
Abstract
Background:
A cyclin-dependent kinase 4/6 inhibitor (CDK4/6i) + endocrine therapy is recommended as first-line treatment for hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) advanced breast cancer (ABC). Quality of life (QoL) is an important endpoint that affects treatment decisions. Understanding the relevance of CDK4/6i treatment on QoL is gaining importance given use in earlier treatment lines for ABC and an emerging role in treating early breast cancer in which QoL may be more impactful. In the absence of head-to-head trial data, a matching-adjusted indirect comparison (MAIC) permits comparative efficacy between trials.
Objective:
In this analysis, patient-reported QoL for MONALEESA-2 [ribociclib + aromatase inhibitor (AI)] and MONARCH 3 (abemaciclib + AI) was compared using MAIC with a focus on individual domains.
Design:
An anchored MAIC of QoL comparing ribociclib + AI versus abemaciclib + AI was performed using data from the European Organization for Research and Treatment of Cancer quality of life questionnaire (QLQ)-C30 and BR-23 questionnaires.
Methods:
Individual patient data from MONALEESA-2 and published aggregated data from MONARCH 3 were included in this analysis. Time to sustained deterioration (TTSD) was calculated as the time from randomization to a ⩾10-point deterioration with no later improvement above this threshold.
Results:
Patients from the ribociclib (n = 205) and placebo (n = 149) arms of MONALEESA-2 were matched with patients from the abemaciclib (n = 328) and placebo (n = 165) arms of MONARCH 3. After weighting, baseline patient characteristics were well balanced. TTSD significantly favored ribociclib versus abemaciclib in appetite loss [hazard ratio (HR), 0.46; 95% confidence interval (CI), 0.27–0.81], diarrhea (HR, 0.42; 95% CI, 0.23–0.79), fatigue (HR, 0.63; 95% CI, 0.41–0.96), and arm symptoms (HR, 0.49; 95% CI, 0.30–0.79). TTSD did not significantly favor abemaciclib compared with ribociclib in any functional or symptom scale of the QLQ-C30 or BR-23 questionnaires.
Conclusions:
This MAIC indicates that ribociclib + AI is associated with better symptom-related QoL than abemaciclib + AI for postmenopausal patients with HR+/HER2− ABC treated in the first-line setting.
Trial registration:
NCT01958021 (MONALEESA-2) and NCT02246621 (MONARCH 3)
Introduction
All three approved cyclin-dependent kinase 4/6 inhibitors (CDK4/6is; ribociclib, abemaciclib, and palbociclib) reported statistically significant progression-free survival (PFS) benefits in the intent-to-treat (ITT) populations of their phase III trials of patients with hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2−) advanced breast cancer (ABC).1–7 Ribociclib plus endocrine therapy (ET) has demonstrated consistent and statistically significant overall survival (OS) benefits over ET alone in patients with HR+/HER2− ABC throughout its entire phase III program to date, including MONALEESA-2 [hazard ratio (HR), 0.76; 95% confidence interval (CI), 0.63–0.93; p = 0.008], MONALEESA-3 (HR, 0.72; 95% CI, 0.57–0.92; p = 0.00455), and MONALEESA-7 (HR, 0.71; 95% CI, 0.54–0.95; p = 0.00973).8–10 A statistically significant OS benefit was reported for abemaciclib plus ET in the MONARCH 2 trial (HR, 0.757; 95% CI, 0.61–0.95; p = 0.01), while the second interim analysis of the MONARCH 3 trial demonstrated no significant OS benefit (HR, 0.75; 95% CI, 0.58–0.97; p = 0.0301) and final OS results are pending.11,12 No significant OS benefit was observed in either of the phase III trials of palbociclib plus ET, PALOMA-2 (HR, 0.956; 95% CI, 0.777–1.177; p = 0.3378) and PALOMA-3 (HR, 0.81; 95% CI, 0.64–1.03; p = 0.09).12,13 A CDK4/6i + ET is recommended for first-line treatment of HR+/HER2− ABC. 14 To date, ribociclib, in combination with ET, is the only CDK4/6i to demonstrate statistically significant OS benefit over ET alone in the first-line setting.8,10,12
The CDK4/6is are known to have different safety profiles attributed to differences in target inhibition. 15 Treatment-related side effects, even when mild, can impact quality of life (QoL). In support of this, a multi-country, cross-sectional survey of oncologists, nurses, advocates, and patients identified diarrhea, fatigue, and appetite loss as key adverse events that had a moderate to severe impact on QoL among patients treated with CDK4/6is. 16 Many of the trials of CDK4/6is in ABC have reported data on QoL; therefore, understanding the impact of these treatments on QoL is of great importance in clinical decision-making.17–23
No head-to-head study comparing CDK4/6is exists to directly observe the differential effects of these agents on patient QoL. A matching-adjusted indirect comparison (MAIC) is strongly advocated and employed for indirect comparisons in the absence of a direct head-to-head study because it adjusts for differences in the study populations, as opposed to an unadjusted indirect comparison. 24 MAICs have been widely used and accepted by several national health technology assessment bodies across diverse therapeutic areas to estimate relative treatment effects to inform reimbursement decisions. 24
In this analysis, MAIC was performed using patient-reported outcomes from MONALEESA-2 and MONARCH 3, with a focus on individual domains, to compare QoL in patients treated with first-line ribociclib + aromatase inhibitor (AI) versus abemaciclib + AI. The PALOMA-2 trial of first-line palbociclib + AI in a similar patient population used different QoL scales than these studies and hence could not be considered for this analysis. 22
Methods
Overview
An anchored MAIC of QoL with ribociclib + AI versus abemaciclib + AI was performed using patient-reported outcome data from the European Organization for Research and Treatment of Cancer (EORTC) quality of life questionnaire (QLQ-C30) and the breast cancer-specific quality of life questionnaire (QLQ-BR-23) used in the MONALEESA-2 (NCT01958021) and MONARCH 3 (NCT02246621) studies. The EORTC QLQ-30 consists of 30 questions assessing functional scales (physical, social, role, cognitive, and emotional), symptom-related scales (fatigue, nausea/vomiting, pain, dyspnea, sleep disturbances, appetite loss, constipation, and diarrhea), financial impact, and overall QoL or global health status (GHS). GHS is not an aggregate score of the different functional or symptomatic scales, and thus the GHS and specific domains are not directly linked. The EORTC QLQ-BR-23 is a breast cancer-specific module consisting of 23 questions assessing functional scales (body image, sexual functioning, sexual enjoyment, and future perspective) and symptom-related scales [systemic therapy side effects, breast symptoms, arm symptoms (including pain in arm or shoulder, swollen arm or hand, and difficulty in raising arm), and upset by hair loss]. All available QoL data from the studies were used in this analysis.
Individual patient data from MONALEESA-2 (patients were randomized from 24 January 2014 to 24 March 2015; data cutoff, 10 June 2021) and published data from MONARCH 3 (patients were randomized from 18 November 2014 and 11 November 2015; data cutoff, 3 November 2017) were used in this analysis. 21 Inclusion and exclusion criteria were generally similar between the studies (Table 1). The median follow-up for MONALEESA-2 was 79.7 months, and the median duration of follow-up at which QoL data were reported for MONARCH 3 was 26.7 months. Patients in MONALEESA-2 completed questionnaires at the start of each visit: at screening; every 8 weeks for the first 18 months; then every 12 weeks until disease progression, death, loss to follow-up, or withdrawal of consent; and at treatment discontinuation. 17 For MONARCH 3, questionnaires were completed at baseline, every two cycles (cycles 2–19) followed by every three cycles, and approximately 30 days after discontinuation. 21
Comparison of key inclusion/exclusion criteria.

ML-2 allowed TFI ⩽ 12 months if the (neo)adjuvant therapy was tamoxifen.
ABC, advanced breast cancer; BC, breast cancer; CDK4/6; cyclin-dependent kinases 4 and 6; CNS, central nervous system; ECOG, Eastern Cooperative Oncology Group; ET, endocrine therapy; HR+/HER2-, hormone receptor-positive/human epidermal growth factor receptor 2-negative; NSAI, nonsteroidal aromatase inhibitor; QTcF, corrected QT interval by Fredericia’s formula; RECIST, Response Evaluation Criteria in Solid Tumors; TFI, treatment-free interval.
MAIC methods
Both studies enrolled postmenopausal patients with HR+/HER2− ABC to be treated with a CDK4/6i + AI or placebo + AI. MONALEESA-2 and MONARCH 3 have a common comparator arm (placebo + AI); thus, an anchored MAIC was used in this analysis with a focus on the comparison between ribociclib and abemaciclib. Patients in both arms of MONALEESA-2 were weighted by the inverse of their propensity score to balance the covariate distribution with that of the aggregated data of MONARCH 3 (Figure 1). Distributions of inverse probability of treatment weights for patients in MONALEESA-2 were plotted as histograms (Figure 2), and effective sample sizes were calculated.

MONALEESA-2 patient selection. ESS reflects sample size after balancing.
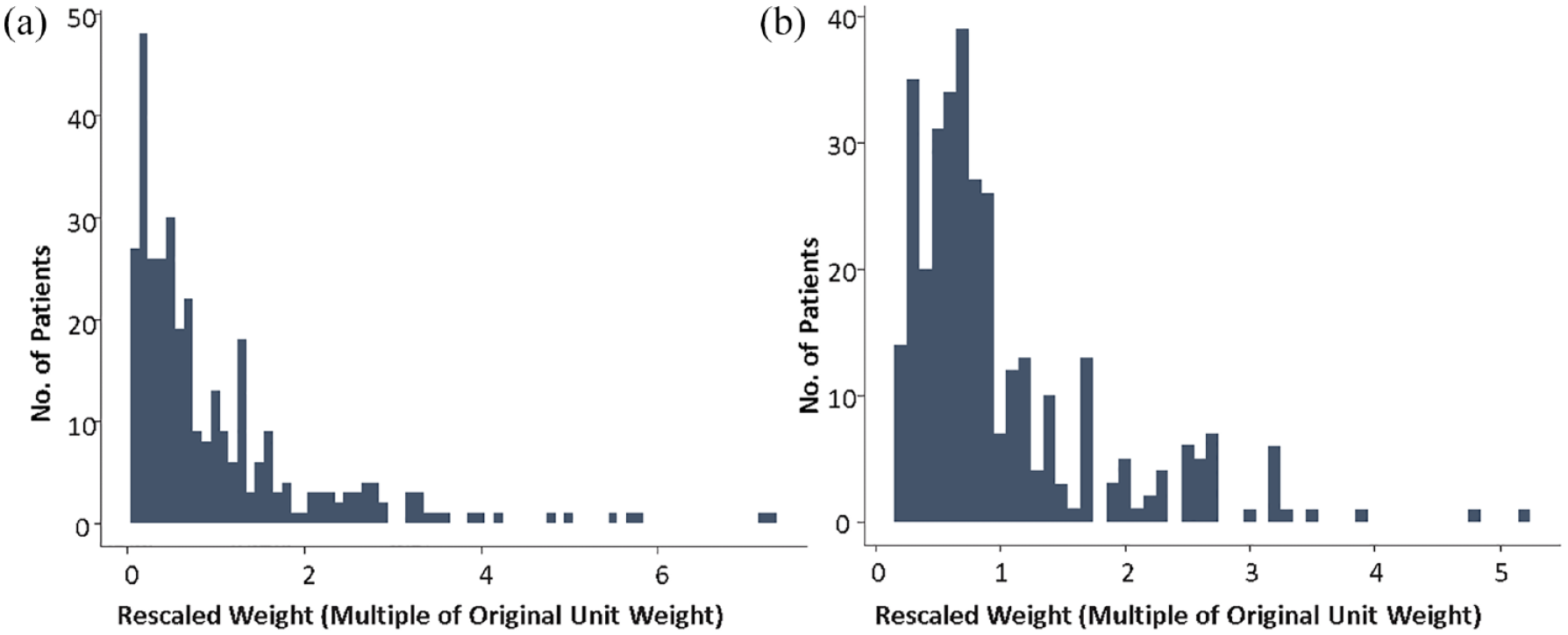
Distribution of MAIC weights for patients in MONALEESA-2 meeting the inclusion criteria for MONARCH 3 in the placebo + AI and ribociclib + AI arms.
Statistical analysis
A Cox proportional hazards model was used to generate HRs; anchored HRs were calculated using the Bucher method. A QoL deterioration of ⩾10 points in the EORTC QoL scales has historically been considered clinically meaningful. In this analysis, time to sustained deterioration (TTSD) was calculated as the time from randomization to a ⩾10-point deterioration in scale scores relative to baseline with no later improvement above this threshold observed during the treatment period or death due to any cause. If a patient had ⩾10-point deterioration followed by improvement, they would be censored and not counted for TTSD. However, if a patient improved after ⩾10-point deterioration, but afterwards had ⩾10-point deterioration again with no further improvement, this second deterioration would be considered for TTSD.
Results
In total, 205 patients treated with ribociclib + AI and 149 patients treated with placebo + AI in MONALEESA-2 were matched with 328 patients treated with abemaciclib + AI and 165 patients treated with placebo + AI in MONARCH 3 (Figure 1 and Table 2). Treatment and placebo arms were matched separately. After weighting, patient characteristics were well balanced (Figure 2 and Table 2). Rescaled weights for patients in MONALEESA-2 who matched the inclusion criteria for MONARCH 3 ranged from 0.06 to 7.33 for the placebo arm and 0.16 to 5.16 for the ribociclib arm, with a median of 0.7 for ribociclib + AI and 0.6 for placebo + AI (Figure 2). The effective sample size was 205 for the ribociclib arm (sample size reduction of 39% from the ITT) and 149 for the placebo arm (reduction of 55%). None of the baseline characteristics reported for MONARCH 3 were removed from the analysis.
Characteristics of patients in MONALEESA-2 and MONARCH 3 meeting the inclusion criteria of MONARCH 3.

ABE, abemaciclib; AI, aromatase inhibitor; ECOG PS, Eastern Cooperative Oncology Group performance status; ET, endocrine therapy; ML-2, MONALEESA-2; MON-3, MONARCH 3; PBO, placebo; PR, progesterone receptor; RIB, ribociclib.
With respect to symptom scales, TTSD analysis significantly favored ribociclib + AI over abemaciclib + AI in four symptom scales ( Figure 3 ): appetite loss (HR, 0.46; 95% CI, 0.27–0.81), diarrhea (HR, 0.42; 95% CI, 0.23–0.79), fatigue (HR, 0.63; 95% CI, 0.41–0.96), and arm symptoms, including pain in arm or shoulder, swollen arm or hand, and difficulty raising arm (HR, 0.49; 95% CI, 0.30–0.79). TTSD analysis numerically favored ribociclib + AI over abemaciclib + AI in three symptom scales (Figure 3): dyspnea (HR, 0.60; 95% CI, 0.34–1.07), pain (HR, 0.73; 95% CI, 0.46–1.16), and systemic treatment side effects (HR, 0.89; 95% CI, 0.55–1.44). No significant differences were observed in any of the EORTC QLQ-C30 or BR-23 functional domains ( Figure 3 ), including GHS (HR, 1.03; 0.61–1.75). However, the TTSD analysis numerically favored ribociclib + AI over abemaciclib + AI in emotional (HR, 0.77; 95% CI, 0.45–1.32), role (HR, 0.66; 95% CI, 0.41–1.06), and social (HR, 0.80; 95% CI, 0.49–1.31) functioning, as well as body image (HR, 0.82; 95% CI, 0.47–1.44), future perspective (HR, 0.61; 95% CI, 0.34–1.08), and sexual functioning (HR, 0.50; 95% CI, 0.24–1.01) (Figure 3). Notably, the TTSD analysis did not significantly favor abemaciclib + AI over ribociclib + AI in any functional or symptom scale of the QLQ-C30 or BR-23 but did numerically trend in favor of abemaciclib + AI in financial difficulties (HR, 1.13; 95% CI, 0.60–2.14) and breast symptoms (HR, 1.26; 95% CI, 0.62–2.55).

TTSD in functional (a) and symptom (b) scales for ribociclib + AI versus abemaciclib + AI.
Discussion
This MAIC used matched and weighted individual patient data from MONALEESA-2 and published data from MONARCH 3 to compare QoL with first-line use of ribociclib + AI versus abemaciclib + AI. Results showed that the TTSD analysis significantly favored ribociclib + AI over abemaciclib + AI in diarrhea, fatigue, appetite loss, and arm symptoms. Although not statistically significant, the TTSD analysis favored ribociclib + AI over abemaciclib + AI in emotional, role, and social functioning, as well as body image, future perspective, and sexual functioning. The TTSD analysis did not significantly favor abemaciclib over ribociclib in any of the functional or symptom scales, but TTSD for constipation, physical functioning, financial difficulties, nausea/vomiting, and breast symptoms trended numerically in favor of abemaciclib. Similar to the current MAIC, a previously published MAIC evaluated QoL with second-line use of palbociclib + fulvestrant versus abemaciclib + fulvestrant using data from PALOMA-3 and MONARCH 2. 25 That MAIC found that abemaciclib was associated with significantly greater impact on several symptom scores, including diarrhea and appetite loss, compared with palbociclib. While previously published QoL data from MONARCH 3 did not demonstrate a meaningful difference between the abemaciclib and placebo arms in most symptoms with the exception of diarrhea, 21 data from these MAICs shed light on the impact of AEs associated with abemaciclib on patient QoL relative to other CDK4/6is.
Both MONALEESA-2 and MONARCH 3 reported significant improvements in PFS in their ITT populations, and MONALEESA-2 demonstrated a significant >12-month improvement in OS with ribociclib + ET versus placebo + ET, with a 24% relative reduction in the risk of death.1,7,8 No significant OS benefit with abemaciclib + ET was observed in the second interim analysis of MONARCH 3, and final OS data are still pending at the time this report was written. 12 The most common any-grade adverse event reported in the CDK4/6i arm of MONALEESA-2 was neutropenia (74%), while the most common in MONARCH 3 was diarrhea (81%).1,7 Understanding the impact of CDK4/6i-related adverse events on QoL is important for treatment decision-making. It is highly relevant to view these results in the context of findings from a recent survey that highlighted specific CDK4/6i-related adverse events impacting patient QoL. 16 In that multi-country survey, patients treated with CDK4/6is reported that diarrhea, fatigue, and appetite loss had a moderate/severe impact on their QoL. The side effect reported by patients treated with a CDK4/6i as having the greatest impact on QoL was diarrhea, which was reported as having a moderate to severe impact on QoL by 75% of patients. Furthermore, several published patient preference surveys, which utilized discrete choice experiments, reported that risk of diarrhea was one of the most important attributes to both patients and physicians when making treatment decisions for ABC and early breast cancer, including whether to use a CDK4/6i.26–28
Analyses like this and the prior MAIC of PALOMA-3 and MONARCH-2 allow for greater understanding of the impact of CDK4/6i-related adverse events and support consideration of QoL, in addition to efficacy and safety, when making treatment decisions. 25 The ESMO Magnitude of Clinical Benefit Scale was created to provide a tool to guide clinical decision-making and considers efficacy, safety, and QoL to assign ratings to cancer therapies. 29 Scores of 4 and 5 indicate substantial clinical benefit. 30 Based on these parameters, ribociclib combined with ET received the highest score (5/5) of the CDK4/6i for the first-line treatment of premenopausal women as per MONALEESA-7 data and the highest score of the CDK4/6is (4/5) for the first-line treatment of postmenopausal women in combination with AI (MONALEESA-2 data), while first-line abemaciclib in combination with AI received a score of 3/5 and is pending the MONARCH 3 OS readout.29,30
MAIC is a well-established and accepted methodology that utilizes individual patient data from one trial and summary data from another. In doing so, this method statistically controls for cross-trial differences in patient populations and provides clinically important comparative results in the absence of head-to-head studies. However, a few limitations should be noted. While MAICs balance treatment-effect-modifying patient characteristics measured in the trials, there may be unmeasured differences between trials that could not be matched. Although the majority of key baseline patient and disease characteristics were matched, the results may be confounded by any unreported factors because only published characteristics for MONARCH 3 were controlled for in this analysis. Interpretation of these results is limited to the subset of patients in MONALEESA-2 who were matched with patients in MONARCH 3. Additionally, the extreme weights required for some patients during matching adjustment may have led to low statistical power for detecting differences between treatments.
In view of the growing role of CDK4/6is in treatment of early breast cancer, it is of increasing importance to give more consideration to QoL in addition to other treatment outcomes. The results from this MAIC indicate that ribociclib + AI was associated with better symptom-related QoL compared with abemaciclib + AI in the first-line treatment of postmenopausal women with HR+/ HER2− ABC. These findings support the overall clinical benefit of ribociclib treatment and the value of understanding that the CDK4/6is are different with respect to all the outcomes, including efficacy, safety, and QoL. It is important to consider these results in light of the most common adverse events identified by patients to have a large impact on day-to-day QoL during treatment with CDK4/6i, including diarrhea, fatigue, and appetite loss. 16 Patients treated with abemaciclib experience QoL that is more heavily impacted by these important adverse events compared with those treated with ribociclib.
Footnotes
Acknowledgements
We thank the patients who participated in this trial, their families, and their caregivers; members of the data monitoring committee; members of the study steering committee; staff members who helped with the trial at each site; and Daniele Cary, PhD, of MediTech Media for medical editorial assistance with this manuscript. Ribociclib was discovered by Novartis Institutes for BioMedical Research in collaboration with Astex Pharmaceuticals.