
Abstract
Background:
Adjuvant therapy is used to reduce the risk of hepatocellular carcinoma (HCC) recurrence and improve patient prognosis. Exploration of treatment strategies that are both efficacious and safe has been extensively performed in the recent years. Although donafenib has demonstrated good efficacy in the treatment of advanced HCC, its use as adjuvant therapy in HCC has not been reported.
Objectives:
To investigate the efficacy and safety of postoperative adjuvant donafenib treatment in patients with HCC at high-risk of recurrence.
Design:
Retrospective study.
Methods:
A total of 196 patients with HCC at high-risk of recurrence were included in this study. Of these, 49 received adjuvant donafenib treatment, while 147 did not. Survival outcomes and incidence of adverse events (AEs) in the donafenib-treated group were compared. Inverse probability of treatment weighting (IPTW) method was used.
Results:
The median follow-up duration was 21.8 months [interquartile range (IQR) 17.2–27.1]. Before IPTW, the donafenib-treated group exhibited a significantly higher 1-year recurrence-free survival (RFS) rate (83.7% versus 66.7%, p = 0.023) than the control group. Contrarily, no significant difference was observed in the 1-year overall survival (OS) rates between the two groups (97.8% versus 91.8%, p = 0.120). After IPTW, the 1-year RFS and OS rates (86.6% versus 64.8%, p = 0.004; 97.9% versus 89.5%, p = 0.043, respectively) were higher than those in the control group. Multivariate analysis revealed that postoperative adjuvant donafenib treatment was an independent protective factor for RFS. The median duration of adjuvant donafenib treatment was 13.6 (IQR, 10.7–18.1) months, with 44 patients (89.8%) experienced AEs, primarily grade 1–2 AEs.
Conclusion:
Postoperative adjuvant donafenib treatment effectively reduced early recurrence among patients with HCC at high-risk of recurrence, while exhibiting favorable safety and tolerability profile. However, these findings warrant further investigation.
Plain language summary
Why was this study done? Donafenib is the only new-generation targeted drug developed in the past 14 years that has demonstrated superior efficacy and increased safety in the first-line treatment of HCC. We aimed to explore whether postoperative adjuvant donafenib can improve the prognosis of patients with HCC at high-risk of recurrence. What did the researchers do? Medical data of patients with HCC at high-risk of recurrence who underwent radical resection at two medical centers between April 2021 and October 2022 were collected to compare long-term outcomes of patients treated with and without donafenib and explore the safety of adjuvant donafenib treatment. What did the researchers find? A total of 196 patients with HCC at high-risk of recurrence, including 49 who received adjuvant donafenib treatment and 147 who did not, were analyzed. At a median follow-up of 21.8 months, it was observed that adjuvant donafenib treatment effectively reduced early recurrence among patients with HCC at high-risk of recurrence, while exhibiting favorable safety and compliance profiles. What do the findings mean? The study provides real-world clinical empirical data on adjuvant donafenib treatment for patients with HCC at high-risk of recurrence, and these results may provide new directions for adjuvant treatment of HCC.
Introduction
Hepatocellular carcinoma (HCC) is a prevalent malignant tumor with poor prognosis. 1 Advancements in surveillance protocols and diagnostic techniques has led to an increase in the proportion of patients diagnosed with early HCC, allowing more patients to benefit from radical resection. Unfortunately, the recurrence rate of HCC can be as high as 70% within 5 years of radical resection, which may be related to existence of micrometastases or hidden residual disease. 2 Tumor recurrence is the leading cause of death and a vital bottleneck hindering the long-term survival of patients with HCC.
Postoperative HCC recurrence is clinically categorized as ‘early’ or ‘late’. 3 Early recurrence occurs within 2 years of radical resection and is typically attributed to intrahepatic metastasis of postoperative micrometastatic lesions. Conversely, late recurrence, which occurs after 2 or more years of radical resection, is generally attributed to the development of a de novo tumor. 3 Various risk factors reportedly contribute to distinct recurrence patterns. Numerous studies have demonstrated that early HCC recurrence is often associated with invasion-related characteristics of the primary tumor, such as tumor size >5.0 cm, multiple tumors, presence of microvascular invasion (MVI), poor differentiation, satellite nodules, and elevated serum alpha-fetoprotein (AFP) level.3–8 In contrast, late recurrence is contemplated to mainly occur due to the etiology of HCC (e.g. viral hepatitis) and the state of underlying liver parenchyma.6–10 It is noteworthy that early recurrence in patients with HCC is typically linked to worse long-term outcomes compared to late recurrence. 11 Furthermore, long-term outcomes of patients with early recurrence are contingent on the number of high-risk recurrence factors present during surgery.11,12 With the increasing recognition of the correlation between high recurrence and long-term outcomes of HCC, the development of new therapeutic drugs and other combined programs to reduce or delay recurrence has been extensively researched in recent years.
Donafenib is a novel, oral, small-molecule multikinase inhibitor that effectively suppresses the activity of several receptor tyrosine kinases and various Raf kinases, thereby exerting dual inhibitory and multitarget blocking antitumor effects. 13 In the ZGDH3 trial, donafenib has demonstrated encouraging outcomes in advanced HCC, with improved overall survival (OS) observed in patients receiving donafenib compared to those treated with sorafenib [hazard ratio (HR), 0.831; 95% confidence interval (CI), 0.699–0.988, p = 0.0245]. 14 In addition, donafenib also exhibited a better safety and tolerability profile than sorafenib. These favorable results may indicate the potential benefit of postoperative adjuvant donafenib; however, as an emerging targeted drug, the efficacy and safety of adjuvant donafenib treatment in patients at high-risk of recurrence after radical resection have not been reported. Whether donafenib can provide more possibilities for reducing tumor recurrence and improving long-term outcomes after radical resection remains to be investigated.
Therefore, we conducted this retrospective study to investigate the efficacy and safety of postoperative adjuvant donafenib treatment in patients with HCC at high-risk of recurrence.
Methods
Patients
In this study, we retrospectively reviewed the data of patients with HCC who underwent hepatectomy at the First Affiliated Hospital of the University of Science and Technology of China and the No. 2 People’s Hospital of Fuyang City between April 2021 and October 2022.
Patients who met the following inclusion criteria were incorporated in the study: (1) HCC confirmed by postoperative pathological examination and complete resection of all tumor nodules with negative incisional margins; (2) Child–Pugh class A or B7; (3) Eastern Cooperative Oncology Group performance status score of 0; (4) no previous antitumor treatment (except anti-hepatitis virus treatment); (5) no tumor thrombus, lymph node metastasis, or extrahepatic metastasis; and (6) at least one of the following high-risk recurrence factors: (1) single lesion >5 cm or multiple lesions of any size, (2) presence of MVI, and (3) presence of satellite nodules. The aforementioned high-risk recurrence factors were defined based on previous studies.4–8
The exclusion criteria were: (1) absence of high-risk recurrence factors; (2) other antitumor therapies after radical resection, except anti-hepatitis virus treatment, donafenib, and transarterial chemoembolization (TACE); (3) heart, lung, brain, or renal insufficiency or severe liver insufficiency (Child–Pugh class beyond B7); (4) death or tumor recurrence within 2 months; and (5) follow-up with insufficient data.
The retrospective variables included patient factors, laboratory parameters, tumor characteristics, and treatment.
Postoperative adjuvant treatment
All patients with hepatitis virus-related HCC received postoperative antiviral treatment, and some patients received one cycle of prophylactic TACE for approximately a month after radical resection. In the donafenib group, donafenib (initial dose of 100 or 200 mg, twice daily) was initiated at the first postoperative review (generally within 2 months) and continued until tumor recurrence, serious AEs, or spontaneous discontinuation. Suspension or dose reduction (100 mg, once daily) was allowed to alleviate serious AEs.
Follow-up and clinical assessment
Regular follow-ups were conducted for all patients postoperatively, and data was obtained from patient charts or telephonic interviews. Follow-ups were performed every 2–3 months for 2 years, and subsequently every 6 months. Follow-up included the following examinations: complete blood count, chemistry panel, serum tumor markers, imaging, and AEs. In some instances, additional imaging of other areas was performed to exclude extrahepatic metastases. The outcomes of this study included short-term survival prognosis of patients in both groups and the incidence of AEs, specifically in the donafenib group.
The 1-year recurrence-free survival (RFS) rate referred to the cumulative percentage of patients who did not experience recurrence or death within 1 year of achieving radical resection status. The 1-year OS rate was defined as the cumulative percentage of patients who remained alive within 1 year of achieving radical resection status. AEs were assessed according to the National Cancer Institute Standards for Common Terminology for Adverse Events, version 5.0. The course of treatment following tumor recurrence is contingent upon both the patterns of tumor recurrence and the physical condition of the patient.
Statistical analysis
To minimize selection bias in this retrospective study and avoid reduction in the overall population, we performed inverse probability of treatment weighting (IPTW) analysis for the two groups. Briefly, we used a logistic regression model to generate a propensity score for the probability of each patient receiving donafenib treatment, and a pseudo-population was created in which donafenib exposure was independent of covariates. In this larger pseudo-population, adjuvant donafenib treatment was randomly assigned. Seventeen possible clinically relevant confounders were included in the model: age, sex, hepatitis status, cirrhosis, alanine aminotransferase, aspartate aminotransferase (AST), platelet, bilirubin–albumin (ALBI) grade, AFP level, Edmondson–Steiner grade, margin, tumor capsule, tumor diameter, number of tumors, MVI, satellite nodules, and TACE.
The baseline characteristics of the patients were reported as mean ± standard deviation, median with interquartile range (IQR), or percentage (%), depending on the nature of the retrospective data. Independent-sample t tests or Mann–Whitney tests were used to analyze continuous variables, whereas Chi-square or Fisher’s exact tests were used to analyze categorical variables. RFS and OS were estimated using Kaplan–Meier curves, and differences between the groups were assessed using log-rank tests. A multivariate Cox proportional hazards regression model was used to examine the independent prognostic factors related to RFS and OS. R software (version 4.2.2; R Foundation, Vienna, Austria) was used to perform all the statistical analyses. A p value of <0.05 was considered statistically signifcant.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement (Supplemental Table 1). 15
Results
Baseline characteristics of the patients
A total of 479 patients with HCC underwent radical resection between April 2021 and October 2022. Of these, 283 patients were precluded on the basis of the exclusion criteria. Finally, this study enrolled 196 patients, of whom 49 received postoperative adjuvant donafenib treatment and 147 did not (Figure 1). The study population was predominantly male (85.2%), and the median age of the study participants was 59 years (IQR 52–68 years). Most patients had chronic liver disease (viral hepatitis, 85.7%; cirrhosis, 76.5%), good preoperative liver function reserve (ALBI grade 1, 55.6%, ALBI grade 2, 44.4%), and Barcelona Clinic Liver Cancer (BCLC) stage A (90.3%). In terms of tumor characteristics, the median tumor size was 6.0 cm (IQR 4.0–9.0), and most patients had a single tumor (85.2%). A small number of patients (33.7%) underwent adjuvant TACE following resection. Before IPTW, the proportion of patients with MVI in the donafenib-treated group was higher than that in the control group (85.7% versus 66.7%, p = 0.011). After weighing, a pseudo-population was created (donafinil-treated group, n = 182.29; control group, n = 196.46). The baseline characteristics of the two groups were generally well-balanced, as is shown in Table 1.

Patient selection flow.
Baseline characteristics of the patients.

AFP, alphafetoprotein; ALBI, bilirubin–albumin grade; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer stage; IPTW, inverse probability of treatment weighting; PLT, platelet; SD, standard deviation.
Survival analysis
All the 196 patients were included in the survival analysis. The median follow-up durations in the donafenib-treated and control groups were 21.1 (IQR 18.7–24.7) and 22.3 (IQR 16.7–28.3) months, respectively. Throughout the follow-up period, 86 recurrent events (14 in the donafenib-treated group and 72 in the control group) and 32 deaths (4 in the donafenib-treated group and 28 in the control group) occurred. The donafenib-treated group exhibited a significantly higher 1-year RFS rate (83.7% versus 66.7%, p = 0.023) than the control group. In comparison, no significant difference was found in the 1-year OS rates between the two groups (97.8% versus 91.8%, p = 0.120) [Figure 2(a) and (b)]. The median RFS in the control group was 22.3 months, which was not attained in the donafenib-treated group. After IPTW, both the 1-year RFS rate (86.6% versus 64.8%, p = 0.004) and the 1-year OS rate (97.9% versus 89.5%, p = 0.043) were higher in the donafenib-treated than those in the control group [Figure 2(c) and (d)]. The median RFS of the control group was 18.3 months, which was not reached in the donafenib-treated group.

Kaplan–Meier analysis of RFS and OS between the two groups. Before IPTW (a, b). After IPTW (c, d).
In the context of location of recurrence, most patients in both the groups predominantly experienced intrahepatic recurrence (Table 2). On the other hand, the proportion of patients with extrahepatic recurrence or a combination of intrahepatic and extrahepatic recurrence was similar (p = 0.826). With the exception of a few patients lost to follow-up, the remaining patients in the study received further treatment after recurrence. Furthermore, patients who experienced recurrence received similar rates of various treatments in both groups (p = 0.805).
Location and treatment of recurrent hepatocellular carcinoma.

ICI, immune checkpoint inhibitor; TKI, tyrosine kinase inhibitor.
Prognostic factors of RFS and OS
Before IPTW, the outcomes of multivariate analysis indicated that AST (HR, 1.009; 95% CI, 1.003–1.014, p = 0.003), tumor diameter (HR, 1.886; 95% CI, 1.198–2.968, p = 0.006), tumor capsule (HR, 1.657; 95% CI, 1.085–2.530, p = 0.019), MVI (HR, 2.419; 95% CI, 1.423–4.111, p = 0.001), and postoperative adjuvant donafenib (HR, 0.362; 95% CI, 0.204–0.642, p < 0.001) were independent prognostic factors related to RFS (Table 3). On the other hand, tumor diameter (HR, 5.463; 95% CI, 1.905–15.665, p = 0.002) was the only independent prognostic factor related to OS (Table 4).
Univariable and multivariable analyses of RFS before IPTW.

AFP, alphafetoprotein; ALBI, bilirubin–albumin grade; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer stage; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; PLT, platelet; RFS, recurrence-free survival; TACE, transarterial chemoembolization.
Univariable and multivariable analyses of OS before IPTW.

AFP, alphafetoprotein; ALBI, bilirubin–albumin grade; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer stage; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; OS, overall survival; PLT, platelet; TACE, transarterial chemoembolization.
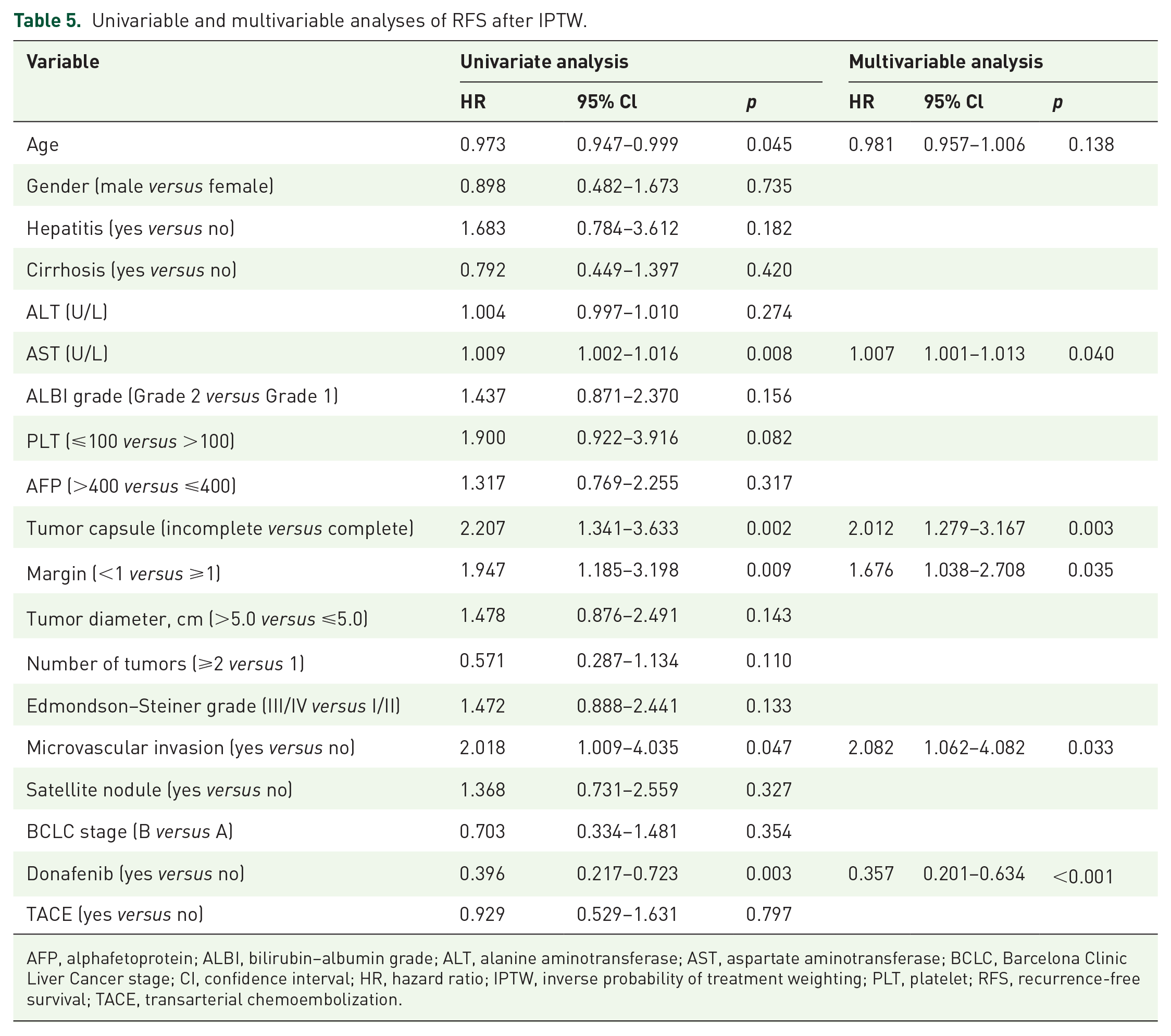
After IPTW, AST (HR, 1.007; 95% CI, 1.001–1.013, p = 0.040), tumor capsule (HR, 2.012; 95% CI, 1.279–3.167, p = 0.003), margin (HR, 1.676; 95% CI, 1.038–2.708, p = 0.035), MVI (HR, 2.082; 95% CI, 1.062–4.082, p = 0.033), and postoperative adjuvant donafenib (HR, 0.357; 95% CI, 0.201–0.634, p < 0.001) were found to be independent prognostic factors related to RFS (Table 5). On the other hand, AFP (HR, 2.345; 95% CI, 1.132–4.861, p = 0.022), tumor diameter (HR, 7.148; 95% CI, 2.344–21.799, p = 0.001), and postoperative adjuvant donafenib (HR, 0.257; 95% CI, 0.201–0.634, p = 0.013) were independent prognostic factors related to OS (Table 6).
Univariable and multivariable analyses of RFS after IPTW.
AFP, alphafetoprotein; ALBI, bilirubin–albumin grade; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer stage; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; PLT, platelet; RFS, recurrence-free survival; TACE, transarterial chemoembolization.
Univariable and multivariable analyses of OS after IPTW.

AFP, alphafetoprotein; ALBI, bilirubin–albumin grade; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer stage; CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; OS, overall survival; PLT, platelet; TACE, transarterial chemoembolization.
Adverse events
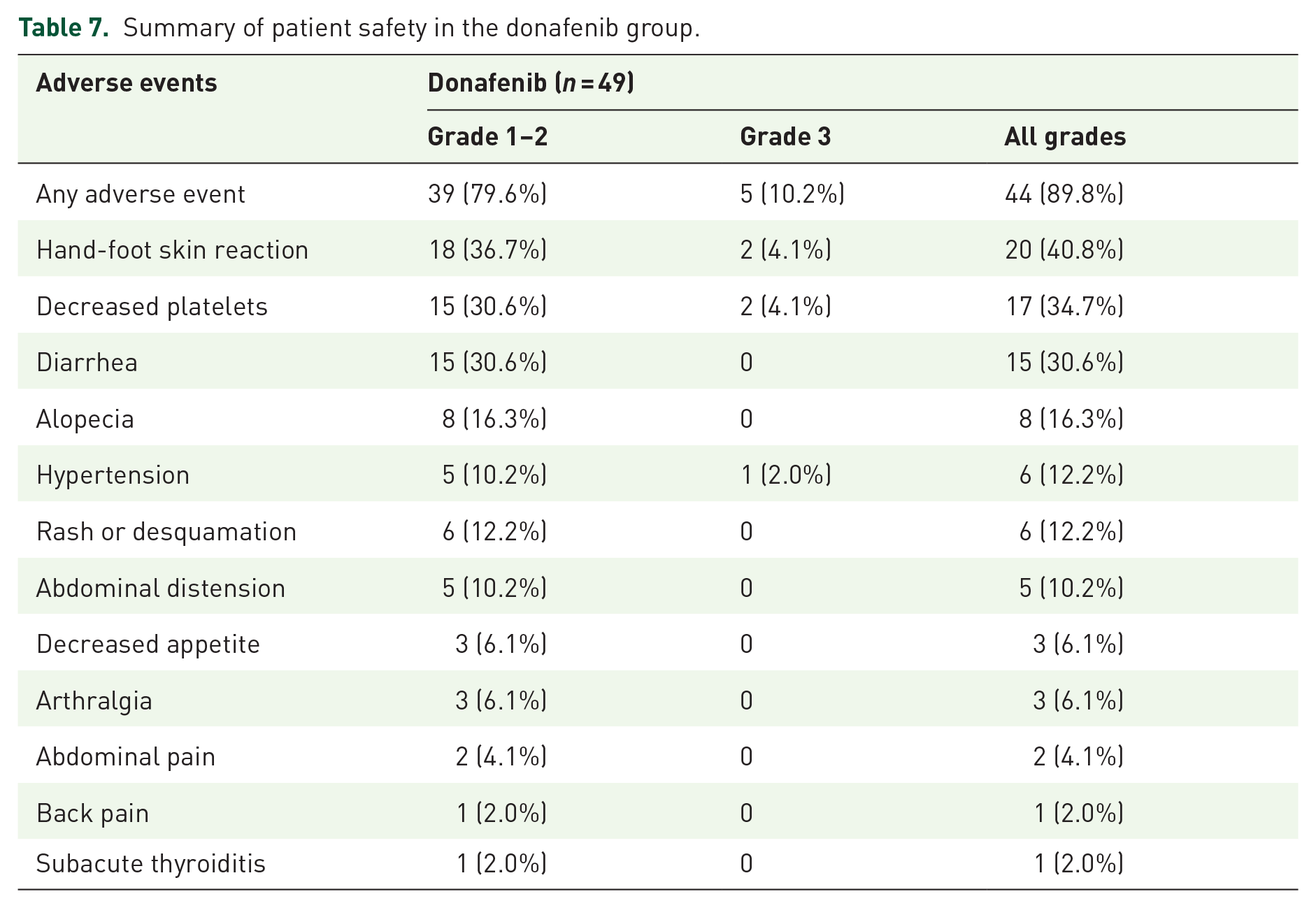
The median duration of adjuvant donafenib treatment was 13.6 (IQR 10.7–18.1) months, with 34 patients initiating treatment with half the dose (100 mg, twice daily) and 15 commencing treatment with the full dose (200 mg, twice daily). Among these patients, 46 (93.9%) completed a treatment cycle lasting longer than 6 months, with only three discontinued treatment due to recurrence within this timeframe. Furthermore, eight (16.3%) patients required dose modifications, while four (8.2%) discontinued treatment due to severe AEs. AEs mainly occurred within 3 months after treatment, and 44 patients (89.8%) experienced AEs, predominantly grade 1–2. Contrarily, five (10.2%) patients experienced grade 3 AEs. The most commonly observed AEs included hand-foot skin reactions [20 (40.8%)], decreased platelet count [17 (34.7%)], and diarrhea [15 (30.6%)] (Table 7).
Summary of patient safety in the donafenib group.
Discussion
Long-term survival is expected in ‘potentially cured’ patients who undergo radical resection. However, the high postoperative recurrence rate remains a significant bottleneck in achieving this goal. The core purpose of postoperative adjuvant treatment is to decrease or delay tumor recurrence and metastasis. Moreover, it is also aimed at improving the long-term outcomes of patients, including treatment against the background of chronic liver disease (such as treatment of viral hepatitis) and eradication of micrometastatic tumor deposits. 16 Active intervention to decrease and delay tumor recurrence is not only vital for improving the overall curative effect in patients with HCC, but is also an area of urgent medical demand. Recently, in the interim analysis of IMbrave050, the median follow-up duration was 17.4 months. Among patients at high-risk of recurrence, RFS was improved in those who received a combination of atezolizumab and bevacizumab in comparison to those who underwent active surveillance (HR, 0.72; 95% CI, 0.53–0.98, p = 0.012). 17 While further follow-up is required to confirm the effectiveness of adjuvant treatment using a combination of atezolizumab and bevacizumab as a milestone in the treatment of HCC, IMbrave050 proved the necessity of postoperative adjuvant treatment and identified patients at high-risk of recurrence as a potential target population.
Over the last decade, targeted drugs have emerged as crucial treatment options for management of patients with advanced HCC due to their distinctive mechanisms of action and noteworthy effectiveness. 18 From a theoretical point of view, the anti-angiogenic and inhibitory effects of targeted drugs on tumor cell proliferation may render them an optimal choice for management of postoperative micrometastases. Using luciferase-labeled orthotopic xenograft mice models of HCC, Feng et al. 19 demonstrated that sorafenib reduced postoperative tumor recurrence, consequently leading to prolonged survival of mice. The lack of success in the STORM trial has diminished the faith of the researchers in targeted monotreatment. 20 However, it is essential to note that the trial included a patient population with relatively low risk of recurrence, as was evidenced by a median tumor size of 3.5 cm and by the fact that 32% patients had MVI. Therefore, the potential role of antiangiogenic activity in preventing or reducing tumor recurrence must be reconsidered. Conversely, several real-world studies have demonstrated that adjuvant-targeted treatment following radical resection is effective in reducing the rates of postoperative tumor recurrence and metastasis.21–25 Recently, a phase II clinical study showed that the median RFS of patients treated with adjuvant apatinib after radical resection for HCC with portal vein tumor thrombosis was 7.6 months and that the 1-year RFS rate was 36.1%. 26 Similarly, Zhou et al. 27 showed that in the patients with China liver cancer staging IIb/IIIa (equal to BCLC stage B/C) treated with lenvatinib after radical resection, the 1-year RFS rate was 50.5% and the median RFS was 16.5 months.
While the potential effects on OS remain to be further investigated, these favorable results further emphasize the value of adjuvant-targeted treatment. As a deuterated derivative of sorafenib, donafenib is the only new-generation targeted drug developed in the past 14 years that has superior efficacy and increased safety in the first-line treatment of HCC. The remarkable efficacy of donafenib in the treatment of advanced HCC highlights the need for further research in the field of adjuvant treatment. In the present study, we included patients with HCC at higher risk of recurrence (median tumor size, 6.0 cm; 71.4% of patients with MVI) than the STORM trial. Survival analysis indicated that adjuvant donafenib treatment effectively reduced early tumor recurrence in patients at high-risk of recurrence (1-year RFS rate, 83.7% versus 66.7%, p = 0.023). Up to the last follow-up, most patients in both the groups in our study predominantly experienced intrahepatic recurrence, and no difference in the location of recurrence was observed. Considering the imbalance in significant prognostic factors related to RFS and the limited sample size, we constructed a pseudo-population using IPTW and observed similar outcomes. A consistent trend of superior OS with donafenib compared to sorafenib was reportedly observed in various predefined subgroups, with significant improvements in OS achieved in specific subgroups. 14 In our study, 162 patients (82.7%) had hepatitis B virus-related HCC, and therefore, adjuvant donafenib may have been more targeted and effective. Before IPTW, no significant improvement in OS was observed in the donafenib-treated group. However, after IPTW, the donafenib-treated group exhibited better OS than the control group. Furthermore, multivariate analysis indicated that postoperative adjuvant donafenib treatment was an independent and favorable factor for OS. The different OS outcomes between the two datasets could be attributed to limited sample size and short follow-up duration. However, the specific effects of postoperative adjuvant donafenib treatment on OS requires further investigation.
Both efficacy and safety are critical, with ‘efficient yet tolerable’ as the paramount aim of postoperative adjuvant treatment. In particular, in cases of early HCC in the absence of active disease, the patient’s acceptance of adverse reactions is further reduced, which leads to poorer adherence. Compared with atezolizumab plus bevacizumab therapy in IMbrave050, donafenib monotherapy is expected to exhibit more favorable safety. Moreover, the oral route of administration of donafenib is more convenient for patients. Throughout the course of treatment, adjuvant donafinib showed favorable safety and adherence. The overall incidence of AEs was 89.8%, most of which were grade 1 or 2. Commonly occurring AEs were consistent with the known safety profile of targeted monotherapy, with no new safety concerns being identified. In the context of compliance, 46 patients (93.9%) received continuous treatment for more than 6 months, while 5 (10.2%) discontinued treatment due to the occurrence of grade 3 AEs. AEs were further controlled and reversed through flexible adjustments such as drug suspension, dose adjustment, and symptom management.
To the best of our knowledge, this is the first study to report the efficacy and safety of adjuvant donafenib treatment for patients with HCC at high-risk of recurrence. Moreover, the preliminary findings showed a favorable trend. However, this retrospective study had some limitations that need consideration. First, numerous high-risk factors are associated with HCC recurrence. In this study, four routine factors were chosen based on prior research to identify patients at high-risk of recurrence, thereby introducing a selection bias within the study population. Previous studies have indicated that patients at high-risk of recurrence are more likely to derive substantial benefits from postoperative adjuvant treatment. Nevertheless, current studies commonly use composite criteria encompassing variables such as tumor size and MVI to identify high-risk patients, which may lead to the omission of potentially beneficial patients. Second, donafenib has been in the market for a short time, which resulted in a smaller sample size and shorter follow-up duration. Further conclusions regarding survival benefit may only be derived from a randomized control trial. How this may also ultimately compare to atezolizumab/bevacizumab is also unclear.
Conclusion
In conclusion, surgery should be combined with numerous cutting-edge drugs to prolong the survival and improve the quality of life of patients with HCC. Individualized adjuvant treatment based on the risk of recurrence is an important direction for future studies. Based on the preliminary findings of this study, it can be inferred that postoperative adjuvant donafenib treatment effectively reduced early recurrence among patients with HCC at high-risk of recurrence, while exhibiting favorable safety and tolerability profile. Nevertheless, additional extensive randomized controlled trials are necessary to validate our findings.
Supplemental Material
sj-docx-1-tam-10.1177_17588359241258394 – Supplemental material for Adjuvant donafenib for hepatocellular carcinoma patients at high-risk of recurrence after radical resection: a real-world experience
Supplemental material, sj-docx-1-tam-10.1177_17588359241258394 for Adjuvant donafenib for hepatocellular carcinoma patients at high-risk of recurrence after radical resection: a real-world experience by Shenyu Zhang, Guibin Yang, Ruipeng Song, Wei Wang, Fanzheng Meng, Dalong Yin, Jiabei Wang, Shugeng Zhang, Wei Cai, Yao Liu, Dayong Luo, Jizhou Wang and Lianxin Liu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.