
Abstract
Introduction:
The MONALEESA-7 trial compared ribociclib plus endocrine therapy (ET) with placebo as first-line treatment of advanced luminal/HER2-negative breast cancer (ABC) in premenopausal and perimenopausal women (age <50 years) and showed significant benefits to progression-free survival and overall survival. This study aimed to compare the cost-effectiveness of ribociclib + ET versus ET alone in patients with ABC from the perspective of the Brazilian public national health system.
Methods:
We calculated the incremental cost-effectiveness ratio (ICER) using a Markov model with progression-free survival, post-progression survival, and death states. We expressed ICER as incremental costs per progression-free life-year (PFLY) and quality-adjusted life-year (QALY) gained in a 10-year time horizon. We used parametric survival distributions fit to MONALEESA-7 data to generate survival distributions for progression-free and post-progression survival. The largest British preference study in breast cancer served as the basis to estimate health-state utilities. We estimated direct costs (ABC treatment, follow-up, monitoring, and adverse events) using Brazilian-specific values from public sources. An expert consensus panel determined the resource patterns required. We applied annual discounts of 5% to costs and QALYs.
Results:
Ribociclib + ET resulted in an incremental gain of 1.03 PFLYs and 0.80 QALYs at a cost of $37,319.31. The ICER of ribociclib + ET versus ET was $36,379.41 per PFLY gained and $46,590.79 per QALY gained. In deterministic sensitivity analysis, results were primarily affected by the annual discount rate, followed by the cost of ribociclib. In probabilistic sensitivity analysis, simulations agreed with the base-case.
Conclusion:
Ribociclib increased PFLYs and QALYs in patients with HR+/HER2− ABC when added to ET. Because Brazil does not have a formally defined cost-effectiveness threshold, other domains need to be considered for incorporation decisions, such as disease burden and humanistic impact on this young, economically active population. These findings may be useful in discussions for incorporation of ribociclib into the Brazilian public health system.
Introduction
Breast cancer (BC) is the world’s most commonly diagnosed cancer. 1 In Brazil, 66,280 new cases are estimated to have occurred in 2020, a rate of 43.74 cases per 100,000 women. 2 Approximately 70% of BCs are positive for hormone receptor (HR) and negative for human epidermal growth factor receptor 2 (HER2), which are referred to as luminal BC. 3
In Brazil, it is estimated that 44,642 women lived with advanced BC (ABC) in 2018, with 58% of cases being luminal ABC, 4 for which endocrine therapy (ET) is the current recommended treatment. 5 The combination of ET with a CDK4/6 inhibitor represents the new reference standard for treatment of luminal ABC according to the main international guidelines. 6
Ribociclib, one of the representatives of the class of CDK4/6 inhibitors, has led to a significant improvement in progression-free survival (PFS) and overall survival (OS), while maintaining or improving patient quality of life, in a series of randomized, double-blinded, placebo-controlled phase III trials: MONALEESA-2,7 –9 MONALEESA-3,10,11 and MONALEESA-7.12,13 These trials investigated ribociclib in combination with aromatase inhibitors (letrozole or anastrozole)7,8,10 –12 or fulvestrant10,11 in premenopausal,12,13 perimenopausal,12,13 and postmenopausal women7,8,11 in first8 –13 and second lines of treatment.10,11 In all these patient profiles, ribociclib combined with ET demonstrated consistent gains in PFS (risk reduction for progression ranging from 41% to 45%) and OS (risk reduction for death of 24%, 28%, and 29%), while maintaining8,10 or improving quality of life. 14
Ribociclib has not yet been incorporated into the Brazilian public national health care system. In Brazil, the National Committee for Technology Incorporation (CONITEC, for the acronym in Portuguese) is responsible for recommending for or against the incorporation of health technologies into the public health care system. CONITEC is affiliated with the Brazilian Ministry of Health and bases its decisions on health technology assessment (HTA). Although there is no official cost-effectiveness threshold in Brazil to determine whether a technology is cost-effective or not, economic impacts are a crucial factor in CONITEC’s decision. Therefore, it is important to provide economic evidence to better inform health decision-making.
This study aimed to explore the cost-effectiveness of ribociclib as first-line therapy in premenopausal or perimenopausal women with HR+/HER2− ABC from the perspective of the Brazilian public national health care system, with effectiveness defined by progression-free life-years (PFLYs) gained as the primary outcome. We also presented the results as costs per quality-adjusted life-year (QALY) gained.
Methods
Population
We estimated the cost-effectiveness of ribociclib plus ET (letrozole or anastrozole) versus ET as monotherapy for first-line treatment in premenopausal or perimenopausal women with HR+/HER2− ABC, based on the MONALEESA-7 trial, using a Markov model.
Markov model
The modeling time horizon was 10 years, the length of cycle was 30 days, and we applied no half-cycle correction. We considered three mutually exclusive health states: PFS, post-progression survival (PPS), and death (Figure 1).
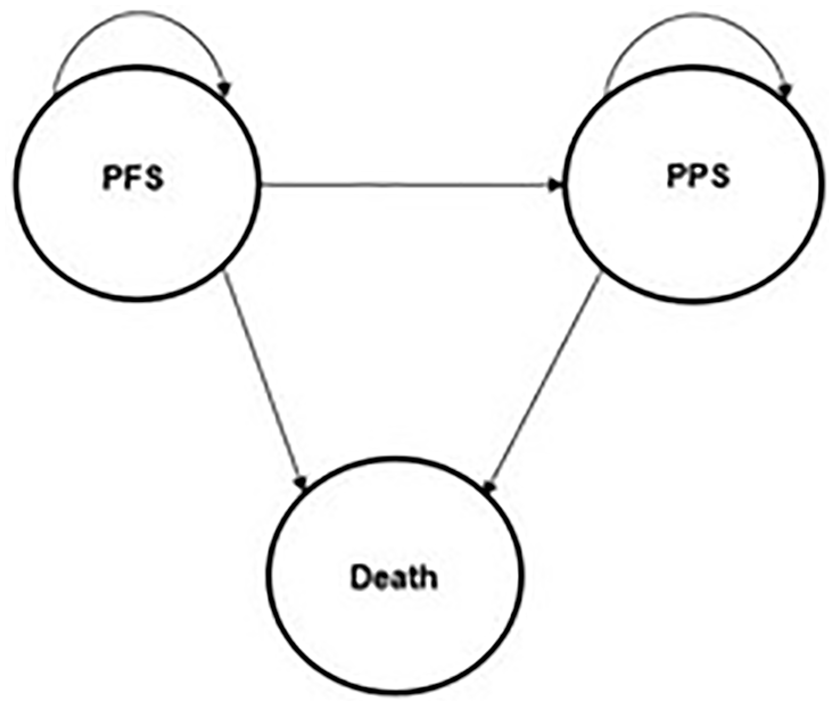
Markov cycle states.
In each strategy, we assumed that the cohort entered the model in the PFS state. At the end of each cycle, patients could remain in PFS, transit to PPS, or transit to death. In the PPS state, patients could remain in PPS or transit to death. Death is an absorptive state.
A third party performed the analysis from the perspective of the Brazilian public national health care system using Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA). The analysis included all direct medical costs: costs of drug acquisition and monitoring, health state-specific disease monitoring, subsequent therapy, and management of adverse events. Future costs and benefits were discounted at 5% annually, consistent with Brazilian guidelines for economic evaluations. 15
An independent researcher (C.A.d.S.M.) developed the model and performed the analyses. A panel consisting of 14 oncologists defined the patterns of health resources for patient monitoring and follow-up in each health state and management of adverse events, which is justified by the paucity of literature defining these parameters. The panel consisted of physicians from both public and private health care systems, thus offering perspectives representative of real-world clinical practice. The panel analyzed the health resources for each pattern through electronic forms in five rounds and defined them by a simple majority. The panel also validated all model assumptions.
Efficacy and transition probabilities
PFS events could be disease progression, resulting in patients transiting to the PPS state, or death. We estimated the proportion of PFS events that resulted in death by using original data from MONALEESA-7 trial extension 16 and assumed that it was dependent on the initial treatment received. We used the rate of PFS events that resulted in death to calculate the proportion of PFS events that were disease progression. Because the data did not differentiate the probability of death between health states, we assumed that both PFS and PPS had the same probability of death.
Because there were no data for the 10-year horizon, we considered several parametric distributions to extrapolate the data, including Gompertz, Weibull, log-logistic, exponential, and lognormal. We used the Akaike information criterion (AIC) and visual inspection to assess goodness of fit (Supplementary Figures 1–4).
Utility parameters
A British study considered the largest preference study in BC designed to survey a representative general public sample 17 provided the basis for the utilities and disutilities associated with the side effects of ribociclib. Based on the results of the MONALEESA-7 trial, 12 we considered the following monthly side effects in the ribociclib arm: 0.52% for febrile neutropenia, 0.99% for diarrhea/vomiting, 1.2% for fatigue, and 0.57% for stomatitis. In the ET arm, we considered the following side effects: 0.36% for stomatitis and 1.3% for asthenia. We estimated utilities in the PFS and PPS states, respectively, at 0.744/0.480 for ribociclib and 0.746/0.480 for ET.
Cost parameters
The present model assumed that, after transiting to PPS, new metastatic sites would occur, impacting costs and disutilities. We extracted the frequencies of site-specific metastasis from the claims database of the Brazilian public national health care system (DATASUS, for the acronym in Portuguese). Each metastatic site has a specific cost estimation and, after transiting to PPS, the subsequent treatment is chemotherapy.
We converted costs from Brazilian reais (R$) to United States dollars ($) based on the official exchange rate on 22 March 2021: $1 = R$5.53. We used the costs of tests and treatments as described on Brazilian government’s official open-access databases. 18 We grouped costs according to Markov states (PFS, PPS, and death) and treatment arms. In the PFS state for the ribociclib arm, we also considered the costs for adverse events, treatments, and specific monitoring tests (Table 1). We summarized all side-effect costs in Supplementary Tables 1–7.
Cost parameters in the progression-free survival state.

CT, computed tomography; NA, not applicable; PET, positron emission tomography.
In Brazil, cancer treatments are reimbursed according to a fixed amount per type of procedure (bundled payment model). The decision on the therapeutic approach is defined by the clinical guidelines established in each hospital. For BC, there are two authorized treatment options, namely ‘hormone therapy treatment’ and ‘chemotherapy treatment’. Each procedure costs $54.52 and $430.2, respectively, and these amounts also include the treatment with luteinizing hormone-releasing hormone (LHRH) agonists necessary to induce menopause in perimenopausal and premenopausal women. Because ribociclib is not yet incorporated into the Brazilian public health system, the cost of the procedure for ribociclib treatment is not defined. Thus, the maximum price that ribociclib can be sold to the Brazilian government (government’s price ceiling, 18%) served as the basis for the calculation of the monthly cost of ribociclib ($2050.76), which is based on an open list according to Brazilian laws.
We considered both ribociclib dose reduction and clinical trial dropout rate when estimating average monthly drug costs. Pooled data from the MONALEESA-2, MONALEESA-3, and MONALEESA-7 trials provided the basis for ribociclib dose reductions, where 45.8% of patients had at least one dose reduction (from 600 to 400 mg); of these, 31.5% had two dose reductions (from 600 to 200 mg). We estimated a continuous average monthly dropout rate of approximately 1.2% by combining data from MONALEESA-7 trial and MONALEESA-7 trial extension. 19 Conservatively, we considered only the cost impact of dose reduction. We did not consider the impact of the utilities associated with ribociclib discontinuation, thus avoiding side effects, as this could overestimate cost impact in the incremental cost-effectiveness ratio (ICER) results.
We estimated PFS and PPS state costs based on the following health resources: blood counts, imaging tests, biopsy, metastasis, and subsequent chemotherapy (Table 2). We calculated death costs ($212.91) based on the Brazilian government’s official open-access cost database for long-term treatment of patients with oncological diseases. 18
Cost parameters in the post-progression survival state.

CT, computed tomography; PET, positron emission tomography.
Outcome measures
We expressed ICER in terms of incremental costs per PFLY gained. We also presented ICER considering QALY gains.
Sensitivity analysis
We performed one-way deterministic sensitivity analyses by varying the value of one parameter at a time to analyze the effects on ICER. Supplementary Table 8 provides the range of each parameter and its reference. When reported data were not available, we defined variance as 20% of the base-case value. We presented the results of one-way sensitivity analyses in a tornado diagram. We conducted probabilistic sensitivity analyses using 1000 Monte Carlo simulations, with each simulation randomly sampling from the distributions of all parameters. We assigned gamma distribution to costs and beta distribution to clinical probabilities and utility scores. Because hazard ratios for transiting to PPS or death states varied according to their confidence interval in pivotal studies, we analyzed them with a lognormal distribution.
Results
The estimated total cost of ribociclib plus ET was $50,733.64, while the estimated total cost of ET alone was $13,414.33, representing an incremental cost of $37,319.31. Regarding effectiveness, ribociclib plus ET resulted in a gain of 2.79 PFLYs, compared with 1.76 PFLYs gained with ET alone, representing an incremental gain of 1.03 PFLYs. When we measured effectiveness by QALYs, we observed a gain of 2.78 QALYs with ribociclib plus ET and 1.98 QALYs with ET alone, representing an incremental gain of 0.80 QALYs. The estimated ICER of ribociclib plus ET was $36,379.41 per PFLY gained and $46,590.79 per QALY gained (Table 3).
Results of ribociclib versus endocrine therapy alone for advanced luminal breast cancer in the Brazilian public national health care system.

ICER, incremental cost-effectiveness ratio; PFLYs, progression-free life-years; QALYs, quality-adjusted life-years.
One-way sensitivity analysis showed that the parameter with the greatest impact on ICER per PFLY gained was discount rate, which was set at 5% annually as recommended by the Brazilian guidelines for economic evaluations and, in this model, ranged from 0% to 10% in the measurement of its impact on ICER results. The second most important parameter was ribociclib cost (Supplementary Figure 5).
Supplementary Figure 6 shows the results of probabilistic sensitivity analysis for PFLYs. The results of all simulations were in accordance with the base-case results, maintaining all simulations at the same upper right quadrant and showing that ribociclib enhanced both costs and benefits in all 1000 simulations.
Supplementary Figure 7 displays the cost-effectiveness acceptability curves for PFLYs gained. The probability of ribociclib being cost-effective per PFLY gained starts at a willingness to pay of $22,400.00.
Discussion
The cost-effectiveness findings suggest that ribociclib plus ET yield relevant effectiveness gains, with additional costs for the health care system. We based our economic model on the MONALEESA-7 trial, a unique high-quality randomized phase III trial evaluating ribociclib in combination with ET as first-line treatment of HR+/HER2− ABC in premenopausal and perimenopausal women with a median age of 50 years. This pivotal trial demonstrated significant OS and PFS gains with ribociclib, reducing the risk of death by 29% and reaching a median PFS of 27.5 months in combination with aromatase inhibitors (letrozole or anastrozole). In addition, in this population, ribociclib achieved a statistically significant improvement in quality of life, being the only indication and representative of CDK4/6 inhibitors achieving the maximum score of the magnitude of benefit of ESMO (European Society for Medical Oncology) clinical practice guidelines. More importantly, these benefits are sustained in the long term, reaching a median OS of 57.8 months as first-line treatment in this population 16 and 53.7 months when combined with fulvestrant. 20 The consistent magnitude of this benefit was recently confirmed by the publication of OS data from the MONALEESA-2 trial. In that study, the median OS achieved with ribociclib plus letrozole in the first-line treatment of postmenopausal women was 63.9 months, one of the highest medians ever achieved with a BC treatment. 7
Even if the ICERs are above the threshold adopted in a country (formally or not), HTA is a multicriteria process, that is, it will encompass criteria other than cost-effectiveness results. This includes a clear and transparent clinical condition prioritization agenda based on epidemiological importance and unmet clinical needs, magnitude of benefit of the health technology, patients’ preferences, equity, implementation, and logistic aspects, as well as budget impact estimations. Taken together, all these criteria are important in the decision-making process.
In Brazil, BC represents a high epidemiological, humanistic, and economic burden. 21 In the public national health care system, approximately 40% of all BC cases are ABC, of which 58% are HR+/HER2− in the metastatic stage. 4 Therapeutic options for ABC are considered palliative, aiming to prolong the patient’s life, maintain or improve quality of life, and postpone the need for chemotherapy. 22 For patients with HR+/HER2− ABC, the Brazilian Ministry of Health Clinical Guidelines recommend using all the therapeutic arsenal of ET, reserving fulvestrant for second-line treatment. However, these therapies fail to meet the goals of palliative treatment, with major limitations represented by primary and secondary resistance, where most patients will be unresponsive and treatment will fail. 23 On a more critical note, subsequent lines of ET provide little benefit, advancing the need for chemotherapy and failing to extend survival significantly. 24 There has been no therapeutic innovation for HR+/HER2− ABC for almost 20 years, with fulvestrant being the latest innovation introduced in 2002. Conversely, we do not see a lack of innovation for the type of BC that accounts for approximately 20% of cases, the HER2+ subtype. For this type of BC, trastuzumab and pertuzumab have changed the natural history of the disease by promoting significant OS gains. The benefits are so significant that, in 2017, CONITEC recommended the incorporation of both molecules into the Brazilian public health care system.
Since 2016, a new class of drugs has emerged as a disruptive treatment for the most common subtype of BC (HR+/HER2−), represented by CDK4/6 inhibitors, whose mechanism of action is able to reverse resistance to ET.25,26 They are currently recommended as the gold standard by the main national guideline27,28 and by international guidelines. 6
Discussing HTA incorporation of these innovations into the Brazilian public national health care system is a necessary step. It is important to highlight that all CDK4/6 inhibitors have been available to patients in the private health care system since April 2021, having their clinical relevance recognized in this perspective. In this setting, the Brazilian National Supplementary Health Agency (ANS, for the acronym in Portuguese) serves as the decision-maker for approximately 47 million people. ANS also uses HTA for incorporation decisions, and cost-effectiveness studies conducted from the perspective of the private health care system were an important criterion in that decision-making. 29 Providing access to these innovations only for patients in the private health care system will exacerbate the differences between both health care systems, thus increasing inequity in BC treatment. Lack of access to CDK4/6 inhibitors in the public setting represents an important gap to be filled, considering the recognized importance of benefits to patients with BC. In fact, reimbursement for these innovations is a major challenge, given the high prevalence and incidence of ABC and costs associated with treatment. However, there is a need for discussion among all stakeholders involved in the process to make this incorporation feasible and to provide alternatives, such as innovative access models, for the benefit of thousands of patients.
Although ribociclib has demonstrated significant and consistent gains in OS,5 –7 our primary effectiveness outcome was PFLYs, which is not a usual outcome in cost-effectiveness studies. The reason for our choice was to provide complementary cost-effectiveness evidence by exploring an outcome that is often considered underestimated from the clinical point of view. It is defined by some authors and decision-makers, including Brazilian guidelines, as a surrogate outcome and is usually not taken into account in health decision-making. 5
In this respect, disease progression is associated with anxiety and a need for more consultations, tests, and hospitalizations for disease-related and treatment-related complications, in addition to advancing the need for chemotherapy, which negatively impacts patients’ quality of life. 30 Ribociclib, which promotes long periods of PFS, has a clinically manageable adverse event profile with the potential to avoid hospitalizations for treatment-related complications.
Benefits are further enhanced when considering the profile of young women who can benefit from ribociclib, as presented in this study. In Brazil, it is estimated that 39% of all BC cases occur in premenopausal women.31,32 Clinical manifestations in this population differ from those in older women, with worse prognostic features and more aggressive tumors, suggesting that younger age is an independent predictor of adverse outcomes.33,34
Young premenopausal women also experience age-specific issues that significantly impair their quality of life. 35 Specific concerns include issues related to motherhood and future goals, as they are confronted with a life-threatening illness.36,37 They also express concerns about body image and sexuality.38,39 As young women are in the workforce, a medical condition or treatment can interrupt their careers and have a negative impact on household income. These factors suggest that illness may place a greater humanistic burden on younger women than in older women with BC.
The economic burden of BC is also significantly greater in younger women than in older women, 40 with greater productivity loss for the former. In Brazil, ribociclib has had a positive impact on productivity loss. Using the Work Productivity and Activity Impairment: General Health (WPAI:GH) questionnaire, data from 672 patients in the MONALEESA-7 trial were analyzed. For an estimated number of 4294 new cases of premenopausal HR+/HER2− ABC per year, the analyses indicated that women treated with ribociclib plus ET would potentially yield $12.95 million in productivity and activity compared with women treated with ET alone. 41
This study has strengths and limitations. A third party developed the model and performed the analyses, with no interference from the sponsor. Because clinical trials reporting PFS and OS are scarce and often have limited follow-up, we had to extrapolate the data, which always increases uncertainty about the results. We used a systematic method based on predetermined selection criteria (AIC) to provide a transparent approach for data extrapolation and to reduce the risk of bias. Furthermore, despite extracting the utility values from the largest preference study in BC, we did not validate their generalization to the Brazilian patient population. To define the patterns of monitoring and follow-up of the health states of the model and also for the management of adverse events of treatments, we used an expert consensus panel mainly because the literature defining such parameters is scarce and clinical practice may differ between countries. As the panel consisted of clinical oncologists who work from both the public and private health care system perspectives, the standard and frequency of consultations or examinations may have been overestimated from the public system perspective. Even so, considering the low amounts reimbursed by the public system, such amounts are not expected to change the magnitude of the results, which are, in most cases, driven by treatment costs.
Conclusion
Given the clinical, humanistic, and economic burden imposed by BC in Brazil, new treatment options that significantly improve patient outcomes are needed for patients in both public and private health care systems. The substantial PFS and OS benefits gained with ribociclib warrant further discussions and negotiations, as ribociclib should become an economically viable option for patients in the Brazilian public national health care system.
Supplemental Material
sj-docx-1-tam-10.1177_17588359221100865 – Supplemental material for Cost-effectiveness of ribociclib for premenopausal or perimenopausal women with HR+/HER2− advanced breast cancer: a Brazilian public health care system perspective
Supplemental material, sj-docx-1-tam-10.1177_17588359221100865 for Cost-effectiveness of ribociclib for premenopausal or perimenopausal women with HR+/HER2− advanced breast cancer: a Brazilian public health care system perspective by Daniela Dornelles Rosa, Carlos Alberto da Silva Magliano, Sergio D. Simon, Gilberto Amorim, Tomás Reinert, Luciana Landeiro, Débora de Melo Gagliato, Pedro Exman, Daniel Argolo, Gisah Guilgen, Max Mano, Laura Testa, Pedro Liedke, Romualdo Barroso, Mariana Sasse and Anna Maria Buehler in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
not applicable
Statement of ethics
Considering the nature of the study, which did not include patients’ data and used only secondary data, the study was exempt from ethics committee approval and waiver of informed consent was applied.
Consent for publication
not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Novartis Brasil sponsored this research.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.M.B. and M.S. are employers of Novartis Biociências S.A. The other authors received fees for the composite of the consensus panel.
Supplemental material
Supplemental material for this article is available online.
Availability of data and materials
All data generated or analyzed during this study are included in this article and its supplementary materials files. Further enquiries can be directed to the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.