
Abstract
Objective
A retrospective single-centre study to compare the clinical features of patients with lung adenocarcinoma with and without epidermal growth factor receptor (EGFR) mutations.
Methods
Pretreatment medical records of patients with lung adenocarcinoma were reviewed. DNA was extracted from paraffin wax-embedded tumour tissue for analysis of EGFR mutations. Malignant pleural effusion (MPE) was diagnosed by cytopathological testing of pleural fluid.
Results
EGFR mutations (19-Del and L858R) were recorded in 81/283 patients (28.6%). MPE was found in 42/283 patients (14.8%). In patients with stage IV disease, the frequency of EGFR mutations was higher in those with MPE than in those without MPE. EGFR mutations were independently associated with female sex, no history of smoking and presence of MPE.
Conclusions
There was a positive association between EGFR mutation and the presence of MPE. EGFR mutations may play an important role in the formation of MPE.
Introduction
Nonsmall cell lung cancer (NSCLC) accounts for around 85% of lung cancers, 1 with lung adenocarcinoma being the most common subtype of NSCLC (at around 40% of cases). 2 Epidermal growth factor receptor (EGFR) mutations occur in the majority of female, nonsmoking Asian patients with lung adenocarcinoma.3,4 The success of EGFR small-molecule tyrosine kinase inhibitors (EGFR-TKIs) in lung adenocarcinoma treatment 5 has allowed the use of EGFR mutation status to select patients who are suitable for first-line therapy with these drugs. 6 The most common EGFR mutations – exon 19 deletion (19-Del) and L858R – can be used to predict response to EGFR-TKI therapy; 7 in addition, EGFR mutations can be used as an indication for EGFR-TKI treatment.8,9
The majority of studies regarding EGFR mutations are related to their role in targeted therapy; little has been addressed concerning the mechanism by which these genetic changes affect (or trigger) particular biological behaviours in cancer cells (such as local invasion, biomarkers and metastasis). Improving our understanding of these mechanisms may be a useful approach for investigating cancer behaviour.
Malignant pleural effusion (MPE) is a common clinical feature in stage IV NSCLC and is associated with poor prognosis. 10 It is estimated that 8–15% of patients with lung cancer have MPE, with higher frequencies observed in those with lung adenocarcinoma, 11 but the mechanism and genetic or epigenetic changes involved in MPE formation are not well understood.
The aim of the present study, therefore, was to compare the clinical features of patients with lung adenocarcinoma, with or without EGFR mutations, in order to determine those factors associated with EGFR mutation.
Patients and methods
Study population
The study retrospectively reviewed medical records of patients with pathologically confirmed lung adenocarcinoma. The patients had been admitted to the Department of Thoracic Surgery, First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China, between July 2010 and July 2012. Data regarding age, sex, clinical stage, smoking history, Eastern Cooperative Oncology Group performance scores (ECOG PS), 12 serum concentrations of carcinoembryonic antigen (CEA) and cytokeratin 19 fragment (Cyfra21-1; both quantified via chemiluminescence enzyme immunoassay), and presence of MPE were extracted from pretreatment medical records. Clinical stage was evaluated by computed tomography (CT) scan of the chest and abdomen, emission computed tomography, skull magnetic resonance imaging and positron emission tomography-CT if possible, as recommended by Union for International Cancer Control (UICC) staging guidelines. 13 MPE was retrospectively confirmed by cytopathological analysis of pleural effusion.
The study was approved by the human ethics committee of the First Affiliated Hospital of Sun Yat-Sen University and all patients provided written informed consent.
Mutation analyses
Detection of EGFR mutations in the primary tumour was performed via an amplification refractory mutation system. 14 Briefly, DNA was extracted from paraffin wax-embedded sections of tumour tissue using a DNA FFPE Tissue Kit (Qiagen, Hilden, Germany). EGFR exon-18, 19, 20 and 21 fragments were amplified and purified via polymerase chain reaction (PCR) with the following primers. Exon 18 forward, 5′-AGGGCTGAGGTGACCCTTGT-3′ and reverse, 5′-TCCCCACCAGACCATGAGAG-3′; exon 19 forward, 5′-ACCATCTCACAATTGCCAGTTAAC-3′ and reverse, 5′-GAGGTTCAGAGCCATGGACC-3′; exon 21 forward, 5′-TCACAGCAGGGTCTTCTCTGTTT-3′ and reverse, 5′-ATGCTGGCTGACCTAAAGCC-3′; and GADPH (internal control) forward, 5′-CCACTCCTCCACCTTTGAC-3′ and reverse, 5′-ACCCTGTTGCTGTAGCCA-3′. 4 The cycling programme involved preliminary denaturation at 95°C for 5 min, followed by 15 cycles of denaturation at 95°C for 25 s, annealing at 64°C for 20 s and elongation at 72°C for 20 s, followed by 31 cycles of denaturation at 93°C for 25 s, annealing at 60°C for 35 s and elongation at 72°C for 20 s. PCR products were purified as described, 15 then analysed using an EGFR Mutation Test kit (AmoyDx, Xiamen, China) for 29 mutation sites in exons 18–21 (including 19-Del, L858R, T790M, 20-Ins, G719X, S768I and L861Q). Quantitative PCR was performed using the LightCycler® 480 (Roche Applied Science, Indianapolis, IN, USA).
Statistical analyses
Data were presented as n (%), median (range) or mean ± SD. Mann–Whitney U-test was used to compare clinical features between patients with and without EGFR mutation, and the differences between cases with and without MPE. Multivariate logistic regression models were applied to estimate odds ratios (OR) and 95% confidence intervals (CI), using EGFR mutations and MPE as dependent variables. All tests were two-tailed, and P-values <0.05 were considered statistically significant. All analyses were performed using SPSS® version 19.0 (SPSS Inc., Chicago, IL, USA) for Windows®.
Results
Demographic and clinical characteristics of patients with lung adenocarcinoma included in a study to investigate the association between epidermal growth factor receptor (EGFR) mutation in tumour tissue and presence of malignant pleural effusion (MPE) (n = 283).
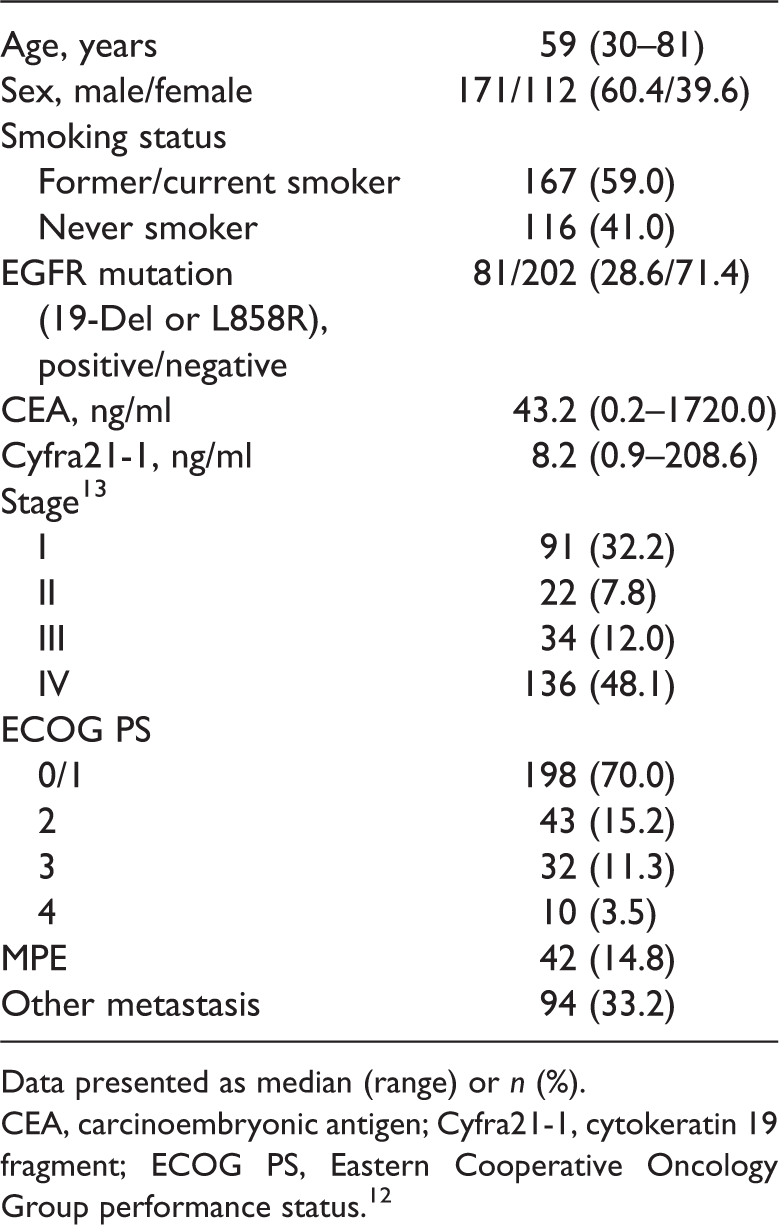
Data presented as median (range) or n (%).
CEA, carcinoembryonic antigen; Cyfra21-1, cytokeratin 19 fragment; ECOG PS, Eastern Cooperative Oncology Group performance status. 12
Demographic and clinical characteristics of patients with lung adenocarcinoma, stratified according to the presence or absence of epidermal growth factor receptor (EGFR) mutation in tumour tissue.

Data presented as median (range) or n (%).
Mann–Whitney U-test.
Cut-off 5 ng/ml.
Cut-off 3.3 ng/ml.
NS, not statistically significant (P ≥ 0.05; Mann–Whitney U-test); CEA, carcinoembryonic antigen; Cyfra21-1, cytokeratin 19 fragment; ECOG PS, Eastern Cooperative Oncology Group performance status; 12 MPE, malignant pleural effusion.
Demographic and clinical characteristics of patients with stage IV lung adenocarcinoma, stratified according to the presence or absence of malignant pleural effusion (MPE).

Data presented as median (range) or n (%).
Mann–Whitney U-test.
Cut-off 5 ng/ml.
Cut-off 3.3 ng/ml.
NS, not statistically significant (P ≥ 0.05; Mann–Whitney U-test); CEA, carcinoembryonic antigen; Cyfra21-1, cytokeratin 19 fragment; ECOG PS, Eastern Cooperative Oncology Group performance status; 12 EGFR, epidermal growth factor receptor.
In multivariate analysis, EGFR mutation was independently associated with female sex (OR 3.705; 95% CI 2.093, 6.559), having never smoked (OR 2.244; 95% CI 1.282, 3.929) and the presence of MPE (OR 2.481; 95% CI 1.087, 5.662). There was no association between EGFR mutation and age, ECOG PS, stage, CEA or Cyfra21-1. Additional multivariate analysis found that the presence of MPE in patients with stage IV disease was significantly associated with EGFR mutation (OR 3.233; 95% CI 1.311, 7.937) but not age, sex, smoking status, ECOG PS, CEA or Cyfra21-1.
Discussion
The present study investigated the relationship between EGFR mutation and selected clinical features of lung adenocarcinoma. These included pretreatment serum concentrations of CEA and CYFRA21-1, which have been shown to predict EGFR-TKI treatment response and survival.16–18 The absence of a statistically significant between-group difference in CEA and CYFRA21-1 concentrations in the present study suggests that other mechanisms besides EGFR mutation may be involved in the relationship between these markers and treatment response.
Studies regarding EGFR mutations have largely focused on advanced-stage lung adenocarcinoma, 4 but tumour behaviour differs widely between the early and advanced stages.19,20 Studies have identified tissue heterogeneity of EGFR mutations,21,22 but it is unknown whether these genetic changes remain stable throughout tumour development. The rate of EGFR mutation in the present study was similar in patients with early stage (I/II) and with advanced stage (III/IV) disease, suggesting that EGFR mutations may be stable during the progression of untreated lung adenocarcinoma. Further studies are required to confirm this hypothesis.
Malignant pleural effusion is a common complication in patients with lung cancer, with a higher incidence occurring in patients with large tumours, mediastinal lymph node involvement and adenocarcinoma.9,23 The cause of MPE is still unclear but it may be ascribed to occlusion of the parietal pleural stomata or obstruction of lymph vessels in mediastinal lymph nodes.24,25 Studies have indicated a high frequency of EGFR mutations in metastatic adenocarinoma cells in MPE,26,27 and an increased frequency of EGFR mutation in the primary tumours of patients with MPE. 15 The causes of MPE are diverse and difficult to understand due to possible differences in genomic status between primary tumours and MPE. 28 Conversely, the heterogeneity of EGFR mutation status in lung cancer suggests that tumours include cancer cells with both mutated and wild-type alleles. A study in Korea comparing EGFR status between paired primary tumour and MPE tissues showed a significant discordance (more mutations in MPE), 26 suggesting that EGFR mutations facilitate the migration of cancer cells into the pleural cavity. The frequency of EGFR mutation in patients with stage IV disease in the present study was significantly higher in those with MPE than in those without, further implicating EGFR mutation in the development of MPE. Further, larger scale studies are required to evaluate the EGFR-TKI treatment response rate in patients with MPE with and without EGFR mutations.
The present study has several limitations. First, the absence of sufficient MPE samples for detection of EGFR mutations meant that comparison of paired MPE and primary tumour samples could not be performed. Secondly, the total EGFR mutation rate was 32.5% (92/283) in the present study, which is lower than the rate reported in other Asian patients with lung adenocarcinoma.3,4 This discrepancy may be a result of bias due to the single-centre nature of our study, and may be resolved by further, multicentre investigations.
In conclusion, the present study findings suggest there is a positive association between EGFR mutations in primary tumours of patients with lung adenocarcinoma and the presence of MPE. EGFR mutations may play an important role in the formation of MPE. Further, large-scale cohort studies are needed to confirm this hypothesis, in addition to the underlying molecular mechanism.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.