
Abstract
Background:
Although immune checkpoint inhibitors (ICIs) and targeted therapies have been widely used as adjuvant treatment for resected melanoma, the optimal therapy remains controversial. Therefore, we conducted this updated network meta-analysis (NMA) to assess the efficacy and tolerability of adjuvant therapies for cutaneous melanoma.
Methods:
PubMed, Embase, Cochrane library, and Web of Science were systematically searched for relevant literatures published in the last 30 years. Disease-free survival (DFS), overall survival (OS), and serious adverse events were considered as the efficacy and tolerability outcomes.
Results:
In all, 27 randomized controlled trials (RCTs) including 16,709 stage III–IV melanoma patients were enrolled in this NMA. For BRAF wild-type melanoma, our analysis showed that both nivolumab and pembrolizumab demonstrated significantly better DFS and tolerability than ipilimumab (10 mg/kg). Nivolumab, pembrolizumab, ipilimumab (3 mg/kg), and ipilimumab (10 mg/kg) all appeared to be effective in prolonging OS, but no therapy demonstrated significantly better OS than ipilimumab (10 mg/kg). Nivolumab + ipilimumab showed the best DFS, but did not appear to be effective in improving OS and ranked only seventh in tolerability. Vaccines and granulocyte-macrophage colony-stimulating factor therapies were well tolerated, but all failed to improve the DFS or OS in stage III melanoma patients. In terms of BRAF mutation-positive melanoma, ICIs (nivolumab + ipilimumab, nivolumab, pembrolizumab, ipilimumab; 10 mg/kg) exhibited comparable efficacy to dabrafenib + trametinib, and all these therapies showed significantly better DFS than placebo.
Conclusion:
Considering efficacy and tolerability, nivolumab and pembrolizumab seem to be preferable adjuvant therapies for patients with stage III–IV melanoma. For BRAF mutation-positive patients, more RCTs are still required to determine which is better between ICIs and targeted therapy.
Introduction
Melanoma is a malignant skin tumor that originates from melanocytes. 1 The incidence of melanoma has been increasing over the past few decades. In 2020, 325,000 patients were diagnosed with melanoma and 57,000 patients died from melanoma. 2 About 90% of melanoma patients are diagnosed without distant metastases, but most stage III–IV patients may experience recurrence after curative surgery. 3 Therefore, it is of great significance to prevent postoperative recurrence of melanoma through adjuvant therapy.
The approval of immune checkpoint inhibitors (ICIs) and targeted therapies has revolutionized the situation in which no drugs are available for the adjuvant therapy of melanoma. 4 However, the optimal adjuvant treatment for melanoma remains controversial.5,6 Although several network meta-analyses (NMAs) have compared adjuvant therapies for melanoma, these NMAs merely included literatures published in 2019 or earlier. Recently, a few randomized controlled trials (RCTs) have reported their results and provided new references for adjuvant treatment of melanoma.4,7,8 The IMMUNED trial (which included stage IV patients) and the Checkmate 915 trial (which mainly included stage III patients) compared the efficacy and safety of nivolumab + ipilimumab and nivolumab as postoperative adjuvant therapy, respectively.9,10 The S1404 trial compared the efficacy and tolerability of pembrolizumab versus ipilimumab (10 mg/kg) or high-dose interferon (HDI) as adjuvant therapy for stage III–IV resected melanoma. 11 In addition, during 2020–2021, multiple trials (E1609, COMBI-AD, EORTC-1325-MG, Checkmate 238, EORTC 18071) have published their long-term follow-up results for disease-free survival (DFS)of patients with stage III–IV resected melanoma receiving ipilimumab, HDI, dabrafenib + trametinib, pembrolizumab, or nivolumab as adjuvant therapy.5,6,12,13 These new results will provide further references for the selection of optimal adjuvant treatment for melanoma.
Several studies have shown that in BRAF mutation-positive melanoma, ICIs as adjuvant therapy may achieve comparable efficacy to targeted therapy; however, relevant head-to-head comparisons are still lacking.5,6,9 In addition to systemic therapy, vaccine is another attractive adjuvant treatment option for melanoma, as they can prevent postoperative recurrence by inducing an durable antitumor immune response with minimal toxic effects. 14 With the development of bioinformation technology and next-generation sequencing (NGS) technology, several new vaccines have been developed. In the past 2 years, three double-blinded RCTs have evaluated the efficacy and tolerability of dendritic cell-based vaccine (DCV), 15 seviprotimut-L vaccine (POL-103A), 16 and tumor lysate, particle-loaded, dendritic cell vaccine (TLPLDCV)17,18 in preventing the postoperative recurrence of resected stage III melanoma.
Therefore, we conducted this more comprehensive updated Bayesian NMA and systematic review to assess the optimal adjuvant therapy for stage III-IV melanoma according to DFS, OS (overall survival) and serious adverse effects (SAEs). We also exploratively evaluated the efficacy of ICI and targeted therapy as adjuvant treatment for patients with BRAF mutation-positive melanoma.
Methods
Protocol
This NMA was conducted under the guidance of the Preferred Reporting Items for Systemic Reviews and Meta-analysis, and has been registered in PROSPERO with the registration code of CRD42021275512.
Search strategy
Before searching the literature, two investigators searched the PROSPERO and INPLASY databases to avoid duplicate topic selections. Then, two investigators independently searched Medline (PubMed), Embase, Cochrane Library, Web of Science, and Clinicaltrials.gov for eligible RCTs published in English within the last 30 years (from 1991.01–2021.11). The main search terms were as follows: (melan* OR skin) AND (pembrolizumab OR nivolumab OR ipilimumab OR immun* OR vaccin* OR dabrafenib OR trametinib OR interferon OR IFN OR vemurafenib OR bevacizumab OR dacarbazine OR chemotherapy) AND (‘Randomized Controlled Trial’ OR ‘Random Allocation’ OR ‘Controlled Clinical Trial’ OR placebo) AND (‘phase II’ OR ‘phase III’ OR ‘phase IV’). The detailed search strategies are provided in Supplemental Appendix 1.
Eligibility criteria
RCTs meet the following criteria were included:
(1) Participants: patients with resected, locally advanced or metastatic melanoma.
(2) Intervention and control: patients were treated with ICIs, targeted therapy, vaccines, interferon (IFN), cytokine therapy, or chemotherapy as adjuvant therapy.
(3) Outcomes: the number of patients underwent grade 3–5 adverse events or the hazard ratios (HRs) and 95% confidence interval (95% CI) for DFS were reported or could be calculated according to the data or Kaplan–Meier curve provided.
(4) Study design: phase II/III RCTs with no fewer than 20 patients in each experimental arm.
For duplicated publications, the one with the longest follow-up and most comprehensive results was included. Studies that reported the mixed outcomes of stage III/IV and stage I/II were also excluded.
Data extraction
The following information was extracted from enrolled studies by two investigators separately: trial name, trial ID, first author name, year of publication, therapy regimens of each arm, number of patients enrolled, HRs and 95% CI for DFS, median follow-up, mutation status and BRAF mutation rate in each arm, number of patients underwent serious adverse events (SAEs), clinical stage and histological type of melanoma, proportion of males and median age of patients, phase and design of studies.
Our primary outcomes were DFS (time from randomization to first disease progression or death due to any causes) and OS (time from randomization until death from any cause). Secondary outcome was tolerability (the proportion of patients who had SAEs). For studies that provided Kaplan–Meier curves only, GetData Graph Digitizer and R software (survival, MASS, and splines packages) were applied to calculate HR and 95% CI based on the methods described by Guyot P. et al. 19 Any discrepancies in data extraction were conferred and solved by consultation among all investigators.
Quality assessment
The methodological quality of the enrolled RCTs was independently evaluated by two investigators using Review Manager (RevMan) v5.3, referring to Cochrane Risk of Bias tool, from the following aspects: selection bias, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. 20 The results of evaluation were graded as high, low, or unclear risk of bias. Any divergences were resolved by consultation among all investigators.
Statistical analysis
We used NMA to estimate pooled HRs (95% CI) for DFS and OS and pooled odds ratios (95% CI) for risk of SAEs to assess the efficacy and tolerability of adjuvant therapies.
The NMA was performed in Bayesian framework by R software (GEMTC package); the Markov chain Monte Carlo simulations were applied to estimate posterior densities (four independent Markov chains for each outcome). After a burn-in phase of 20,000 iterations, 200,000 inference iterations are run for each chain with a thinning interval of 10 for each chain to estimate the posterior distribution of the parameters.21,22 The deviance information criteria (DIC) value was used to assess the fit of each model, and if the difference between the DIC values of two models exceeded five, then the model with the smaller DIC value is selected.
In addition, SUCRA curves were utilized to rank the efficacy and tolerability of different adjuvant regimens. The SUCRA values ranged from 0 to 1, and the greater the SUCRA value of a therapeutic regimen, the more effective/safe that regimen is considered to be.23,24
To assess publication bias, comparison-adjusted funnel plot was constructed and egger’s test was performed (p ⩽ 0.1 was considered to indicate significant publication bias in the studies). 25 The consistency between direct and indirect comparisons for closed loops was evaluated using node splitting assay. In addition, a network meta-regression was performed to assess whether the effect of adjuvant therapies on DFS or OS were affected by median follow-up of the experimental and control groups.
To further select the optimal adjuvant treatment option, a two-dimensional approach was applied to take both efficacy and tolerability into account, and the intervention located in the upper left corner was preferred over the other interventions. 26
Results
Study characteristics
In total, 25,232 literatures were identified after searching databases, and 193 possible eligible articles were retrieved in full text (Figure 1). After full-text screening, 27 phase II/III RCTs (including 16,709 stage III-IV melanoma patients) conducted between 1993 and 2021, comparing 15 adjuvant therapeutic regimens, were enrolled in this NMA. Of all trials, 22 are phase III trials and 12 are double-blinded trials (Table 1).

Flow chart of study searching and selection.
Characteristics of included studies.

Ctrl, control group; DCV, dendritic cell vaccine; DFS, disease-free survival; Exp, experimental group; GMCSF, granulocyte-macrophage colony-stimulating factor; IFN, interferon; ITT, intention-to-treat population; NR, not reported; OS, overall survival; SAEs, serious adverse events; TLPLDCV, tumor lysate, particle-loaded, dendritic cell vaccine; TCV, therapeutic cancer vaccine.
There were seven trials (10 arms, 7675 patients) used ICIs as experimental group;5,6,9-12,27–29 three trials (four arms, 2029 patients) used targeted therapy as experimental group13,30–32; 11 trials (17 arms, 5214 patients) used IFN and/or chemotherapy as experimental group;16,33-42 and six trials (10 arms, 1791 patients) applied vaccines or/and GMCSF as experimental group.16–18,43–45 All trials reported their DFS outcomes, 23 trials reported OS outcomes, and 17 trials evaluated the tolerability of therapeutic regimens. In all, 24 trials reported their median follow-up duration (ranged from 16 to 91.2 months); 10 trials reported the proportion of BRAF mutation-positive patients; five trials reported the proportion of PD-L1-positive patients. HRs and 95% CI of seven trials were calculated based on Kaplan–Meier curve.17,39–42,44,45
The networks of comparisons for efficacy and tolerability are presented in Figure 2. The detailed characteristics of enrolled RCTs are summarized in Supplemental Table S1.

Network diagrams of eligible comparisons for DFS (a), OS (b), and tolerability (c). The thickness of the lines in the network diagram is in proportion to the number of direct comparisons of trials; the node size depends on the total sample size of the treatment.
Assessment of methodological quality
We performed a critical assessment of the methodological quality of the enrolled RCTs according to the Cochrane Risk of Bias tool. 46 In terms of random sequence generation, a total of 15 RCTs (55.56%) were assessed as low risk for randomization due to the authors’ detailed description of the principles of randomization, while the remaining 12 trials were defined as unknown risk. In all, 25 trials (92.59%) offered information about allocation concealment; therefore, they were considered to be low risk. In terms of performance bias, 12 double-blind trials (44.44%) were considered as low risk, while the remaining 15 trials were considered as high risk. Among enrolled RCTs, only eight trials (29.63%) introduced proper procedures in the blinding of outcomes assessment and therefore, were deemed to be at low risk for detection bias. For attrition bias, 25 trials (92.59%) reported the detailed information about withdrawals, and were considered as low risk. In terms of selective reporting, no trial explicitly showed reporting bias. Other bias was not reported. Supplemental Figure S1 shows the summary of risk of bias for enrolled trials.
Efficacy of adjuvant therapies in BRAF wild-type patients
After assessing the fit of each model by DIC (Supplemental Table S2), we compared the improvement of DFS with different adjuvant therapies by NMA in a random-effects model. There were eight regimens showed significantly better DFS than placebo/observation (Figure 3(a), Table 2). We ranked these eight therapies based on SUCRA values as follows: nivolumab + ipilimumab (0.996) > nivolumab (0.907) > pembrolizumab (0.835) > ipilimumab (10 mg/kg) (0.616) > ipilimumab (3 mg/kg) (0.561) > IFN + chemotherapy (0.548) > bevacizumab (0.47) > IFN (0.276) (Supplemental Figure S2). Among these therapies, nivolumab + ipilimumab, nivolumab, and pembrolizumab showed significant superior efficacy to ipilimumab (10 mg/kg) (Table 2).
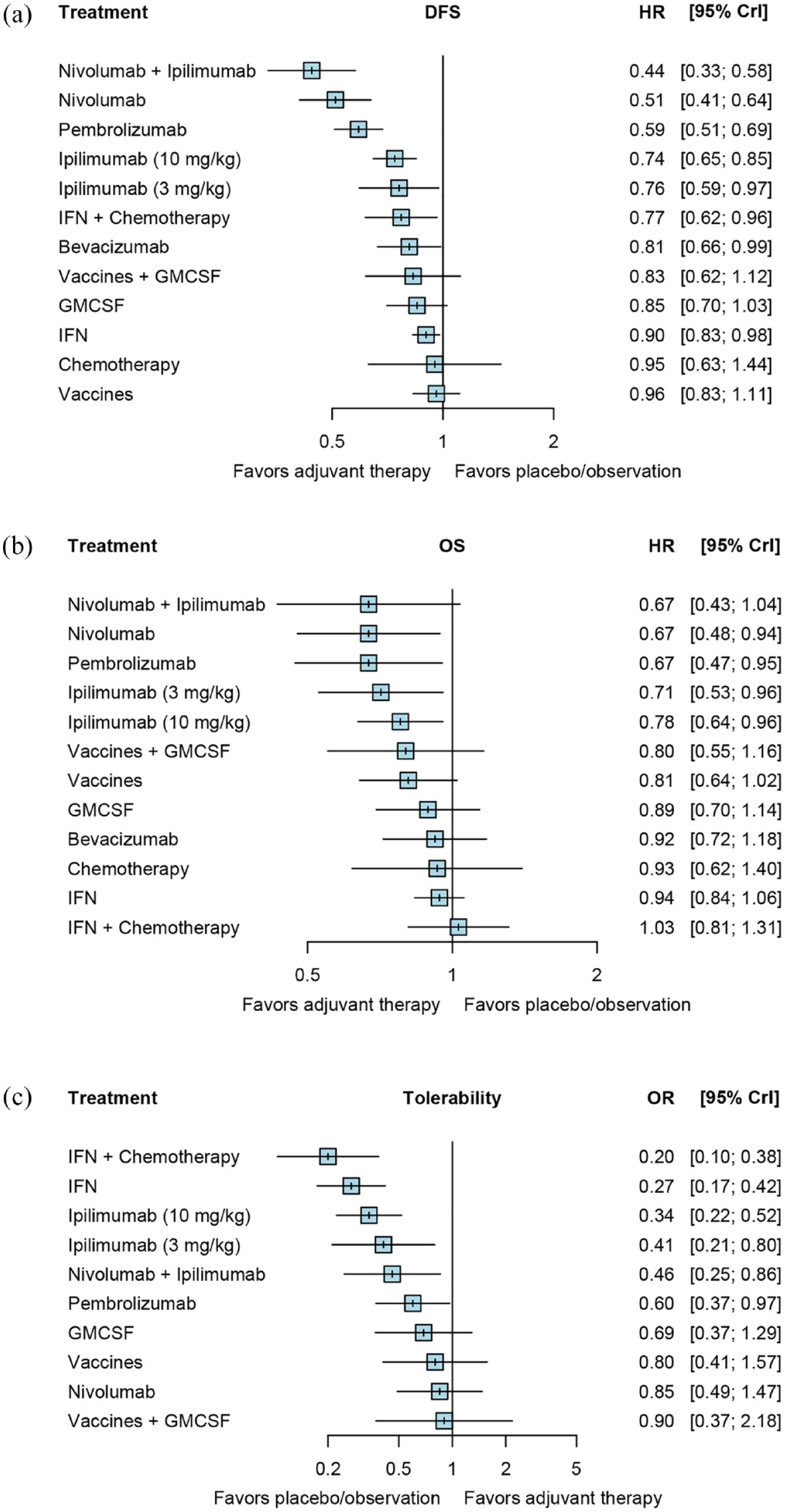
Forest plots of network comparisons of therapeutic regimens with placebo/observation for DFS (a), OS (b), and tolerability (c).
Network comparisons of the DFS improvement and tolerability of adjuvant therapies.

 Comparison.
Comparison.
 Efficacy (based on DFS).
Efficacy (based on DFS).
Tolerability (based on SAEs).
 Significantly better than ipilimumab (10 mg/kg).
Significantly better than ipilimumab (10 mg/kg).
Significant results are in bold. DFS, disease-free survival; GMCSF, granulocyte-macrophage colony-stimulating factor; IFN, interferon; SAEs, serious adverse events.
In addition, a network meta-regression based on median follow-up was performed to detect whether the DFS outcome was influenced by the length of follow-up. The results of meta-regression suggested no significant correlation between DFS and median follow-up (Supplemental Table S3). The comparison-adjusted funnel plot did not show significant publication bias (Supplemental Figure S3). The node-splitting analysis involved 13 loops and showed significant inconsistency in one loop (nivolumab + ipilimumab versus placebo/observation). (Supplemental Table S4).
According to DIC (Supplemental Table S5), we compared the improvement of OS with different adjuvant therapies by NMA in a random-effects model. There were four regimens showed significantly better OS than placebo/observation (Figure 3(b), Table 3). We ranked these therapies based on SUCRA values as follows: nivolumab (0.825) > pembrolizumab (0.797) > ipilimumab (3 mg/kg) (0.747) > ipilimumab (10 mg/kg) (0.610) (Supplemental Figure S4). No therapy showed significant better efficacy than ipilimumab (10 mg/kg) (Table 2).
Network comparisons of the OS improvement of adjuvant therapies.

 Comparison.
Comparison.
 Efficacy (based on OS).
Efficacy (based on OS).
Significant results are in bold. GMCSF, granulocyte-macrophage colony-stimulating factor; IFN, interferon; OS, overall survival; SAEs, serious adverse events.
Network meta-regression based on median follow-up suggested no significant correlation between OS and median follow-up (Supplemental Table S6). The comparison-adjusted funnel plot showed insignificant publication bias (Supplemental Figure S5). The node-splitting analysis involved 12 loops and showed significant inconsistency in one loop (vaccines versus GMCSF) (Supplemental Table S7).
Tolerability of adjuvant therapies in BRAF wild-type patients
After referring to DIC (Supplemental Table S9), we evaluated the tolerability of adjuvant therapies by NMA based on a random-effects model. There were four regimens showed significant better tolerability than ipilimumab (10 mg/kg) (Table 2). We ranked these regimens according to SUCRA as follows: vaccines + GMCSF (0.79) > nivolumab (0.776) > vaccines (0.733) > pembrolizumab (0.562) (Supplemental Figure S6). Among these therapies, nivolumab, GMCSF, vaccines, and vaccines + GMCSF showed comparable tolerability to placebo/observation (Figure 3(c), Table 2).
The consistency test for tolerability involved 10 loops and showed inconsistency in three loops [nivolumab versus ipilimumab (10 mg/kg), placebo/observation versus ipilimumab (10 mg/kg), and placebo/observation versus nivolumab + ipilimumab] (Supplemental Table S10). The comparison-adjusted funnel plot of the NMA for tolerability outcome did not show significant publication bias (Supplemental Figure S7).
Integrated analysis of efficacy and tolerability
Integrative analyses were performed in a two-dimensional manner to comprehensively assess the efficacy and tolerability of each treatment. As shown in Figure 4, nivolumab and pembrolizumab showed significant better DFS and tolerability compared with ipilimumab (10 mg/kg). Nivolumab + ipilimumab showed the best DFS, but only ranked seventh in tolerability among all regimens.

Two-dimensional ranking plot of DFS and OS (a), DFS and tolerability (b), OS and tolerability (c).
Efficacy of systemic therapies for BRAF-mutation positive patients
There were six studies (including 7 arms, 2517 patients) reported DFS outcomes, three studies reported OS outcomes, and two studies reported SAEs outcomes in BRAF mutation-positive patients receiving adjuvant therapy (Figure 5(a)). Among them, four trials used ICIs as experimental group, two trials used targeted therapy as experimental group. Placebo was used as control for all trials except for CheckMate 238 and CheckMate 915, which used ipilimumab (10 mg/kg) and nivolumab as controls, respectively (Table 4).

Network diagrams of eligible comparisons for DFS (a), and forest plots of network comparisons for DFS (b) in BRAF mutation-positive patients. The thickness of the lines in the network diagram is in proportion to the number of direct comparisons of trials; the node size depends on the total sample size of the treatment.
Characteristics of studies that reported efficacy outcome of BRAF-mutation melanoma patients.

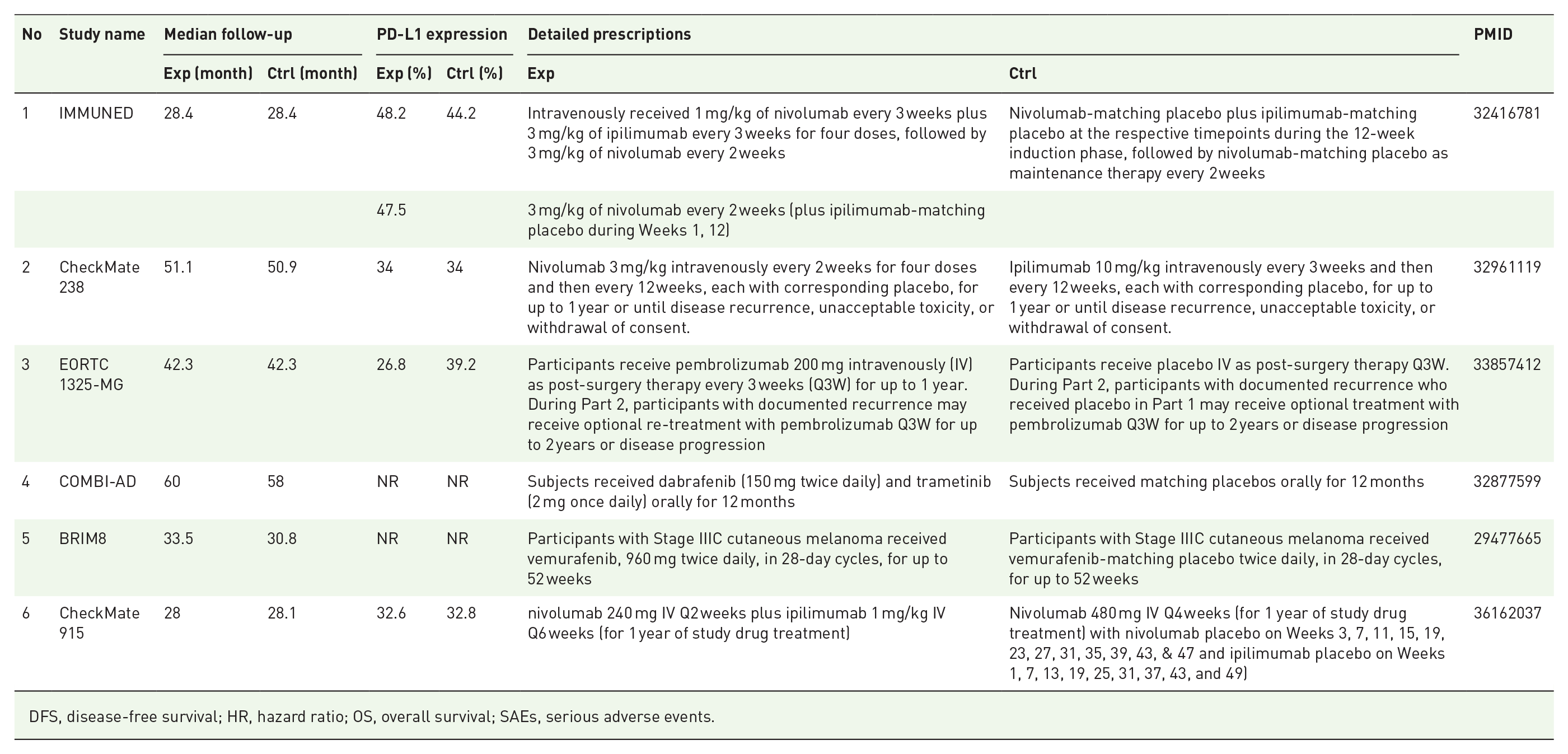
DFS, disease-free survival; HR, hazard ratio; OS, overall survival; SAEs, serious adverse events.
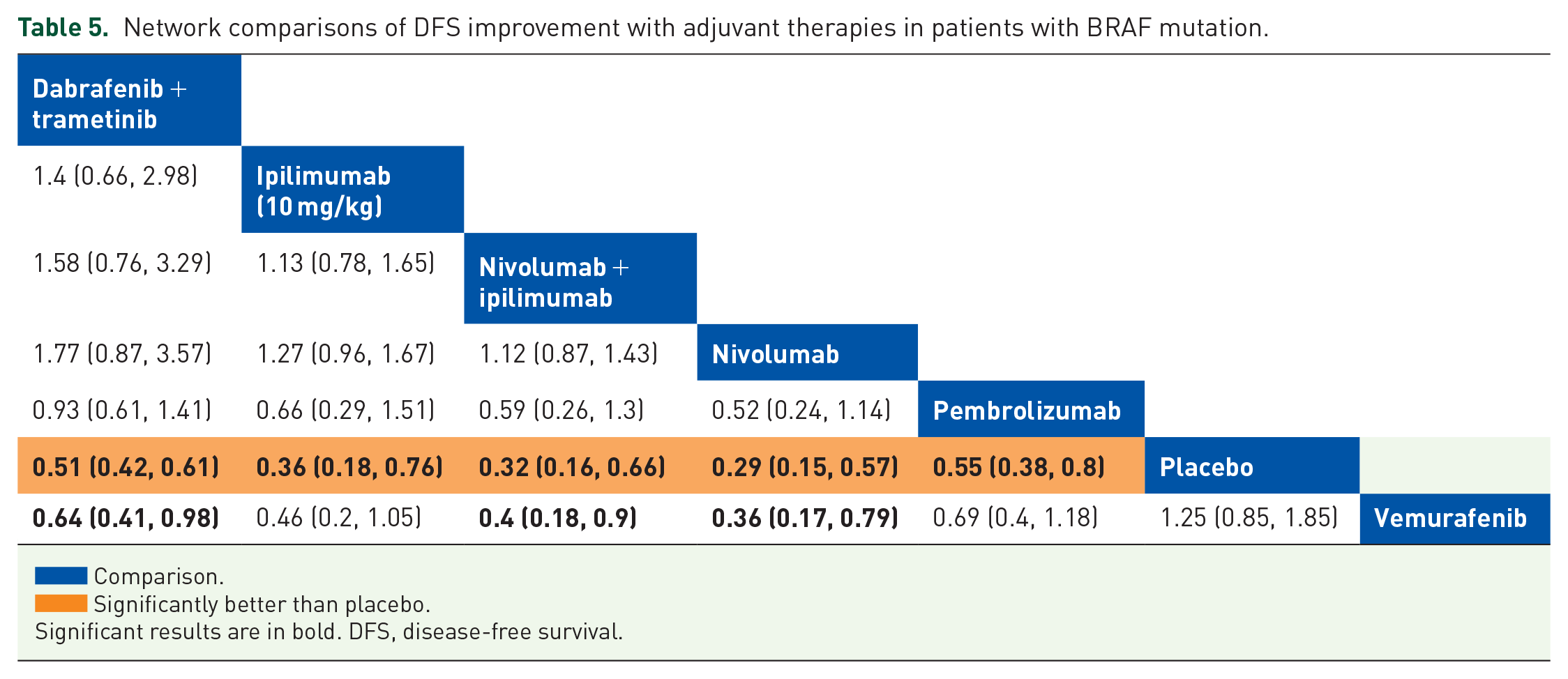
We assessed DFS improvement with different adjuvant therapies by NMA in a fixed-effects model. There were five regimens showed significantly better DFS than placebo (Figure 5(b), Table 5). We ranked these therapies based on SUCRA values as follows: nivolumab (0.941) > nivolumab + ipilimumab (0.785) > ipilimumab (10 mg/kg) (0.652) > dabrafenib + trametinib (0.497) > pembrolizumab (0.431) (Supplemental Figure S8). No therapy showed significant better efficacy than dabrafenib + trametinib (Table 5).
Network comparisons of DFS improvement with adjuvant therapies in patients with BRAF mutation.
 Comparison.
Comparison.
 Significantly better than placebo.
Significantly better than placebo.
Significant results are in bold. DFS, disease-free survival.
Discussion
Principal findings
The results of our NMA showed that compared with ipilimumab (10 mg/kg), both nivolumab and pembrolizumab demonstrated significantly better DFS and tolerability, but similar OS benefits. Although nivolumab + ipilimumab demonstrated the best DFS, but did not appear to be effective in improving OS and only ranked seventh in terms of tolerability. In terms of BRAF mutation-positive patients, both dabrafenib + trametinib and ICIs are effective in improving DFS, and they showed comparable efficacy.
Comparison with other studies
IFN
IFN is the first adjuvant therapy proven to be effective in reducing the risk of postoperative recurrence and improving the OS melanoma patients. 47 Despite numerous studies and meta-analyses have investigated the modes of IFN administration, the survival benefits that IFN can bring to patients is still very limited, besides the serious neutropenia, hepatotoxicity, and fatigue caused by IFN treatment cannot be ignored, either.36,48–52 The results of our NMA suggested that although IFN and IFN + chemotherapy showed significantly better efficacy than watchful waiting, they were inferior to ICIs both in terms of efficacy and tolerability.
ICIs
Ipilimumab is the first ICI authorized for adjuvant therapy of melanoma. EORTC 18071 trial demonstrated that ipilimumab (10 mg/kg) can effectively improve postoperative DFS in stage III melanoma compared with placebo. However, high-dose ipilimumab also caused serious toxic effects.28,29 In the subsequent E1609 trial, low-dose ipilimumab (3 mg/kg) showed better tolerability, but neither ipilimumab (3 mg/kg) nor ipilimumab (10 mg/kg) could bring patients better DFS than HDI. 12 The recently published 4-year follow-up results of Checkmate 238 trial demonstrated that compared with ipilimumab (10 mg/kg), nivolumab can provide patients a better DFS with fewer SAEs. 5 In S1404 trial, pembrolizumab group showed significantly better DFS and tolerability than ipilimumab (10 mg/kg) group. 11 Unlike previous trials that mainly recruited patients with resected stage III melanoma, the IMMUNED trial showed that nivolumab was effective in improving DFS in patients with stage IV resected melanoma. 9 The results of our NMA were basically consistent with the original trials, except that ipilimumab (10 mg/kg) was speculated to have significantly better DFS than IFN, but this may be because many of the trials using IFN were conducted many years ago, when the treatments were very different than they are today. The same conclusions were also reached in two previous NMAs based on stage II–IV melanoma patients.4,7 In addition, although our results showed that tolerability of nivolumab is as good as placebo, there is currently no clear scientific basis. This may be because most patients treated with nivolumab in this NMA were in stage III and tend to have better general condition.5,53
In terms of long-term survival benefit, neither nivolumab nor pembrolizumab demonstrated better OS than ipilimumab (10 mg/kg) in the trials.5,12 However, imbalanced post-relapse treatment situation between groups may have contributed to this result, and fewer OS events occurred than anticipated for the time-based prespecified statistical analysis, which may reduce the ability to detect true differences between groups. Furthermore, the clinical effects of ipilimumab (3 mg/kg) seemed to be more durable than ipilimumab (10 mg/kg) and may translate into greater OS benefits, which raised the question of whether increased toxicity of ipilimumab (10 mg/kg) affected the efficacy. In addition, in IMMUNED trial, the DFS benefit achieved with nivolumab versus placebo did not translate into the OS benefit. The rapid use of systemic therapy at first progression in the placebo group may partly explain this result, and the limited sample size of IMMUNED trial may also be considered as a limitation. Therefore, whether nivolumab monotherapy could significantly improve survival outcomes in patients who have reached the unresectable stage remains unanswered. Our NMA also attempted to analyze the OS outcomes of adjuvant therapies and reached conclusions consistent with the original studies, but the results are only exploratory and need to be to be interpreted with caution.
Nivolumab + ipilimumab combination therapy had drawn wide attention in the treatment of multiple tumors. In IMMUNED trial, nivolumab (1 mg/kg) + ipilimumab (3 mg/kg) combination therapy demonstrated significant better DFS than nivolumab monotherapy in stage IV melanoma patients. However, combination treatment also correlated with a significantly increased incidence of SAEs, with more than 70% patients in the combination therapy group experienced SAEs, while only 20% patients in the nivolumab monotherapy group. 9 The Checkmate 915 trial investigated the efficacy and tolerability of nivolumab (240 mg) + ipilimumab (1 mg/kg) as adjuvant therapy predominantly in patients with resected stage III melanoma, but ended in failure. 10 In Checkmate 915 trial, the dose and frequency of ipilimumab in combination group were significantly reduced compared with commonly used clinical dose (1 mg/kg Q6W versus 3 mg/kg Q3w), and the median duration of therapy and cumulative dose of nivolumab in combination group were lower than nivolumab monotherapy group (7.6 months/3840 mg versus 11.1 months/6240 mg). These might be related to the high discontinuation rate in combination group due to adverse events (32% versus 10%). However, in the nivolumab + ipilimumab group, the 6-month landmark DFS rates were similar between patients who did/did not discontinue treatment due to adverse events. Therefore, early discontinuation due to adverse effects was not sufficient to explain the lack of DFS benefit.
Although the difference in OS reached statistical significance for nivolumab + ipilimumab versus placebo in IMMUNED trial, there was a lack of OS benefit in recent trials including Checkmate 915, CheckMate 238, S1404 and nivolumab monotherapy arm in IMMUNED. Therefore, a question of whether waiting for recurrence and receiving treatment for metastatic disease might be acceptable to patients was raised, and this may help avoid the risk of potentially irreversible immune-related adverse events in patients whose disease can be cured with surgery alone.53,54 The oncologists need to discuss the known DFS benefits and the lack of OS benefit and side effects in the relatively short follow-up to date with the patient before making an adjuvant therapy decision. And assays like circulating tumor DNA (ctDNA), circulating tumor cells, tumor mutation burden (TMB), or exosome vesicles might be helpful in determining which patients are at a higher risk of disease recurrence after surgery. 55
Targeted therapy
In prior to BRAF/MEK inhibitors, AVAST-M trial investigated the efficacy of bevacizumab as an adjuvant therapy for stage II–III resected melanoma; however, the median disease-free interval was not reached. 30 Then, the COMBI-AD trial proved a durable long-term survival benefit of dabrafenib + trametinib combination therapy for stage IIIA-C resected melanoma with BRAF mutations. 13 In addition, the BRIM8 trial assessed the efficacy of vemurafenib as adjuvant therapy in patients with resected BRAF mutation-positive melanoma. In stage IIIC patients, the BRIM8 study did not meet its primary DFS endpoint. However, in patients with resected stage IIC-IIIB BRAF mutation-positive melanoma, vemurafenib adjuvant therapy reduced the risk of DFS events compared with placebo (HR: 0.54, 95% CI: 0.37–0.78). 32 On the basis of these results, it seems that the combination of dabrafenib + trametinib adjuvant therapy could provide a favorable DFS for melanoma patients with a high risk of recurrence. However, we cannot exclude a role for vemurafenib monotherapy in patients in certain disease sub-stages (IIC-IIIB), either.
Notably, among patients with BRAF mutations, the efficacy of pembrolizumab or nivolumab is consistent with the improvement reported in the COMBI-AD trial.5,6,13 Trials also found that patients with BRAF mutations especially seemed to benefit from nivolumab + ipilimumab combination therapy and this phenomenon was speculated to be associated with the use of Ipilimumab.5,9,56
Vaccines
Researchers have been trying to apply tumor vaccines to the adjuvant therapy of melanoma, and several phase II/III RCTs have evaluated the efficacy of vaccines, but all have failed. These vaccines include peptide vaccine (PV), 43 GMK vaccine (GMKV), 40 DCV, 17 and allogeneic TCV. 45
GMCSF is a well-tolerated cytokine whose activity suggests a possible role in cancer immunotherapy. 57 GMCSF can increase the number of monocytes/macrophages in cancer patients and enhance their ability to lyse tumor cells.58,59 GMCSF is also a major mediator of the maturation, proliferation and migration of dendritic cells.60,61 Some trials suggest that the application of GMCSF with melanoma vaccines may enhance the anti-tumor responses.62,63 In a phase II trial, Spitler et al. 44 demonstrated that GMCSF can improve postoperative DFS with a favorable tolerability for melanoma patients. However, in the subsequent E4697 trial, neither GMCSF nor GMCSF + PV combination therapy improved DFS in patients with resected stage III-IV melanoma, which did not support the assumption that systemic administration of GMCSF could enhance efficacy of PV. 43 Our analysis also came to the same conclusion as previous trials, that although the vaccines and GMCSF therapies were tolerated well, they both failed to improve DFS of stage III–IV melanoma.
Strengths and limitations
Here, we conducted an updated NMA, based on 27 phase II/III RCTs including 16,709 patients to evaluate the optimal adjuvant therapy for stage III-IV resected melanoma based on efficacy (DFS) and tolerability (SAEs). This NMA has several strengths from the following aspects. First, we included the results of multiple newly published studies and long-term follow-up outcomes and, for the first time, evaluated the efficacy and tolerability of nivolumab + ipilimumab combination therapy, which provided an updated reference for the selection of adjuvant treatment options for stage III-IV melanoma. Second, almost all included studies were multicenter RCTs, which minimized the potential selection bias originating from the study design. Third, we preliminary evaluated the efficacy and tolerability of vaccines as adjuvant treatment for melanoma, and discussed the relevant research advances.
However, this NMA is also restricted by many limitations. First, the number of enrolled studies is insufficient and many enrolled trails were conducted in the early days when surgical techniques and systemic treatments at that time are much different from what they are today. Therefore, more high-quality studies on novel therapies are required to draw more convincing conclusions. Second, there are some inconsistencies in this study which may be due to the differences in design or basic information across studies. Third, the follow-up between studies is different; therefore, we conducted a network meta-regression analysis and demonstrated that the length of median follow-up did not have statistically significant correlation with DFS or OS outcomes. Fourth, multiple studies on ICI were included in this NMA, but only few studies reported information on proportion of patients with BRAF mutations or PD-L1 positivity. In addition, HR and 95% CI of several studies were calculated based on Kaplan–Meier curves, which may be subject to large errors. In summary, the results of this study are only exploratory and should be interpreted with caution
Implications and future directions
IFN
Although the use of IFN in the treatment of melanoma has gradually declined, its contribution to the efficacy of ICI indicates that IFN may still have some clinical value. Recently, the Keynote-020 trial demonstrated that IFN could enhance the killing ability of cytotoxic T cells and stimulate immune cells, thereby promoting the efficacy of pembrolizumab in advanced melanoma. 64 This combination therapy was also well tolerated, but since Keynote-020 is a single-arm trial, these findings should be interpreted with caution. In addition, a retrospective analysis of Jia et al. 65 demonstrated that front-line therapy with IFN may enhance the efficacy of later-line adjuvant therapy with pembrolizumab, which offered the possibility of sequential treatment modalities of IFN and pembrolizumab in resected melanoma.
ICIs
At present, PD-1/PD-L1 inhibitors have become one of the most commonly used therapies in the clinical treatment of melanoma. However, PD-L1 expression was reported to be significantly attenuated in microscopic melanoma lesions <1 mm in diameter. 66 This suggests that additional biomarkers are required to help guide anti-PD-1/PD-L1 adjuvant therapy.
TMB is defined as the total number of somatic mutations per megabase and is considered as a biomarker that is independent of PD-L1. 67 To date, several trials and meta-analysis have confirmed the predictive effect of TMB on the efficacy of ICIs in the treatment of melanoma.68–71 In 2020, the FDA even approved anti-PD-1/PD-L1 therapy for patients with any type of solid tumor with TMB ⩾10 mut/Mb based on the results of the Keynote-158 trial. 72 However, the application of TMB in clinical practice still faces many problems. For example, some patients are not suitable for biopsy, and the invasive nature of biopsy makes it difficult to conduct real-time monitoring of tumor treatment by TMB, besides, the heterogeneity of the tumor itself may lead to large errors in TMB detection.73,74 As for detection methods, whole-exome sequencing requires a lot of time and cost, NGS technology still needs to be improved, and the cutoff value of TMB remains to be identified.75–77 Researchers have also tried to detect TMB levels using ctDNA in peripheral blood, so as to avoid the problems of tumor heterogeneity and biopsy invasiveness.78–80 However, it has been demonstrated that maximum somatic allele frequency of ctDNA and benign DNA mutations originating from blood cells are likely to cause severe interference in the detection of blood-based TMB.81–83 Therefore, the application of TMB in the screening of ICI treatment advantage population still needs to be further supplemented and improved by more prospective RCTs and meta-analyses.
On 18 March 2022, the FDA officially approved Opdualag, the ‘first-in-class’ lymphocyte-activation gene-3 (LAG-3) product, for the treatment of unresectable or metastatic melanoma. 84 Opdualag is a pre-mixed combination of nivolumab and relatlimab (anti-LAG-3), administered by intravenous injection. In the RELATIVITY-047 trial, the 12-month DFS rate for the relatlimab + nivolumab combination group was 47%, which was not significantly different from the 49% in the ipilimumab + nivolumab combination group in the CheckMate 067 trial. However, 59% of patients receiving ipilimumab + nivolumab experienced SAEs, while this value was only 19% in relatlimab + nivolumab combination group, suggesting a better tolerability of relatlimab + nivolumab. 85 As the fourth approved immune checkpoint, LAG-3 is a type I transmembrane protein with a similar structure to CD4. Accumulating evidence suggests that LAG-3 is an inhibitory coreceptor that plays a key role in autoimmunity, tumor immunity and anti-infection immunity. 86 Conventional view suggests that, similar to PD-1, blocking the interaction between LAG-3 and MHC II restores T-cell activity. 87 However, a recent study has shown that LAG-3 molecule can migrate to the immune synapse via the TCR-CD3 complex, and lower the pH of the immune synapse, causing dissociation of tyrosine kinase Lck from CD4 or CD8 co-receptors and blocking co-receptor-TCR signaling, thereby inhibiting T-cell activity. 88 These findings bring new opportunities and challenges for drug discovery around LAG-3.
Vaccines
One limitation of tumor vaccines is that the composition of tumor antigens is complex, limiting the recognition of therapeutically relevant immune response. 89 Slingluff et al. developed the Seviprotimut-L vaccine which contains a wide range of shared melanoma antigens and does not require patient selection based on expression of human leukocyte antigens.90,91 In the MAVIS trial, seviprotimut-L was shown to be well tolerated, but the improvement in DFS in patients with resected stage III melanoma did not meet expectations.15,92 However, in patients with stage II-IIIC disease who received seviprotimut-L therapy, there was a significantly improvement in DFS and OS. In fact, the FDA has approved Seviprotimut-L for the adjuvant therapy of patients with stage IIB/IIC melanoma in June 2020. 93
Another phase IIb RCT tested the efficacy of TLPLDCV as adjuvant therapy in patients with stage III/IV melanoma after surgery. TLPLDCV is an autologous dendritic cell vaccine that integrates all related antigens and neoantigens from the patients’ tumors into their individualized vaccines. 94 Although TLPLDCV was shown to be well tolerated in the trial, it failed to improve DFS but greatly prolonged OS in patients. 18 This is probably related to the immunological stress generated by vaccination, which may alter the growth kinetics of the target tumor and even the course of the disease without preventing recurrence. 95 These results indicate that TLPLDCV treatment may require time to achieve full efficacy. Moreover, researchers suggested that patients with early recurrence may not be ideal candidates for vaccine monotherapy because such more aggressive tumor biology usually does not respond to cancer vaccines. 96 TLPLDCV has been planned to be further tested in a phase III RCT.
Compared with conventionally used tumor-associated antigen-based vaccines, neoantigen-based vaccines have the advantage of better tumor specificity and tolerability. Moreover, the augmented neoantigen-specific T-cell responses mediated by these vaccines are likely to be sustained and provide post-treatment immunological memory, which has the potential to provide long-term protection against disease recurrence. 97 It was also reported that neoantigen-based vaccines may be able to transform ‘cold’ tumors into ‘hot’ tumors and induce upregulation of PD-L1 in the tumor microenvironment, which allows the extension of anti-PD-1/PD-L1 therapy to patients without a pre-existing T-cell response. This is especially attractive for patients with a low TMB who are unlikely to benefit from PD-1/PD-L1 inhibitors. 14 In the NT-001 trial, nine unresectable melanoma patients receiving nivolumab + neoantigen-based vaccine (NEO-PV-01) combination therapy showed major pathological remission, and three of them had a tumor load of more than 80% before therapy. However, prior to vaccination, these patients did not benefit from nivolumab monotherapy. 98 The trial also showed us that neoantigen-specific CD4+ and CD8+ T cells have a cytotoxic phenotype and are able to traffic to tumors which is associated with a prolonged DFS. 98 These results demonstrated the feasibility and tolerability of NEO-PV-01 in combination with nivolumab for the treatment of melanoma. However, NT-001 is a single-arm, non-RCT, and more studies are required to further refine and validate this therapy.
Although vaccines have shown great promise in melanoma treatment, their development and clinical application still facing many challenges. Vaccines can be expensive and it may take 3–4 months from the start vaccines production to administration. How to reduce manufacturing time and lowering the cost has been an critical challenge in broadening vaccine application. 99 Furthermore, although large numbers of T cells targeting certain neoantigens were detected, many vaccines induced only low frequency T-cell responses. Therefore, another challenge in the field of cancer vaccines is how to induce maximal activation and expansion of T-cell responses.98,100 In addition, sequence of ICIs and vaccine administration also should be carefully considered, as a preclinical study has demonstrated that inappropriate timing of dosing may lead to treatment failure. 101
Neoadjuvant therapy
In recent years, there has been an increasing interest in neoadjuvant therapy for melanoma. In contrast to adjuvant therapy, neoadjuvant therapy allows clinicians to adjust treatment regimens timely based on the patient’s response to therapy. 102 Combi-Neo trial demonstrated that dabrafenib + trametinib combination is a highly effective neoadjuvant treatment option and can provide substantial survival benefits for patients with BRAF mutation-positive stage III-IV melanoma. 103 In addition, several clinical trials have shown that the combination of nivolumab + ipilimumab is more efficient as neoadjuvant treatment than as an adjuvant in melanoma, but also resulted in more adverse effects.104,105 The subsequent OpACIN-neo trial further identified a better-tolerated neoadjuvant dosing regimen for the nivolumab + ipilimumab combination therapy in stage III melanoma. 106 It is foreseeable that with the further development and refinement of neoadjuvant treatment options, neoadjuvant therapy will make a profound impact on the treatment of high-risk resected melanoma.
Conclusion
For resected stage III-IV BRAF wild-type melanoma, nivolumab and pembrolizumab appear to be the most preferable adjuvant therapies; for BRAF mutation-positive melanoma, more RCTs are still required to find out which is better between ICIs and targeted therapy.
Supplemental Material
sj-docx-1-tam-10.1177_17588359221148918 – Supplemental material for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359221148918 for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis by He Ba, Fangyuan Zhu, Xiaoze Zhang, Zubing Mei and Yaodong Zhu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359221148918 – Supplemental material for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis
Supplemental material, sj-docx-2-tam-10.1177_17588359221148918 for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis by He Ba, Fangyuan Zhu, Xiaoze Zhang, Zubing Mei and Yaodong Zhu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359221148918 – Supplemental material for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis
Supplemental material, sj-docx-3-tam-10.1177_17588359221148918 for Comparison of efficacy and tolerability of adjuvant therapy for resected high-risk stage III-IV cutaneous melanoma: a systemic review and Bayesian network meta-analysis by He Ba, Fangyuan Zhu, Xiaoze Zhang, Zubing Mei and Yaodong Zhu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.