
Abstract
Background:
Current standard-of-care first-line treatment of patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) advanced breast cancer (ABC) is cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) + endocrine therapy. In the MONALEESA-2 trial, first-line ribociclib + letrozole demonstrated statistically significant overall survival (OS) benefit versus placebo + letrozole in postmenopausal patients with HR+/HER2− ABC. In the PALOMA-2 trial, first-line palbociclib + letrozole did not show OS benefit versus placebo + letrozole in a similar patient population. Understanding OS outcomes in the respective trials is critical for treatment decisions; however, there are no head-to-head clinical trial data comparing ribociclib and palbociclib.
Objectives:
To conduct a matching-adjusted indirect comparison (MAIC) to compare progression-free survival (PFS) and OS of first-line ribociclib + letrozole versus palbociclib + letrozole in postmenopausal patients with HR+/HER2− ABC.
Design:
Letrozole-anchored MAIC using individual patient data from MONALEESA-2 and published summary data from PALOMA-2.
Methods:
Using individual data, patients from MONALEESA-2 who matched inclusion criteria from PALOMA-2 were selected, and weighting was conducted to ensure baseline characteristics were similar to those in published aggregated data from PALOMA-2. The Bucher method was used to generate corresponding hazard ratios (HRs).
Results:
The final effective sample size compared n = 150 (ribociclib) and n = 112 (placebo) MONALEESA-2 patients with n = 444 (palbociclib) and n = 222 (placebo) PALOMA-2 patients. After matching and weighting, patient characteristics were well balanced. MAIC analysis showed a numerical PFS benefit [HR, 0.80; 95% confidence interval (CI), 0.58–1.11; p = 0.187] and significant OS benefit (HR, 0.68; 95% CI, 0.48–0.96; p = 0.031) with ribociclib + letrozole versus palbociclib + letrozole.
Conclusion:
Results of this cross-trial MAIC analysis showed a numerical PFS benefit and significantly greater OS benefit with first-line ribociclib + letrozole versus palbociclib + letrozole. These results support letrozole + ribociclib as the preferred first-line CDK4/6i for postmenopausal patients with HR+/HER2− ABC.
Trial registration:
NCT01958021; https://www.clinicaltrials.gov/study/NCT01958021 (MONALEESA-2) and NCT01740427; https://clinicaltrials.gov/study/NCT01740427 (PALOMA-2).
Introduction
A cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) combined with endocrine therapy (ET) is the standard-of-care first-line treatment for postmenopausal patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) advanced breast cancer (ABC). 1 In respective phase III trials, three approved CDK4/6is (abemaciclib, palbociclib, and ribociclib) in combination with ET have demonstrated significant improvements in progression-free survival (PFS) over ET alone when used as first-line treament.2–6 However, recent data have shown differences in overall survival (OS) benefits among the three CDK4/6is. In the final OS analysis of MONALEESA-2, first-line ribociclib + letrozole demonstrated significant OS benefit versus placebo + letrozole in postmenopausal patients with HR+/HER2− ABC [hazard ratio (HR), 0.76; 95% confidence interval (CI), 0.63–0.93; p = 0.008]. 7 By contrast, the final OS analysis of PALOMA-2 did not demonstrate OS benefit with palbociclib + letrozole versus placebo + letrozole in a similar first-line setting (HR, 0.96; 95% CI, 0.78–1.18; p = 0.338). 8 An interim analysis of the MONARCH 3 trial demonstrated an OS HR of 0.75 (95% CI, 0.58–0.97; p = 0.030) for abemaciclib + nonsteroidal aromatase inhibitors (NSAIs) versus placebo + NSAIs; however, the prespecified criteria for significance were not met, and as of this writing, the final OS results have not yet been reported.5,9
Demonstrating OS benefit is recognized as the gold standard in oncology clinical trials, clearly surpassing any other end point. 10 Thus, understanding the OS outcomes of the respective CDK4/6i trials in HR+/HER2− ABC is critical to inform treatment decisions. In the absence of head-to-head trial results and the possibility to directly compare within the same trial, a matching-adjusted indirect comparison (MAIC) can be used to evaluate the relative effectiveness of treatments across trials, as it adjusts for known baseline differences in the study populations, unlike unadjusted indirect comparisons. 11 MAIC has been widely used to compare a range of outcomes from phase III clinical trials where no head-to-head study has been available, including among CDK4/6is.12–15 In addition, MAIC has been accepted by several national health technology assessment agencies to help inform decision-making.11,16
In this study, an MAIC was performed to compare both PFS and OS with first-line ribociclib + letrozole versus palbociclib + letrozole using data from the MONALEESA-2 and PALOMA-2 trials. MONARCH 3 (abemaciclib + NSAIs) was not included in the analysis because the currently available interim OS data were still considered immature at the time of this writing.
Methods
Overview
An anchored MAIC of PFS and OS with ribociclib + letrozole versus palbociclib + letrozole as first-line treatment for HR+/HER2− ABC was conducted using individual patient data from the MONALEESA-2 trial (NCT01958021) and aggregated summary data reported for the PALOMA-2 trial (NCT01740427). Data for the MONALEESA-2 PFS and OS analyses were taken from the MONALEESA-2 data cutoff of 10 June 2021. 7 PFS and OS data from PALOMA-2 were used up to the most recently available respective data cutoff of 31 May 2017 and 15 November 2021.8,17 The median follow-up in the MONALEESA-2 trial was 80 months for both PFS and OS, and the median follow-up in the PALOMA-2 trial was approximately 38 and 90 months for PFS and OS, respectively. The study designs and inclusion criteria for both trials have been reported in detail elsewhere.2,4 Patients enrolled in MONALEESA-2 were included in the analysis if they also met the PALOMA-2 inclusion criteria. Patients in both trials were postmenopausal and diagnosed with HR+/HER2− ABC, with no prior treatment for ABC. Baseline characteristics included in the MAIC analysis were age, race, Eastern Cooperative Oncology Group performance status (ECOG PS), liver or lung metastases, number and location of metastatic sites, stage at initial diagnosis, prior surgery, prior radiotherapy, prior (neo)adjuvant chemotherapy, prior adjuvant ET, treatment-free interval (TFI), and geographic region. This trial was conducted in accordance with the provisions of the Declaration of Helsinki and Good Clinical Practice Guidelines.
Statistical analyses
Patients in each arm (ribociclib and placebo) of MONALEESA-2 were matched and weighted separately so that baseline characteristics matched those of patients in the corresponding palbociclib and placebo arms in PALOMA-2. Study designs were generally similar between the studies (Table 1). In MONALEESA-2, patients were stratified by the presence or absence of liver or lung metastases. In PALOMA-2, patients were stratified by visceral versus nonvisceral metastases, prior hormone therapy, and duration of TFI (time from end of (neo)adjuvant treatment to recurrence – referred to as ‘DFI’ in PALOMA-2). Both trials enrolled a similar proportion (18–22%) of patients with a TFI of ⩽12 months.2,4,8,18 Although the inclusion and exclusion criteria for the two trials were generally similar, there were some differences that were reflected in a small subset of patients. These absolute differences were less than approximately 10% for most characteristics, except ECOG PS (Table 2). Therefore, patients from MONALEESA-2 were matched based on inclusion and exclusion criteria for PALOMA-2, and then individual patient data were weighted to match the average baseline characteristics of PALOMA-2 participants. To balance the covariate distribution, patients in one treatment group (MONALEESA-2) were weighted by their inverse odds of being in that group versus the other treatment group (PALOMA-2). The propensity score model was estimated using the generalized method of moments based on the aggregate data and individual patient data. The weights were assumed to follow the logistic regression model:
Comparison of MONALEESA-2 and PALOMA-2 study details.

In PALOMA-2, ‘visceral’ was defined as any lung involvement, which included non-measurable pleura and pleural effusion, in addition to a measurable lung lesion, and/or liver involvement. 20
TFI’ was defined as the time from the end of (neo)adjuvant treatment to recurrence and was referred to as a ‘disease-free interval’ in the PALOMA-2 trial. 18
ABC, advanced breast cancer; PFS, progression-free survival; TFI, treatment-free interval.
Baseline characteristics after matching.

Only one region level (North America) was included to minimize the number of levels to avoid the assignment of extreme weights to patients. North America was chosen to align with a previous MONALEESA-2 MAIC publication. 15
chemo., chemotherapy; ECOG PS, Eastern Cooperative Oncology Group performance status; ET, endocrine therapy; LET, letrozole; MAIC, matching-adjusted indirect comparison; PAL, palbociclib; PBO, placebo; RIB, ribociclib.
PFS and OS with ribociclib + letrozole (from MONALEESA-2) versus palbociclib + letrozole (from PALOMA-2) were compared using time-to-event data. Cox regression models were used to calculate adjusted HRs for PFS and OS for ribociclib + letrozole versus placebo + letrozole before Bucher indirect treatment comparisons were performed to assess ribociclib + letrozole versus palbociclib + letrozole via letrozole. 21 Cox proportional hazards regression is a semiparametric regression technique commonly used to estimate the HR between the two treatment groups when patient-level data are available. The proportional hazards assumption of the Cox regression model states that the HR between any two individuals remains constant over time. In other words, it is assumed that the ratio of the hazard rates for two treatments is constant and does not vary with time. The Bucher method assesses the difference between the treatment group and the placebo group in two different clinical trials – in this case, MONALEESA-2 and PALOMA-2. 21
Results
Patient characteristics
In MONALEESA-2, 334 patients were treated with ribociclib + letrozole, and 334 patients were treated with placebo + letrozole. The MONALEESA-2 patients were matched with 444 patients treated with palbociclib + letrozole and 222 patients treated with placebo + letrozole in PALOMA-2 (Figure 1).

MONALEESA-2 patient selection.
The percentage of patients in the intent-to-treat (ITT) population who received either ribociclib (MONALEESA-2) or palbociclib (PALOMA-2) and had a TFI of ⩽12 months was 17.7% and 22.3%, respectively. Using the variables described in Table 2, the ribociclib and placebo arms were separately matched and weighted; patient characteristics were well balanced after weighting. The ESS was 150 patients for the ribociclib arm and 112 for the placebo arm. Both the ribociclib and palbociclib sample sizes were large enough to provide reasonable results for indirect comparison. Baseline characteristics reported for PALOMA-2 were matched with those reported in ML-2 in the MAIC (Table 2). Rescaled weights ranged from 0 to 5.15 for ribociclib + letrozole (median, 0.72) and from 0 to 12.68 for placebo + letrozole (median, 0.64). The histograms of weight distribution are shown in Figure 2.
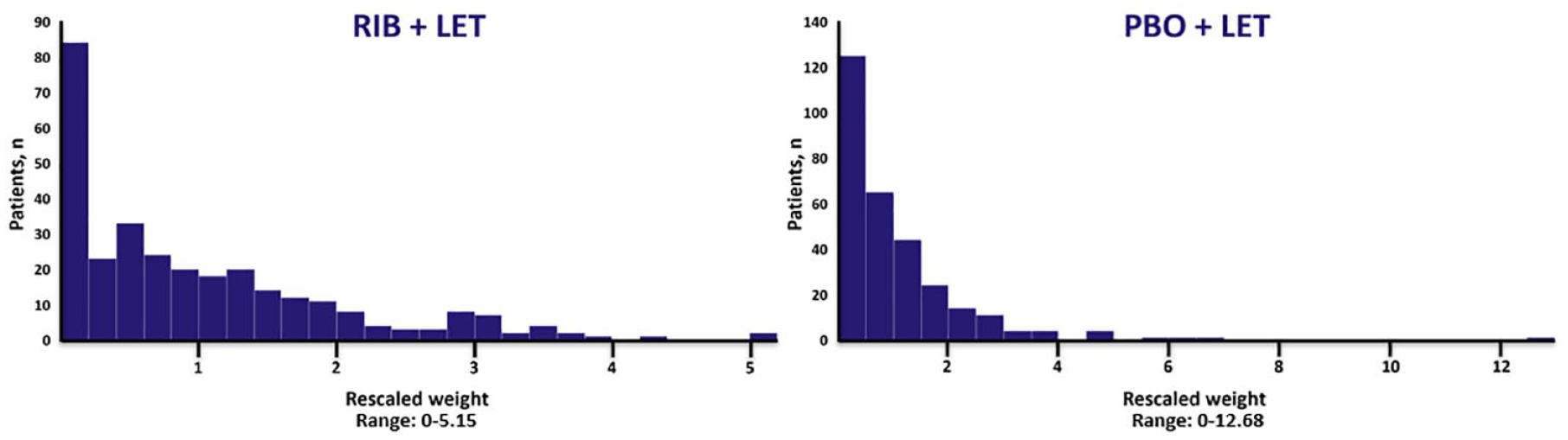
Distribution of weights for patients in MONALEESA-2 who met the PALOMA-2 inclusion criteria in the ribociclib + letrozole and placebo + letrozole arms.
Progression-free survival
The HR estimates for PFS for patients in PALOMA-2 and MONALEESA-2 are shown in Figure 3. The unmatched HR for MONALEESA-2 (based on the ITT population) was 0.58 (95% CI, 0.49–0.70) and significantly (p < 0.001) favored ribociclib + letrozole over placebo + letrozole. After matching and weighting, the MAIC-adjusted HR for ribociclib + letrozole versus placebo + letrozole decreased to 0.45 (95% CI, 0.35–0.58), favoring ribociclib + letrozole over placebo + letrozole (p < 0.001) (based on the ESS). Unadjusted ITT data from the PALOMA-2 trial reported an HR of 0.56 (95% CI, 0.46–0.69), which significantly favored palbociclib + letrozole versus placebo + letrozole (p < 0.001). 17 Comparing MAIC-adjusted HRs for ribociclib + letrozole versus palbociclib + letrozole resulted in a PFS HR of 0.80 (95% CI, 0.58–1.1; p = 0.187).

Forest plot of PFS: ribociclib + letrozole versus palbociclib + letrozole.
Overall survival
The HR estimates for OS for patients in PALOMA-2 and MONALEESA-2 are shown in Figure 4. The data from the MONALEESA-2 trial (based on the ITT population) showed significant OS benefit with ribociclib + letrozole over placebo + letrozole (HR, 0.76; 95% CI, 0.63–0.93; p = 0.008). 7 Similarly, analysis after matching and weighting of MONALEESA-2 patients showed that ribociclib + letrozole had significant OS benefit versus placebo + letrozole. The HR for ribociclib + letrozole versus placebo + letrozole decreased to 0.65 (95% CI, 0.48–0.87; p = 0.004) after MAIC adjustment (based on the ESS). Comparing MAIC-adjusted HRs for ribociclib + letrozole versus palbociclib + letrozole resulted in an OS HR of 0.68 (95% CI, 0.48–0.96), which showed a statistically significant OS benefit with ribociclib + letrozole over palbociclib + letrozole (p = 0.031).

Forest plot of OS: ribociclib + letrozole versus palbociclib + letrozole.
Discussion
This MAIC used matched and weighted individual patient data from MONALEESA-2 and aggregated data from PALOMA-2 to compare PFS and OS with first-line use of ribociclib + letrozole versus palbociclib + letrozole. Results showed that ribociclib + letrozole was associated with a significantly greater OS benefit compared to palbociclib + letrozole as first-line treatment for postmenopausal patients with HR+/HER2− ABC. Although ribociclib + letrozole was also associated with a numerically greater PFS than palbociclib + letrozole, this difference did not reach statistical significance. In these phase III clinical trials, both MONALEESA-2 and PALOMA-2 reported significantly longer PFS in the treatment arms (ribociclib + letrozole or palbociclib + letrozole, respectively) compared with the control arms (placebo + letrozole).2,4 However, while MONALEESA-2 reported significant OS benefit with the addition of ribociclib to letrozole, PALOMA-2 did not demonstrate OS benefit with the addition of palbociclib to letrozole.7,8 It should be noted that when the same TFI definition (time from end of (neo)adjuvant treatment to recurrence – referred to as ‘DFI’ in PALOMA-2) was applied to both trials, the percentage of patients with a TFI of ⩽12 months was not appreciably different between MONALEESA-2 (ribociclib arm, 17.7%; placebo arm, 19.2%) and PALOMA-2 (palbociclib arm, 22.3%; placebo arm, 21.6%). This suggests that differences in the percentage of patients with a TFI ⩽ 12 months were not the reason behind the differences in OS outcomes in MONALEESA-2 and PALOMA-2. Furthermore, the results of this MAIC, which adjusted for patient-level differences (including any slight differences in TFI ⩽ 12 months) between MONALEESA-2 and PALOMA-2, provide additional data to demonstrate the superiority of ribociclib over palbociclib in OS.
The results of the current anchored MAIC analysis are also consistent with a prior unanchored MAIC analysis that compared PFS and OS with first-line ribociclib versus palbociclib, such that there was a numerical PFS benefit and significant OS benefit observed with ribociclib over palbociclib. 14 This previously published MAIC analysis used individual patient data from patients treated with first-line ribociclib + fulvestrant in the phase III MONALEESA-3 trial and palbociclib + letrozole in the phase II PALOMA-1 trial. 14 Although the analysis used a phase II trial (PALOMA-1) with a smaller sample size (and associated limitations on statistical power), the results of this analysis were still consistent with those of the current analysis.
Taken together, the MAIC data presented here, along with data from prior MAIC and primary efficacy analyses, provide meaningful evidence that the CDK4/6is – in this case, ribociclib and palbociclib – are not the same.7,8,14 Preclinical data have shown that ribociclib has greater CDK4 versus CDK6 inhibition; additionally, at clinically relevant doses, ribociclib has higher free drug concentrations than palbociclib.22–25 Clinical data have shown significant OS benefit with ribociclib in prespecified final analyses of all three of its phase III clinical trials in HR+/HER2− ABC (MONALEESA-2: HR, 0.76; 95% CI, 0.63–0.93; p = 0.008; MONALEESA-3: HR, 0.72; 95% CI, 0.57–0.92; p = 0.005; MONALEESA-7: HR, 0.71; 95% CI, 0.54–0.95; p = 0.010).7,26,27 Conversely, palbociclib has not shown significant OS benefit in any prespecified final analysis of its phase III clinical trials in HR+/HER2− ABC (PALOMA-2: HR, 0.96; 95% CI, 0.78–1.18; p = 0.338; PALOMA-3: HR, 0.81; 95% CI, 0.64–1.03; p = 0.09).8,28 Taken together, these data, along with an understanding of the adverse event profiles of each of the two individual agents, can help to inform treatment decisions.
MAIC is a methodology that uses individual patient data from a randomized controlled trial and aggregated data from another trial. This well-accepted technique controls for variations among trials in a statistical manner and provides comparative, clinically meaningful data in instances where head-to-head studies are not feasible. However, this study does include limitations. Biases can occur when comparing nonrandomized treatment groups due to both observed and unobserved differences among trials. 19 Although known differences were accounted for using MAIC, only aggregated characteristics for PALOMA-2 were controlled for in this analysis; therefore, any unreported data may confound the results described in this study. Patients enrolled in PALOMA-2 who had missing survival data were censored at the time of analysis, and unequal distribution of these patients among the matched populations may have led to potential biases in the results. However, baseline characteristics after removing patients with missing data were not available; thus, an MAIC could not be conducted using this cohort of patients. The Bucher indirect treatment comparison method sums the variance of the two trials to generate the CIs that compared ribociclib with palbociclib. The addition of variances may, to some extent, widen the CIs, thus making some relationships that may be significant otherwise become nonsignificant. In particular, the widening of the CIs may have limited the PFS differences observed in this analysis.
Despite some of the limitations mentioned above, anchored MAIC is a validated and widely accepted method for comparing treatments in lieu of head-to-head trials. Analyses such as MAICs can help inform decisions by patients, clinicians, and policymakers. The results from this MAIC show that first-line use of ribociclib was associated with numerically longer PFS and significantly longer OS compared with palbociclib in postmenopausal patients with HR+/HER2− ABC. These results are consistent with and supportive of a now substantial body of evidence that demonstrates clear differences between ribociclib and palbociclib, including differences in OS benefit between the two CDK4/6is. Taken together, these data indicate that ribociclib appears to be preferable over palbociclib as a first-line treatment for postmenopausal patients with HR+/HER2− ABC.
Footnotes
Acknowledgements
We thank the patients who participated in this trial, their families, and their caregivers; members of the data monitoring committee; members of the study steering committee; staff members who helped with the trial at each site; and Kathryn Russo, PhD, of MediTech Media, for medical editorial assistance with this manuscript. Medical writing support and editorial support were paid for by Novartis. We would also like to thank Sina Haftchenary for supporting this study. Ribociclib was discovered by Novartis Institutes for BioMedical Research in collaboration with Astex Pharmaceuticals.