
Abstract
Background:
Patients with non-small cell lung cancer (NSCLC) presenting with mesenchymal–epithelial transition (MET) exon 14 skipping mutation have an unfavorable prognosis with standard treatments. Capmatinib is a selective MET inhibitor, which showed promising efficacy in this patient population in early trials.
Methods:
We performed a retrospective, international, multicenter efficacy and safety analysis in patients with NSCLC treated with capmatinib in an early access program between March 2019 and December 2021.
Results:
Data from 81 patients with advanced MET exon 14 mutated NSCLC treated with capmatinib in first- or later-line therapy were analyzed. Median age was 77 years (range, 48–91), 56% were women, 86% had stage IV disease, and 27% had brain metastases. For all patients, the objective response rate (ORR) to capmatinib was 58% (95% CI, 47–69), whereas it was 68% (95% CI, 50–82) in treatment-naïve and 50% (95% CI, 35–65) in pretreated patients. The median progression-free survival was 9.5 months (95% CI, 4.7–14.3), whereas it was 10.6 months (95% CI, 5.5–15.7) in first-line and 9.1 months (95% CI, 3.1–15.1) in pretreated patients. After a median follow-up of 11.0 months, the median overall survival was 18.2 months (95% CI, 13.2–23.1). In patients with measurable brain metastases (n = 11), the intracranial ORR was 46% (95% CI, 17–77). Capmatinib showed a manageable safety profile. Grade ⩾ 3 treatment-related adverse events included peripheral edema (13%), elevated creatinine (4%), and elevated liver enzymes (3%).
Conclusion:
In patients with MET exon 14 skipping mutation, capmatinib showed durable systemic and intracranial efficacy and a manageable safety profile. This analysis confirms previously reported phase II data in a real-world setting.
Introduction
During the last decade, remarkable progress has been made in the personalized treatment of non-small cell lung cancer (NSCLC), which is the most frequent type of lung malignancy, accounting for 84% of all lung cancer diagnoses.1,2
The c-mesenchymal–epithelial transition proto-oncogene – known as c-MET or MET – encodes for a receptor tyrosine kinase expressed mainly by epithelial cells and promotes tissue proliferation and regeneration. 3 Aberrant MET signaling leads to increased cell proliferation and survival, invasion, and metastasis. 4 In cancers with MET exon 14 skipping, the transcription process of the MET gene is disrupted by underlying genomic alterations that affect the splice site regions of exon 14 leading to in-frame deletion of exon 14 and a shortened MET receptor3–7 with increased stability and thus sustained activation of MET signaling, which enhances tumor growth. 8 Several alterations of the MET gene have been identified, including point mutations and small deletions that may occur at different positions. 9
MET exon 14 skipping mutations are the most frequently reported oncogenic MET variant and typically occur in the absence of other driver mutations. 7 They are observed in about 3–4% of NSCLC cases10,11 and are associated with an unfavorable prognosis with standard treatments. 12 This alteration seems to be more frequent in elderly patients, females, and never smokers. 13 Brain metastases are observed in up to 40% of NSCLC patients, including those with MET exon 14 skipping mutations. 14
In the last two decades, MET-targeting small-molecule kinase inhibitors, conventional therapeutic monoclonal antibodies, and antibody-based biotherapeutics led mainly to disappointing outcomes in preclinical and clinical trials.15,16 Different MET-targeted therapies are currently under investigation, including monoclonal antibodies against MET or its ligand [hepatocyte growth factor (HGF)], 17 and small-molecule MET inhibitors. The role and efficacy of immune-checkpoint inhibitors in treatment of patients with MET exon skipping 14 mutations is still unclear. Despite high programmed death-ligand 1 (PD-L1) expression, those patients might not benefit from immune-checkpoint inhibitor treatment due to lower tumor mutational burden compared with unselected NSCLC.9,18
Capmatinib is a potent and highly selective small molecule MET inhibitor, which has shown substantial and clinically meaningful antitumor activity in cancers presenting with various types of MET activation.8,19–21 Moreover, capmatinib is known to cross the blood–brain barrier and demonstrates intracranial efficacy in patients with NSCLC harboring MET exon 14 skipping mutations and presenting with brain metastasis.8,22 In the nonrandomized, open-label, multicenter, multicohort phase II GEOMETRY Mono-1 trial, capmatinib was investigated in patients with advanced NSCLC. 8 Treatment-naïve patients in the GEOMETRY Mono-1 trial showed an objective response rate (ORR) of 68% and a median progression-free survival (mPFS) of 12.4 months. In pretreated patients, an ORR of 41% and mPFS of 5.4 months were observed. The results indicate clinical benefit and a good safety profile in both treatment-naïve and previously treated patients.
Real-life data of MET exon 14 mutated patients treated with capmatinib outside of a clinical trial are scarce, and there is an urgent need for additional data in the real-world setting, particularly for patients with poorer performance status and for treatment-naïve patients. This retrospective study was based on international data from a capmatinib early access program (EAP) for patients with MET exon 14 mutated advanced NSCLC.
Methods
Study design
This is a retrospective, non-interventional, multicenter real-world analysis called Real-world Experience with Capmatinib (RECAP), which aims to evaluate the efficacy and safety of MET exon 14 mutated NSCLC patients treated with capmatinib within an EAP.
The primary endpoint of this retrospective data analysis was the ORR – proportion of patients with complete response (CR) and partial response (PR) defined according to RECIST v1.1 criteria. 23 The secondary endpoints were the following: (i) evaluation of treatment-related adverse events (TRAEs) determined by the treating physician; (ii) disease control rate (DCR) defined as the proportion of patients with CR, PR, and stable disease (SD); (iii) intracranial ORR (icORR); (iv) median duration of response (mDoR) assessed as the time between the initial response to therapy and subsequent disease progression or death due to any cause; (v) mPFS measured as the time from the first dose of capmatinib to the first progression event [progressive disease (PD) or death if no PD documented until then, irrespective of cause of death]; and (vi) median overall survival (mOS) defined as the time between date of diagnosis of advanced stage lung cancer and death.
Study population and treatment
Oncological and pneumological centers specialized in the treatment of lung cancer from seven different countries (Austria, France, Israel, The Netherlands, Slovenia, Sweden, and Switzerland) contributed to this dataset. Data from all eligible patients treated by physicians who participated in a capmatinib EAP were included. For inclusion, the following criteria had to be met: histologically confirmed NSCLC with locally advanced or metastatic disease, age ⩾18 years, confirmed MET exon 14 skipping mutation, treatment with capmatinib outside of a clinical trial (at least one dose), and at least one follow-up assessment of response using computed tomography (CT) and/or magnetic resonance imaging (MRI).
Next-generation sequencing (NGS)-based genomic profiling, Sanger sequencing, or polymerase chain reaction (PCR) from tissue and/or liquid biopsy were used for the identification of MET exon 14 skipping mutations. MET alterations were described with the reference sequences of MET variant 1 (NM_001127500.3) or the shorter variant 2 (NM_000245.3).
Capmatinib was taken orally (standard dose of 400 mg twice daily). Reduced starting dose, dose reductions, and re-escalations were decided at treating physicians’ discretion. Capmatinib treatment was continued until disease progression, lack of clinical benefit, unacceptable toxicity, patient’s withdrawal of consent, or the treating physicians’ decision.
Data collection
In 2019, capmatinib became available through an EAP for the treatment of patients with advanced NSCLC harboring a MET exon 14 skipping mutation who were not able to participate in a clinical trial and with limited other treatment options.
Clinical characteristics and treatment data were extracted from medical records, anonymized by the treating physicians and transferred for statistical analysis. Data included information about patients’ demographics and clinical characteristics [country, gender, date of birth, ethnicity, smoking and Eastern Cooperative Oncology Group (ECOG) performance status, disease stage, previous treatments, histology, MET mutation status, testing method, and co-mutations], capmatinib treatment (duration and dose, best response, as well as date, type, and location of progression), and drug safety.
Efficacy and safety assessments
According to clinical practice at each institution, a CT scan of the chest and abdomen performed every 6–12 weeks was used to evaluate tumor response and progression per RECIST v1.1. Additional brain CT and/or MRI assessment were done according to institutional standard of care.
In the overall population, as well as for each subgroup (treatment-naïve and pretreated patients), the following efficacy parameters were analyzed: ORR, DCR, duration of response (DoR), progression-free survival (PFS), and overall survival (OS). Tumor response (maximum change in tumor size) was compared through pretreatment lesion measurements performed at baseline and post-treatment (at least one imaging evaluation). For calculation of intracranial response, only patients with untreated or progressing brain lesions were included. Measurable brain lesion was defined as ⩾5 mm at baseline.
Adverse events (AEs) were graded as per Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Treatment relation of an AE to capmatinib was assessed by the treating physicians. Safety monitoring was performed at baseline, at every subsequent evaluation visit, or as clinically indicated. A documentation of each dose modification or interruption, as well as treatment discontinuations, related to TRAEs was done.
Ethics approval and informed consent
The study protocol was approved by the ethics committee of the city of Vienna, Austria (EK-21-239-1121). Informed consent was obtained in accordance with local legislation in the respective countries at each study side. According to Austrian laws, informed consent for each patient was not necessary for this retrospective analysis. The study was conducted according to the principles of the Declaration of Helsinki.
Statistical analysis
PFS, OS, and DoR have been analyzed using the Kaplan–Meier method and derived related 95% confidence intervals (CI). DoR was calculated for all patients who achieved CR or PR; if a patient died, irrespective of cause of death, without PD beforehand, then the date of death has been used as end date. Concerning the PFS, patients without any documented progression and who are alive at the time of data cut-off have been censored at time of data cut-off or last contact. Patients who initiated subsequent anticancer therapy in the absence of documented PD (e.g., discontinued treatment due to an AE) have been censored at time of treatment discontinuation. Data for patients who were lost to follow-up or alive have been censored for the OS at the date of last contact. Confidence interval for proportions, such as ORR and DCR, has been calculated using the exact Clopper–Pearson method. For a comparison of subgroups defined by previous lines of systemic anticancer therapy, a log-rank test with a level of significance of 5% (chi-square p = 0.05) has been used. Median follow-up time has been estimated using Kaplan–Meier estimate of potential follow-up (so-called reverse Kaplan–Meier method); standard errors of this method (e.g., due to ties) have been limited by RStudio packages (prodlim 2019.11.13, survival 3.2–13 and haven 2.4.3).
All statistical analyses have been conducted using SPSS software (v.27.0, IBM SPSS Statistics) and RStudio v.1.4.1106. Tables and figures have been created by using SPSS v.27.0 (IBM SPSS Statistics), Microsoft Excel 2019, and RStudio v.1.4.1106.
Results
Patients
We included 81 patients with locally advanced or metastatic MET exon 14 mutated NSCLC, receiving capmatinib whereas participating in an EAP with capmatinib between March 2019 and December 2021. Demographics, clinical, and pathological characteristics are presented in Table 1. The overall population enclosed 37 treatment-naïve and 44 pretreated patients. The median age was 77 years (range, 48–91). A greater number of females (56%) and only one patient (1%) of Asian ethnicity participated, whereas 43% of patients reported never smoking, the proportion of former smokers being 48%, and 9% currently smoking. Overall, 69% of patients presented with a good (0–1) ECOG performance status. A higher proportion of treatment-naïve patients had a poor performance status (ECOG ⩾2) compared with the pretreated group (43% versus 21%).
Demographics and characteristics of patients prior to capmatinib administration.

Data cut-off date: November 8, 2021.
Percentage may not be 100 because of rounding.
As defined by the National Lung Screening Trial. 24
ECOG performance status, with higher numbers indicating worse daily living capability.
One patient was treated in stage IIIa but with palliative intend and one patient was down-staged after capmatinib therapy.
Previous regimens defined as at least one dose of chemotherapy and/or immunotherapy or one dose of TKI; one patient received a combination of capmatinib and pembrolizumab; one patient received first osimertinib during 2.5 months before capmatinib was additionally administered; two patients received tepotinib (c-MET inhibitor) but had to stop the therapy because of adverse events and received then capmatinib; one patient received APL 101 (c-MET inhibitor).
Five patients received chemo- and anti-VEGF therapies.
One patient received immuno- and anti-TIGIT therapy. One patient received immunotherapy and lenvatinib.
TKIs administered include crizotinib (12 patients), cabozantinib (3 patients), tepotinib (2 patients), afatinib (1 patient), gefitinib (1 patient), and osimertinib (1 patient). Two patients received more than one prior TKI.
As already defined, most common clones used for PD-L1 testing were SP263 and 22C3. 17
Five patients were tested negative for MET exon 14 skipping mutation in tissue but positive in liquid biopsy.
Anti-PD-1, anti-cell death protein 1; anti-TIGIT, T-cell immunoreceptor with immunoglobulin and immunoreceptor tyrosine-based inhibitory motif domain; anti-VEGF, vascular endothelial growth factor; ECOG, Eastern Cooperative Oncology Group; NA, not applicable; NOS, not otherwise specified; NSCLC, non-small cell lung cancer; PCR, polymerase chain reaction; PD-L1, programmed death-ligand 1; EGFR, epidermal grow factor receptor; GCN, gene copy number; py, pack years; TKIs, tyrosine kinase inhibitors.
At the time when capmatinib treatment started, most patients (86%) had stage IV disease, and the most frequent site of metastasis was bones (36%), lung (35%), pleura (31%), and/or brain (27%). In total, 40% of patients presented with only a single-site metastatic lesion. Pretreated patients had received a median number of one therapeutic agent prior to capmatinib (range, 1–5). Prior regimens included platinum-based therapies (70%), anti-PD-1 (anti-cell death protein 1) or PD-L1 treatments (61%), and tyrosine kinase inhibitors (TKIs) (41%).
The majority of patients (78%) presented with an adenocarcinoma. The primary testing method of MET mutations was NGS in 98% of the cases, mainly from tissue only (77%). An alteration at the CBL binding-domain was reported in one patient. A MET exon 14 skipping was detected in 91% of patients. An associated MET splice site mutation was reported in 42%, mostly point mutations at the splice donor site [NM_001127500.3:c.3082G>Xp.(Asp1028X)] in 38% [alternative description NM_000245.3:c.3028G>Xp.(Asp1010X)], or splice donor site (3082+/3028+) in 32%, or further insertions and deletions (indels) at the splice acceptor site in 26%. In five patients (6%), MET mutation was only found in liquid biopsy sample but was negative in tissue. Reported co-mutations were mostly TP53 (9%), KRASG12C (2%), or an activating EGFR mutation (2%). In total, 80% of patients showed PD-L1 expression [tumor proportion score (TPS)> 1%] with 40% showing a highly positive (TPS ⩾ 50%) PD-L1 status.
Response
The efficacy results are presented in Table 2. The overall ORR was 58% (95% CI, 47–69), with two patients (3%) having CR and 45 patients (56%) having PR. Non-responders included 12 patients (15%) showing PD and 18 patients (22%) SD. Four patients (5%) had no measurable target lesion. Both CRs were observed among pretreated patients, but the proportion of PRs was higher in the treatment-naïve group (68% versus 45%, respectively). Treatment-naïve patients showed a better response rate (ORR, 68%; 95% CI, 50–82) than pretreated patients (ORR, 50%; 95% CI, 35–65) to capmatinib treatment. Median time to first response was 1.7 months in the overall population. The DCR reached 81% (95% CI, 70–88) in the overall population, 84% (95% CI, 68–94) in the untreated group, and 77% (95% CI, 62–89) in pre treated patients.
Efficacy of capmatinib in MET exon 14 skipping mutation positive patients.

Data cut-off date: November 8, 2021. ORR, PFS assessed according to RECIST v1.1 for patients with measurable disease.
Percentage may not equal to 100 because of rounding.
ORR was including complete or partial response.
DCR was including complete response, partial response, or stable disease.
PFS was calculated from start of therapy to progression or death independent of reason of death. Patients who have no documented progression and are alive at the time of data cut-off have been censored at time of data cut-off or last contact. Patients who initiate subsequent anticancer therapy in the absence of documented PD (e.g., discontinued treatment due to adverse events) have been censored at time of treatment discontinuation.
OS was calculated from start of capmatinib treatment to date of death independent of cause. Patients who are alive or lost to follow-up have been censored at last date known alive.
Only includes patients with measurable brain lesions ⩾5 mm and recent follow-up MRI or CT, who did not have prior intervention of brain metastasis, or prior intervention but progression of brain lesions before capmatinib start.
CI, confidence interval; CR, complete response; CT, computed tomography; DCR, disease control rate; (ic)DCR, (intracranial) disease control rate; (ic)ORR, (intracranial) ORR; MRI: magnetic resonance imaging; NR, not reached; ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease; TRAEs, treatment-related adverse events.
Maximum change in tumor size related to baseline of 75 patients (retrospective measurement of lesions was not possible for two patients) is shown in Figure 1(a).

Best response to capmatinib. Waterfall plots of maximum change in tumor size measured according to RECIST v1.1 in all target lesions between baseline and follow-up imaging in pretreated and treatment-naïve patients in the overall population (a) and in patients with baseline intracranial target lesions (b). Both growth (+20%) and shrinkage (−30%) of tumor size are indicated by the dashed lines.
The median DoR was still immature. The DoR for individual patients are presented in Supplemental Figure S1. At a median follow-up of 9.5 months, 70% (33 of 47) of the responses were ongoing.
Figure 2(a) shows the response to capmatinib according to the starting dose, PD-L1 expression, and TP53 status. A slightly higher response was observed among patients having received a full starting dose compared with reduced starting dose (ORR, 61% versus 50%) and showing PD-L1 ⩾ 50% (TPS) compared with PD-L1 < 50% (70% versus 52%). Patients presenting with MET exon 14 skipping mutation and TP53 co-mutation reached an overall ORR of 67% (95% CI, 30–93).
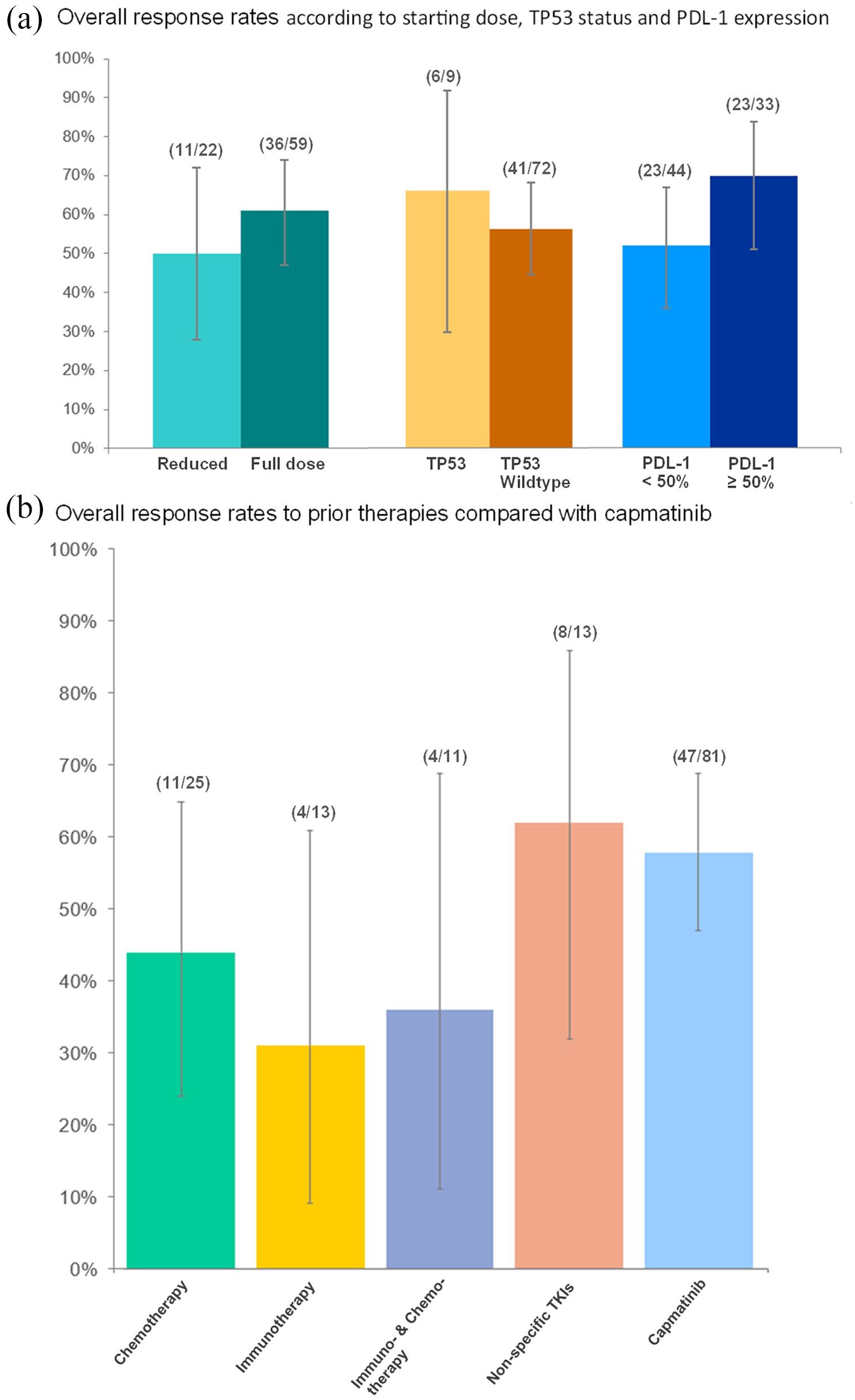
Comparison of response rates. (a) Response according to starting dose and molecular characteristics. (b) Response to prior therapies compared with capmatinib.
Figure 2(b) and Supplemental Table S1 show the ORR to prior therapies of pretreated patients compared to capmatinib. ORR to capmatinib and non-specific TKIs (crizotinib and cabozantinib) (ORR, 62%) were higher compared with chemotherapy (44%), chemoimmunotherapy (36%), or immunotherapy (31%). Higher DCR were observed for capmatinib (81% versus 76% for overall previously administered treatment) (Supplemental Table S1).
Progression-free survival and overall survival
After a median follow-up of 10.7 months, the mPFS was 9.5 months (95% CI, 4.7–14.3) in the overall population, 10.6 months (95% CI, 5.5–15.7) in the treatment-naïve, and 9.1 months (95% CI, 3.1–15.1) in the pretreated patients (Table 2, Figure 3(a) and (b)). At data cut-off, 43% of treatment-naïve patients and 59% of the previously treated patients had disease progression, which was mainly systemic (81% versus 46%, respectively) or an oligo-progression (6% versus 19%, respectively). Based on Kaplan–Meier analysis, PFS rate was 64% at 6 months and 38% at 1 year.
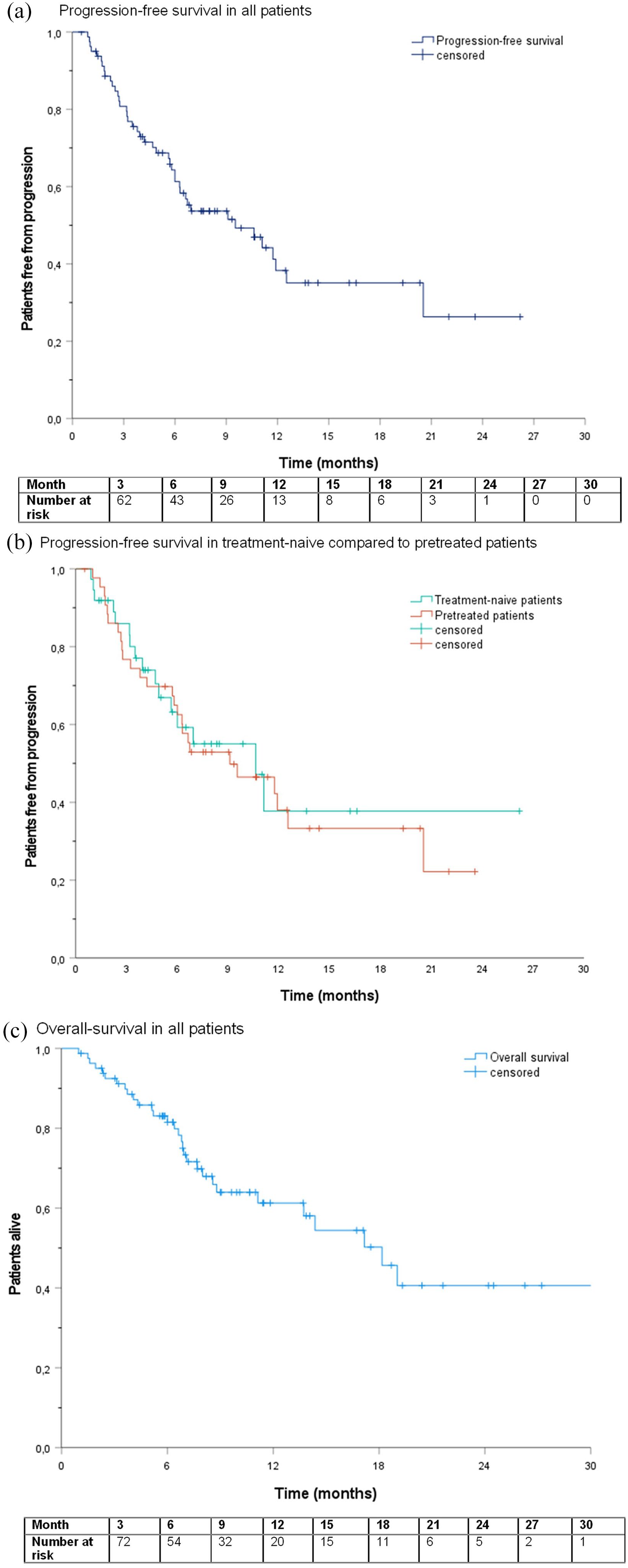
Progression-free survival (PFS) and overall survival (OS). Kaplan–Meier plots of median PFS in the overall population (a) and in previously treated and treatment-naïve patients (b), as well as of the median OS in the overall population (c).
The mOS was 18.2 months (95% CI, 13.2–23.1) after a median follow-up of 11.0 months (Figure 3(c)). In pretreated patients, the mOS reached 17.2 months (95% CI, 6.7–27.7), whereas the mOS was not reached in the treatment-naïve group (Table 2).
Intracranial outcome
At baseline 22 patients (27%) had confirmed brain lesions, 55% of them being asymptomatic (Table 2). The overall mPFS in these patients was 9.1 months (95% CI, 4.0–14.2), with 38% of patients showing intracranial progression. The progression rate was similar in both analyzed groups (58% versus 60%). For the assessment of intracranial response, only patients with measurable untreated or progressing brain lesions were included (n = 11). The overall icORR was 46% (95% CI, 17–77), with an icORR of 50% (95% CI, 12–88; one CR, two PRs) in treatment-naïve patients and 40% (95% CI, 5–85; two PRs) in pretreated patients (Figure 1(b)). The overall intracranial disease control rate (icDCR) was 91% (95% CI, 59–100) (Table 2).
Safety
The TRAEs that occurred at any grade are presented in Table 3. Overall, 61 patients (75%) experienced TRAEs, although most of them of low severity (grade ⩽ 2) (Figure 4). Peripheral edema was the most common TRAE (n = 39, 48%), followed by fatigue/asthenia (n = 16, 20%), nausea (n = 14, 17%), and creatinine increase (n = 10, 12%). Grade ⩾ 3 TREAs included peripheral edema (n = 11, 13%), creatinine increase (n = 3, 4%), liver enzymes increase (n = 3, 3%), nausea (n = 2, 2%), vomiting (n = 2, 2%), as well as dyspnea, ascites, confusion, hypoalbuminemia, and weight loss (each n = 1, 1%).
Treatment-related adverse events (TRAEs) that occurred at any grade in patients treated with capmatinib (N = 81).

Data cut-off date: November 8, 2021.
This analysis included any patient who received at least one dose of capmatinib; TRAEs were graded as per Common Terminology Criteria for Adverse Events (CTCAE) version 5.0, as determined by the treating physician. n, number of patients.
Percentage may not equal to 100 because of rounding.
In three patients, dose reduction occurred because of two simultaneously TRAEs; in two other patients, dose reduction was due to three TRAEs at once.
In two patients, treatment interruption occurred because of two simultaneously TRAEs.
Liver enzymes are related to aspartate aminotransferase (AST) and alanine aminotransferase (ALT), bilirubin, and gamma-glutamyl transferase (GGT).

Treatment-related adverse events (TRAEs). Data cut-off date: November 8, 2021; TRAEs that occurred at any grade in at least 2% of treated patients. The analysis included all patients who received at least one dose of capmatinib. Relatedness of any adverse event to the treatment was assessed by the treating physician. TRAEs were graded as per Common Terminology Criteria for Adverse Events (CTCAE, version 5.0) as determined by the treating physician. Percentage may not equal to 100 because of rounding; liver enzymes were including aspartate aminotransferase (AST), alanine aminotransferase (ALT), bilirubin, and gamma-glutamyl transferase (GGT).
For most patients (n = 59, 73%), capmatinib starting dose was 400 mg twice daily (BID), followed by 21% of them (n = 17) having received either 200 mg BID or 400 mg daily (QD) because of patient’s age, weight, or comorbidities; the latter was also the best tolerated dose in most patients (n = 34, 42%) (Table 3). Due to emergence of TRAEs, dose reduction occurred in 40% (n = 32) of patients, treatment interruption in 26% (n = 21) of them, and treatment discontinuation in 14% (n = 11). Peripheral edema led to capmatinib dose reduction in 23 patients (28%), to treatment interruption in 10 patients (12%), and to treatment discontinuation in six cases (7%). In six patients, after TRAEs resolved, capmatinib dose was then re-escalated. In case of treatment pause, the mean time of interruption was 13.8 days (range, 2–42 days).
Discussion
Because of a significant unmet medical need for the treatment of patients with advanced NSCLC harboring MET exon 14 skipping mutations, capmatinib received an accelerated approval from the U.S. Food and Drug Administration (FDA) in May 2020 based on the positive results of the GEOMETRY Mono-1 study. 25 Therefore, capmatinib was the first oral and selective MET inhibitor approved by the FDA. The Japanese Ministry of Health, Labor, and Welfare (MHLW) approved capmatinib for advanced and/or recurrent unresectable NSCLC shortly after. 26
The RECAP analysis evaluated capmatinib under real-world conditions, and, so far, represents the largest published retrospective data set on capmatinib for the treatment of MET exon 14 mutated advanced NSCLC. When comparing RECAP with outcomes from the phase II GEOMETRY Mono-1 trial 8 – a prospective, open-label multiple-cohort study including 97 NSCLC patients with a MET exon 14 skipping mutation – our data confirm the systemic and intracranial anticancer activity of capmatinib, as well as its favorable safety profile, in 81 patients, both treatment-naïve and previously treated.
As expected, the real-world RECAP patient population was less selected and therefore, patients presented with less favorable baseline conditions compared to the ones recruited in the GEOMETRY Mono-1 trial. In our population, 31% of patients had an ECOG performance status ⩾2 (versus 1%), the median age was slightly higher (77 versus 71 years), and more patients presented with brain metastases at the initiation of capmatinib (27% in both groups versus 11% in treatment-naïve and 16% in pretreated patients). Both studies included a higher proportion of women compared with men, and similar percentages of patients with adenocarcinoma, which is in line with previously published data. 13 Of note, in RECAP, a large proportion of patients had oligometastatic disease (40% with only one site of metastasis) what might have contributed to a better outcome regarding OS.
Both the ORR and DCR in our patient population were comparable with the results from the GEOMETRY Mono-1 trial. In contrast, a higher rate of previously treated patients responded in our study (50% versus 41%). 8 Overall mPFS was 9.5 months (9.1 months in pretreated cases and 10.6 months in treatment-naïve cases) in the RECAP study versus 5.4 or 12.4 months in the GEOMETRY Mono-1 trial. 8
In the RECAP population, an encouraging intracranial activity of capmatinib was observed. In patients with measurable brain lesions according to protocol, the icORR reached 46% (including 18% with a CR) and a icDCR of 91%. In addition, mPFS in patients with intracranial disease was similar to overall population in RECAP. These results are comparable with the results of the phase II trial with an icORR of 54% and a icDCR of 92%.
No new safety signals were reported in the RECAP study. Capmatinib showed a manageable safety profile and low discontinuation rates, with mainly low-grade and reversible TRAEs. However, dose reductions and treatment interruptions were frequently necessary emphasizing the importance of regular monitoring of patients during capmatinib therapy. TRAEs grade 3/4 were reported in 23% of patients in the RECAP cohort, compared to 53% of patients with MET exon 14 skipping mutation in the GEOMETRY Mono-1 trial. This difference mostly can be explained by differential recall bias, given the retrospective nature of the RECAP study on one side, and the prospective reporting in the GEOMETRY Mono-1 trial on the other side. The most common TRAE are peripheral edema in both analyzed populations.
When analyzing the prior therapies administered to patients in RECAP, capmatinib achieved a higher response rate than chemotherapy or immunotherapy, either as monotherapy or combined. This finding must be interpreted with caution due to the small sample size. In RECAP, 40% of patients had a high PD-L1 expression (TPS ⩾ 50%); which is in line with previous published report. 27 However, in MET exon 14 mutated NSCLC, prior publications indicated a response rate to PD-1 inhibition of only 16–36%; biomarkers of immunotherapy efficacy are not well defined so far.18,28
Additionally, TP53 has been described as the most common co-mutation to a MET exon 14 skipping genomic alteration, with an incidence of 22% in non-squamous patients who never smoked. 29 In our mixed population containing 43% of never-smokers, the TP53 mutation was the most frequent co-mutation found in seven patients (9%). In MET exon 14-mutated patients, no correlation between co-mutations with TP53 and efficacy of therapy were identified up to now, 29 though this aspect remains unclear, given the small number of patients in this analysis.
The challenge for pathologists is to timely identify MET exon 14 skipping mutations, to enable patients to benefit from this targeted therapy. According to the international ESMO guidelines, NGS is the recommended testing method for detecting rare genomic alterations, such as MET exon 14 skipping mutation, in metastatic cancer cases. 30
This retrospective analysis carries several inevitable limitations, such as selection bias, reporting bias, and information bias. Moreover, given the small sample size of some subgroups, only descriptive efficacy outcomes have been presented. Additionally, inherent limitations to clinical routine practice in each participating center – especially in terms of MET testing methods, intervals of radiographic assessments, and national- or hospital-based treatment guidelines – should be considered. With those limitations in mind, our real-world results were however in line with previously reported phase II clinical data. 8
In the case of rare disease, data from patients treated in real-world settings are essential to assess treatment efficacy and safety in non-selected patient populations presenting with comorbidities and poor performance status. To date, several trials are testing selective MET inhibitors – as monotherapy or in combinations – in NSCLC.11,31 Anticipating the emergence of acquired resistance against current MET inhibitors, co-alterations that might be involved in treatment escape mechanisms have been already identified32,33; however, the frequency and the type of resistance may change with broader use of more potent and specific MET-TKIs or MET molecular antibodies. 11
Supplemental Material
sj-docx-1-tam-10.1177_17588359221103206 – Supplemental material for Real-world experience with capmatinib in MET exon 14-mutated non-small cell lung cancer (RECAP): a retrospective analysis from an early access program
Supplemental material, sj-docx-1-tam-10.1177_17588359221103206 for Real-world experience with capmatinib in MET exon 14-mutated non-small cell lung cancer (RECAP): a retrospective analysis from an early access program by Oliver Illini, Hannah Fabikan, Aurélie Swalduz, Anders Vikström, Dagmar Krenbek, Michael Schumacher, Elizabeth Dudnik, Michael Studnicka, Ronny Öhman, Robert Wurm, Luciano Wannesson, Nir Peled, Waleed Kian, Jair Bar, Sameh Daher, Alfredo Addeo, Ofer Rotem, Georg Pall, Alona Zer, Akram Saad, Tanja Cufer, Hadas Gantz Sorotsky, Sayed M. S. Hashemi, Katja Mohorcic, Ronen Stoff, Yulia Rovitsky, Shoshana Keren-Rosenberg, Thomas Winder, Christoph Weinlinger, Arschang Valipour and Maximilian J. Hochmair in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Medical writing assistance was provided by Dr. Florence Boulmé.
Author contribution(s)
Compliance with ethical standards
The study protocol was approved by the ethics committee of the city of Vienna, Austria (EK-21-239-1121). According to Austrian laws, informed consent for each patient was not necessary for this retrospective analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This academic collaboration was supported by the Karl Landsteiner Institute for Lung Research and Pulmonary Oncology.
Conflict of interest statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.