Baseline characteristics by treatment.
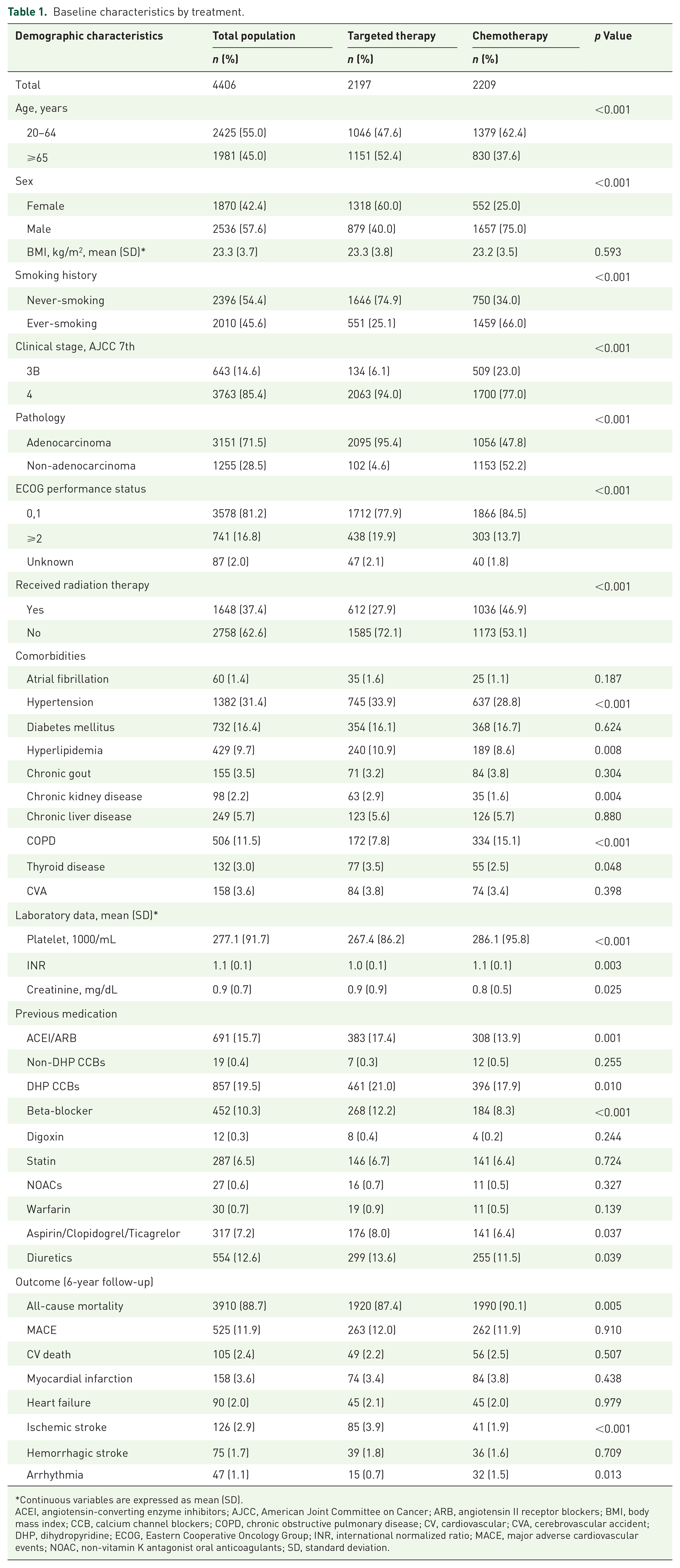
Continuous variables are expressed as mean (SD).
ACEI, angiotensin-converting enzyme inhibitors; AJCC, American Joint Committee on Cancer; ARB, angiotensin II receptor blockers; BMI, body mass index; CCB, calcium channel blockers; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; CVA, cerebrovascular accident; DHP, dihydropyridine; ECOG, Eastern Cooperative Oncology Group; INR, international normalized ratio; MACE, major adverse cardiovascular events; NOAC, non-vitamin K antagonist oral anticoagulants; SD, standard deviation.
As shown in Table 1, there was no significant difference in the incidence of MACE between patients treated with first-line EGFR-TKI therapy and patients treated with first-line chemotherapy. The incidence of CV death, myocardial infarction, heart failure, hemorrhagic stroke, and arrhythmia was similar between the two groups. The incidence of ischemic stroke was significantly higher in the EGFR-TKI group than in the chemotherapy group. The all-cause mortality rate was significantly different between the two groups and most patients (88.7%) died within 6 years of follow-up. The median time to MACE was 18.96 months in the EGFR-TKI group. On the other hand, in the chemotherapy group, the median time to MACE was 10.92 months. The median overall survival in the EGFR-TKI group was 19.92 months. By contrast, in the chemotherapy group, the median overall survival was 11.4 months (Supplemental Table S1).
During the 6-year follow-up study period, the cumulative patient-years for the first-line targeted therapy group was 4492, while for the first-line chemotherapy group, it was 3376. The incidence of MACE was significantly different between the first-line EGFR-TKI therapy group and the first-line chemotherapy group (HR: 1.29; 95% CI: 1.19–1.43, p = 0.041; Table 2). There were no statistically significant differences in the incidence of CV death, myocardial infarction, heart failure, ischemic stroke, hemorrhagic stroke, and arrhythmia between the two treatment groups. In Figure 2, the all-cause mortality rate was significantly higher in the first-line chemotherapy group than in the first-line EGFR therapy group (HR: 1.31; 95% CI: 1.19–1.43, p < 0.001). To mitigate the influence of non-cardiac deaths on MACE, due to the chemotherapy group’s higher mortality rate than the target group in previous years, we employed the Fine and Gray subdistribution hazard model for competing non-cardiac deaths to assess the risks of varying outcomes between both groups. The cumulative incidence of various MACE plotted using the Fine and Gray method are shown in Figure 3. There were no significant differences in the incidence of CV death, myocardial infarction, heart failure, and hemorrhagic stroke between the two groups. However, the incidence of ischemic stroke was significantly higher in the first-line EGFR-TKI group than in the first-line chemotherapy group but the incidence of arrhythmia was significantly lower in the first-line EGFR TKI group than in the first-line chemotherapy group. After adjusting for competing risks (non-CV death), the risk of ischemic stroke was still higher in the first-line EGFR therapy group than in the first-line chemotherapy group (HR: 2.04; 95% CI: 1.18–3.45, p = 0.011, the chemotherapy was as a reference group; Table 2).
Multivariable Cox proportional hazards model analysis of death and MACE in patients treated by chemotherapy and targeted therapy.

HRs were adjusted by age, sex, BMI, smoking, clinical stage, pathology, ECOG, radiation therapy, comorbidities, laboratory data, and previous medication. The targeted therapy was as a reference group.CI, confidence interval; CV, cardiovascular; HR, hazard ratio; MACE, Major adverse cardiovascular events; SHR, subdistribution hazard ratio.

Six-year cumulative incidence curves for (a) MACE adjusted for competing risks of death and (b) all-cause mortality.
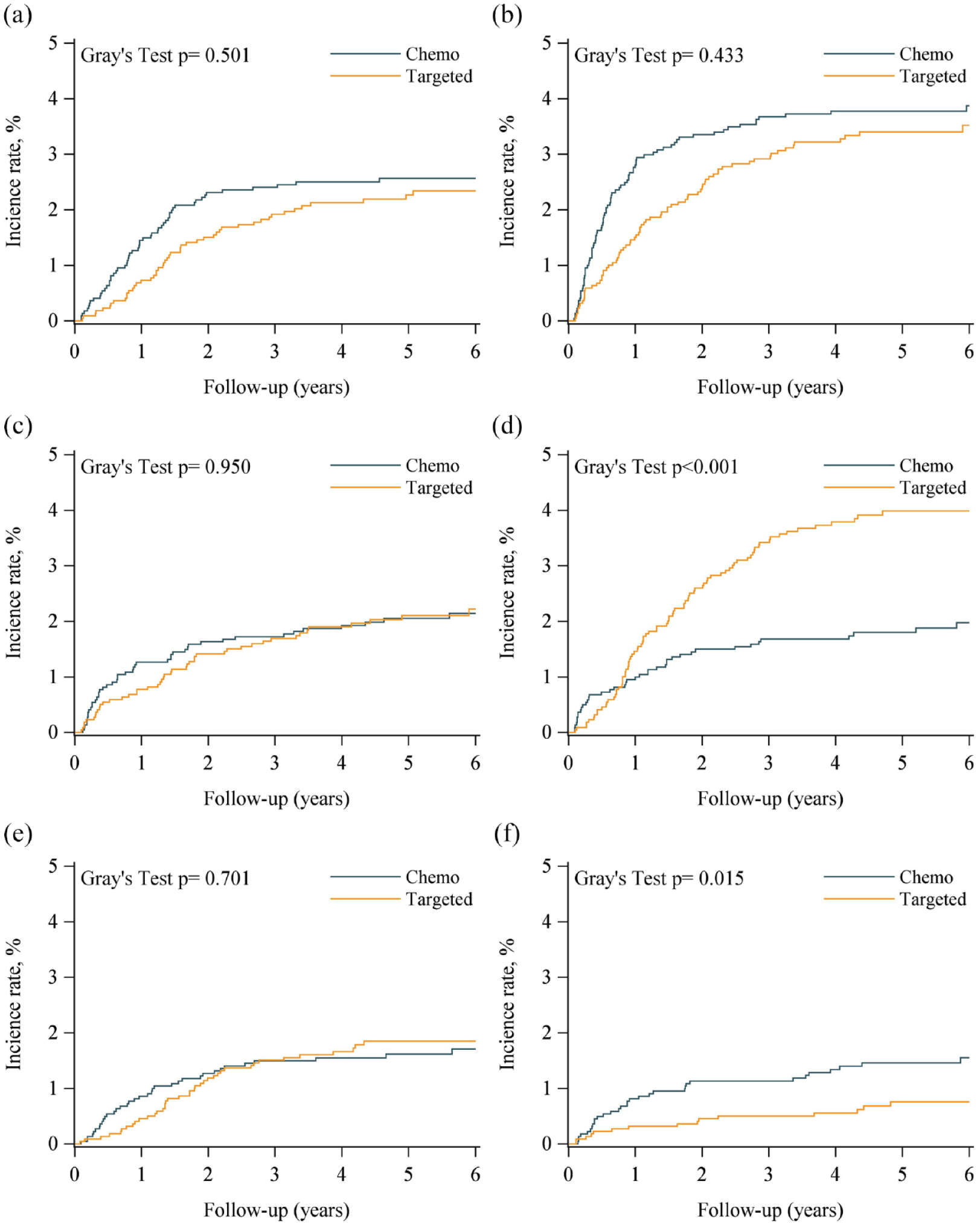
Six-year cumulative incidence curves for (a) cardiovascular (CV) death, (b) myocardial infarction, (c) heart failure, (d) ischemic stroke, (e) hemorrhagic stroke, and (f) arrhythmia adjusted for competing risks of death.
Discussion
In this study, we analyzed real-world data from the CGRD regarding the incidence rates of MACE in patients with advance-stage lung cancer getting different first-line treatments. This study showed that the incidence rate of MACE was 11.9% in patients with advanced-stage lung cancer during anticancer treatment, either first-line EGFR-TKI therapy or first-line chemotherapy.
Platinum-based chemotherapeutic agents such as cisplatin and carboplatin are widely used to treat various types of cancers. Platinum-based chemotherapeutic agents bind to DNA molecules in cancer cells and induce cytotoxicity. This leads to DNA damage and the activation of cell death pathways, ultimately resulting in cancer cell death. 29 However, platinum-based chemotherapy can also damage healthy cells, leading to various side effects including cardiotoxicity. The relationship between cardiotoxicity and chemotherapy is well understood in previous studies.30,31 Cisplatin interferes with the DNA repair mechanism. 31 The mechanisms underlying platinum-based chemotherapy-induced cardiotoxicity include oxidative stress and the potential promotion of thrombosis.32,33 Oxidative stress plays an important role in cardiotoxicity in cancer cisplatin-based chemotherapy. 34 The incidence of cardiotoxicity varies depending on the dose administered; however, it is generally higher in patients with preexisting heart disease or risk factors for cardiovascular disease. 35 With the improvement in the overall survival of patients with lung cancer, MACE, including myocardial infarction, arrhythmias, stroke, heart failure, and cardiac arrest, were also recorded. Symptoms of cardiotoxicity range from mild, such as shortness of breath and fatigue, to severe, such as cardiac arrest.
EGFR-TKIs, such as afatinib, gefitinib, and erlotinib, have shown significant efficacy in the treatment of patients with NSCLC with activating EGFR mutations. However, few studies reported on MACE after cancer therapy in the TKI era. Understanding the risks associated with MACE during anticancer therapy is crucial. Our study reported that 12% of advanced patients with NSCLC who received EGFR-TKIs developed MACE at a median of 18.96 months (interquartile range: 25.44) from lung cancer diagnosis. EGFR-TKI-induced cardiotoxicity has been previously reported. 36 A study conducted at a cancer institute in Japan reported osimertinib-associated cardiac toxicity in a patient cohort. 37 Several mechanisms have been proposed for the cardiotoxicity of EGFR-TKIs, including direct effects on the heart, such as inhibition of the human epidermal growth factor receptor 2 pathway. 38
Gefitinib and erlotinib showed no significant cardiovascular toxicity as reported in a previous study. 39 A systematic review analyzed the adverse effects of EGFR-TKIs and showed that patients treated with second-generation EGFR-TKIs had more high-grade vascular disorders than those treated with first-generation EGFR-TKIs. 40 With third-generation EGFR-TKIs, heart failure with reduced left ventricular ejection fraction developed after osimertinib treatment.41,42 Another study found that patients treated with osimertinib had a higher incidence of heart failure, atrial fibrillation, and QT prolongation than those treated with other EGFR-TKIs. 43 In our database, the number of patients who received osimertinib was relatively small. Further studies using real-world databases should be conducted in the future. Cardiac function evaluation may be required for patients at cardiac risk who are receiving EGFR-TKIs.
Immune checkpoint inhibitor-related cardiotoxicity is uncommon but often fatal. 44 A recent study analyzed MACE after the first immune checkpoint inhibitor (ICI) therapy in lung cancer patients, and 11% of patients had MACE after the first ICI infusion therapy. 45 The incidence of MACE was similar to that observed in the present study.
The ESC guideline recommends baseline cardiovascular toxicity risk assessment before EGFR-TKI therapies. 17 The guideline also suggests electrocardiogram (ECG) and transthoracic echocardiography before osimertinib treatment. Besides, monitoring of magnesium levels and follow-up echocardiography is recommended during osimertinib treatment. Long-term vascular effects and stroke can also be seen in patients treated with cisplatin.46–48 However, in the study, the risk of ischemic stroke was higher in patients who received first-line EGFR-TKI therapy than in those who received first-line cisplatin-based chemotherapy. Lifestyle modification, treatment of underlying cardiovascular conditions, stroke prevention, baseline ECG, and risk factors of atrial fibrillation assessment should be considered.
Cardiovascular disease differences exist not only between countries but also within different ethnic groups. 49 It is a reminder that cardiovascular health is influenced by a complex interplay of genetic, lifestyle, and environmental factors. An observational study enrolled from the United Kingdom Biobank reported that the risks of MACE were different between South Asian and European subjects. 50 A research article reviews 41 studies, and the authors showed that South Asians had higher cardiovascular disease-related mortality than Whites. 51 Ethnicity plays a role in cardiovascular disease risk. The subjects in the study were all Asian populations, and the result should be interpreted for global populations carefully. The MACEs in patients with lung cancer are difficult to predict before EGFR-TKI or other anticancer treatment, but the incidence of MACE is not rare in the study. Besides closely monitoring the MACEs during anticancer treatment, genetic research, and predicting MACEs using artificial intelligence and big data should be conducted in future research in this emergent field of cardio-oncology. Future investigations to mitigate MACEs by personalized risk assessments and early intervention strategies are warranted.
The overall MACE risk was not significantly different between patients in the first-line EGFR-TKI treatment group and those receiving first-line platinum-based chemotherapy in this study. Although more patients in the EGFR-TKI group were female and never-smokers, the risk of ischemic stroke was higher in patients who received first-line EGFR-TKI therapy than in those who received first-line chemotherapy. To minimize the risk of cardiotoxicity in lung cancer patients, physicians may arrange for cardiac testing before treatment to assess baseline heart function and identify any preexisting cardiac conditions that may increase the risk of cardiotoxicity. In addition, patients may be monitored regularly during treatment to detect any signs of cardiac damage or dysfunction and to adjust anticancer therapy individually. Controlling and managing cardiovascular risk factors is crucial in reducing the risk of cardiotoxicity and cardiovascular events in patients with lung cancer. Some common risk factors include hypertension, hyperlipidemia, diabetes, and smoking. Managing cardiovascular risk factors and using cardioprotective medications are essential strategies to reduce the risk of cardiotoxicity in patients with lung cancer. Certain cardioprotective medications, such as ACE inhibitors and beta-blockers, have shown potential cardioprotective effects in patients undergoing cancer treatment.
Limitations
First, because the study is a retrospective observational study, it is challenging to control for all potential confounding variables. We used propensity scores to balance the comorbidities between groups with first-line targeted therapy and chemotherapy. Second, the second-line anticancer therapy varies, the aim of this study is to follow up the MACE in these patients with lung cancer. We did not discuss the second-line anticancer treatment in this study. Third, relying on principal discharge diagnoses to determine study outcomes, such as cardiovascular death, can lead to potential detection bias. Fourth, we were unable to evaluate the compliance of target therapy in a database study.
Conclusion
In conclusion, MACEs are common among patients with advanced-stage lung cancer undergoing anticancer treatment. The incidence of MACE was similar between the first-line EGFR-TKI therapy and first-line chemotherapy groups. Although more patients in the EGFR-TKI group were female and never-smokers, the risk of ischemic stroke was higher in patients who received first-line EGFR-TKI therapy than in those who received first-line chemotherapy. Due to the longer overall survival of patients treated with first-line EGFR-TKIs, doctors should be aware of the risk of MACE after anticancer treatment.
Supplemental Material
sj-docx-1-tam-10.1177_17588359231221907 – Supplemental material for Major adverse cardiovascular events in advanced-stage lung cancer: a multicenter cohort study
Supplemental material, sj-docx-1-tam-10.1177_17588359231221907 for Major adverse cardiovascular events in advanced-stage lung cancer: a multicenter cohort study by Chih-Hao Chang, Shih-Hao Huang, Hung-Yu Huang, Meng-Hung Lin, Chung-Shu Lee, Hsin-Fu Lee, Jason Chia-Hsun Hsieh and Chun-Yu Cheng in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
This study was based in part on data from the Chang Gung Research Database (CGRD) provided by Chang Gung Memorial Hospital. The authors thank the Health Information and Epidemiology Laboratory, Chang Gung Memorial Hospital, Chiayi Branch, for providing comments and assistance with data analysis.
Correction (April 2024):
The author inadvertently added an affiliation in the Methods section, which has now been corrected.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.