
Abstract
Background:
A reliable model is needed to estimate the risk of postoperative recurrence and the benefits of postoperative radiotherapy (PORT) in patients with thoracic esophageal squamous cell cancer (TESCC).
Methods:
The study retrospectively reviewed 3652 TESCC patients in stage IB-IVA after radical esophagectomy, with or without PORT. In one institution as the training cohort (n = 1620), independent risk factors associated with locoregional recurrence (LRR), identified by the competing-risks regression, were used to establish a predicting nomogram, which was validated in an external cohort (n = 1048). Area under curve (AUC) values of receiver operating characteristic curves were calculated to evaluate discrimination. Risk stratification was conducted using a decision tree analysis based on the cumulative point score of the LRR nomogram. After balancing the baseline of characteristics between treatment groups by inverse probability of treatment weighting, the effect of PORT was evaluated in each risk group.
Results:
Sex, age, tumor location, tumor grade, and N category were identified as independent risk factors for LRR and added into the nomogram. The AUC values were 0.638 and 0.706 in the training and validation cohorts, respectively. Three risk groups were established. For patients in the intermediate- and high-risk groups, PORT significantly improved the 5-year overall survival by 10.2% and 9.4%, respectively (p < 0.05). Although PORT was significantly associated with reduced LRR in the low-risk group, overall survival was not improved.
Conclusion:
The nomogram can effectively estimate the individual risk of LRR, and patients in the intermediate- and high-risk groups are highly recommended to undergo PORT.
Introduction
Although the CROSS and NEOCRTEC5010 trials demonstrated that patients with locally advanced esophageal cancer could benefit from neoadjuvant chemoradiation,1,2 nevertheless it is still the case that more than 50% of patients still underwent surgical excision as their first treatment.3,4 Regardless of pathological T and N categories, 2020 National Comprehensive Cancer Network (NCCN) guidelines for thoracic esophageal squamous cell cancer (TESCC) do not recommend adjuvant treatment for patients with clear margins after esophagectomy. 5 However, evidence indicates that the locoregional recurrence (LRR) rate is as high as 39.5%–52.4%.6–10 Moreover, the efficacy of salvage therapy after recurrence is poor, with a median survival time of only 3–8 months.11–13 Thus, limitations with surgery result in the need for multidisciplinary adjuvant therapy.
Estimating recurrence patterns after surgery is a prerequisite for adjuvant therapy decisions. Since postoperative recurrence is affected by a variety of biological and clinical factors,14,15 radiation oncologists need to identify a candidate subset who may obtain survival benefit from prophylactic postoperative radiotherapy (PORT). Nomograms serve as statistical tools to integrate clinicopathological variables and generate individual risk predictions, and data suggest that nomograms can achieve precise prediction for both LRR and distant metastasis (DM) in esophageal cancer and also in other cancer types.16–18 Therefore, stratifying patients into different categories based on individual LRR risk to assist decision-making in the aspect of PORT is promising.
Since the rarity of thoracic esophageal adenocarcinoma in Asia and its distinct biological characteristics, only squamous cell carcinoma was analyzed. Our study aimed to build a risk stratification based on the nomogram estimating individual LRR after radical surgery and further identify a patient subset who might benefit from PORT.
Materials and methods
Patient selection
This two-center retrospective study collected 3811 TESCC patients who underwent esophagectomy from two independent medical institutions, including 2281 patients treated from January 2004 to December 2012 in the Cancer Hospital, Chinese Academy of Medical Sciences, and 1530 patients treated from February 1993 to March 2007 in the Fujian Provincial Cancer Hospital. All patients had histologically proven TESCC after radical resection with no neoadjuvant anticancer therapy. Patients with stage I TESCC who underwent PORT, those who had lymph node metastasis above the sternal notch (M1 disease according to the American Joint Committee on Cancer system), those who received a radiation dose greater than 60 Gy, or those who had a follow-up period of less than 3 months after surgery were excluded from the study. All patients provided written informed consent, and the study was approved by the Ethics Committee of the Cancer Hospital, Chinese Academy of Medical Sciences (ID:14-090/880) and Fujian Province Cancer Hospital (ID: K201427).
Surgery
Prior to the surgery, the clinical staging was evaluated with the physical examination; endoscopic ultrasound; computed tomography (CT) scan of the neck, chest, and abdomen; ultrasound of cervical and supraclavicular region; and radionuclide bone scan. Positron emission tomography (PET)-CT in clinical staging in this study was not used routinely. Details of the operation are described previously.19,20 Briefly, Mckeown esophagectomy with three-field lymphadenectomy was performed in the Fujian Provincial Cancer Hospital, and Ivor Lewis and left transthoracic esophagectomy with two-field lymphadenectomy were the most common surgical approach performed in the Cancer Hospital Chinese Academy of Medical Sciences.
Radiotherapy
Determined by a multidisciplinary team and patients’ preference, adjuvant therapy options included radiotherapy, concurrent chemoradiation, or chemotherapy initiated 4–6 weeks after surgery. In the Cancer Hospital Chinese Academy of Medical Sciences, the clinical target volume (CTV) was determined by the primary tumor and the high-risk lymphatic drainage areas. For upper thoracic lesions despite nodal status, the CTV borders were defined superiorly as the upper margin of the T1 vertebral body and inferiorly as 2 to 3 cm below the trachea carina; for middle and lower thoracic lesions without lymph node involvement or middle thoracic lesions with lymph node metastasis which was confined to the mediastinum, the CTV borders were defined superiorly as the cricothyroid membrane and inferiorly as 2 to 3 cm below the lower border of the tumor bed; for middle thoracic lesions with lymph node metastasis which was extended to the upper abdomen and lower thoracic lesions with lymph node involvement, the CTV borders were defined superiorly as the cricothyroid membrane and inferiorly as the origin of the celiac artery. In the Fujian Provincial Cancer Hospital, for patients treated after 1996, a modified T-shaped field was performed with the superior border at C6 vertebral body and inferior border below the lower border of the tumor bed; previous patients were treated with a large T-shaped field, including bilateral supraclavicular fossa, mediastinum, left gastric nodes, and the tumor bed. 21 Radiation was delivered by conventional, three-dimensional conformal or intensity-modulated radiotherapy with the prescription of 50–60 Gy in 1.8–2.0 Gy fractions. The chemotherapy regimen typically included platinum, taxane, and fluorouracil.
Surveillance and recurrence
All patients were followed up every 3 months for the first 2 years, every 6 months in years 3 and 4, and annually after that. Follow-up evaluation consisted of clinical examination, blood tests, and neck/chest/abdominal computed tomography and barium swallow, and pathological biopsy was attempted once suspicious recurrence was reported.
LRR was defined as recurrence at the anastomosis, tumor bed, and lymphatic drainage of supraclavicular, mediastinal, left gastric, or celiac trunk regions. In contrast, DM was defined as nonregional lymph node recurrence or systemic metastases. Localization and the date of identification of the first recurrences were recorded, and multiple recurrences detected within 1 month were considered synchronous.
Statistical analysis
A chi-square test was used to compare categorical data. Overall survival (OS) was estimated using the K–M analysis with the log-rank test. Independent risk factors associated with LRR and DM were identified using multivariate analysis based on competing-risks regression for patients who underwent surgery alone. Death before estimating recurrence was defined as a competing risk. Patients from the Cancer Hospital, Chinese Academy of Medical Sciences were defined as the training cohort, and those from the Fujian Provincial Cancer Hospital were defined as the validating cohort.
Next, a predictive nomogram was developed based on independent risk factors associated with LRR, and then the external validation was performed. The area under the curve (AUC) values of the time-dependent receiver operating characteristic (ROC) curve was used to calculate the predictive power of the nomogram; calibration was conducted by comparing the decile of predicted probabilities and actual probabilities.
Finally, a decision tree analysis was conducted to determine two optimal cutoff points based on the LRR nomogram scores; and the overall patients were further stratified into low-, intermediate-, and high-risk groups. Then, cumulative incidence analysis was used to describe the LRR and DM rates, of which the difference between the S (defined as the patients who received surgery alone) and PORT groups (defined as the patients who received surgery followed by radiotherapy) was compared with Fine and Gray’s test. Stabilized inverse probability of treatment weighting (sIPTW) was conducted to reduce selection bias by balancing the baseline of characteristics between the S and PORT groups. 22 All tests were two-sided, and the criterion for significance was p < 0.05. All statistical analyses were conducted using SPSS (version 23.0; Chicago, IL, USA) and R (version 3.4.3; R Foundation for Statistical Computing, Vienna, Austria) software.
Results
A total of 3652 patients were included in the analysis, with 2668 patients in the S group and 984 patients in the PORT group. The baseline characteristics of the overall cohort are summarized in Table 1. The median age of the entire patient was 58 years (range, 28–83 years) and the median length of primary length was 5.0 cm (range, 1.0–20.0 cm). More than 60% of lesions in this analysis were located in the middle esophagus. Most lesions invaded outside the esophageal wall (T3–4a), with more than 50% of lesions having node-positive diseases. Since pT1N0M0 patients for whom PORT was not performed as a standard treatment were excluded, all pT1 patients in this study only underwent surgery. Nearly 30% of patients underwent adjuvant therapy. Younger patients and those with a longer lesion length, higher histologic grade, or a more advanced pathological stage were more likely to undergo PORT.
Baseline characteristics of the S and PORT groups.

AJCC, American Joint Committee on Cancer; LVSI, lymph vascular space invasion; PORT, postoperative radiotherapy; S, surgery.
The baseline characteristics of patients in the S group are summarized in Supplemental Table 1. The median follow-up period was 61.5 months [95% confidence interval (CI) 59.7–63.3], with 1-, 3-, and 5-year OS rates of 88.1%, 60.7%, and 50.6%, respectively. Death from any cause occurred in 1297 patients. The median follow-up period was 62.0 months (95% CI 60.1–63.9) in the training cohort and 59.7 months (95% CI 55.6–63.8) in the validation cohort. The 1-, 3-, and 5-year OS rates in the training cohort were 87.2%, 57.0%, and 47.5%, and in the validation cohort were 89.3%, 66.8%, and 55.7%, respectively. Recurrence occurred in 922 patients in the training cohort and 473 patients in the validation cohort. In the training cohort, the median time to overall recurrence, LRR, and DM was 11.1 months, 11.0 months, and 11.5 months, respectively, and 11.8 months, 12.2 months, and 11.0 months, respectively, in the validation cohort.
Competing-risks nomogram development and external validation
In the training cohort, multivariate analysis identified male sex, age younger than 60 years, upper and middle esophageal tumor, high tumor grade, and advanced N categories as independent risk factors for a high LRR rate. Furthermore, male sex, high tumor grade, and advanced N categories were independent predictors of DM rate (Table 2). The competing-risks nomogram for LRR is illustrated in Figure 1. The risk score was the sum of points assigned by independent risk factors, and 1-, 2-, and 3-year LRR probabilities were predicted according to the lowest scale. The 3-year AUC values of time-dependent ROC curves were 0.638 in the training cohort and 0.706 in the validation cohort, respectively (Figure 2(a) and (b)). The calibration plot for the probability of 3-year LRR was consistent between the predictive and actual survival rates (Figure 2(c) and (d)).

Nomogram for locoregional recurrence developed from the training cohort.
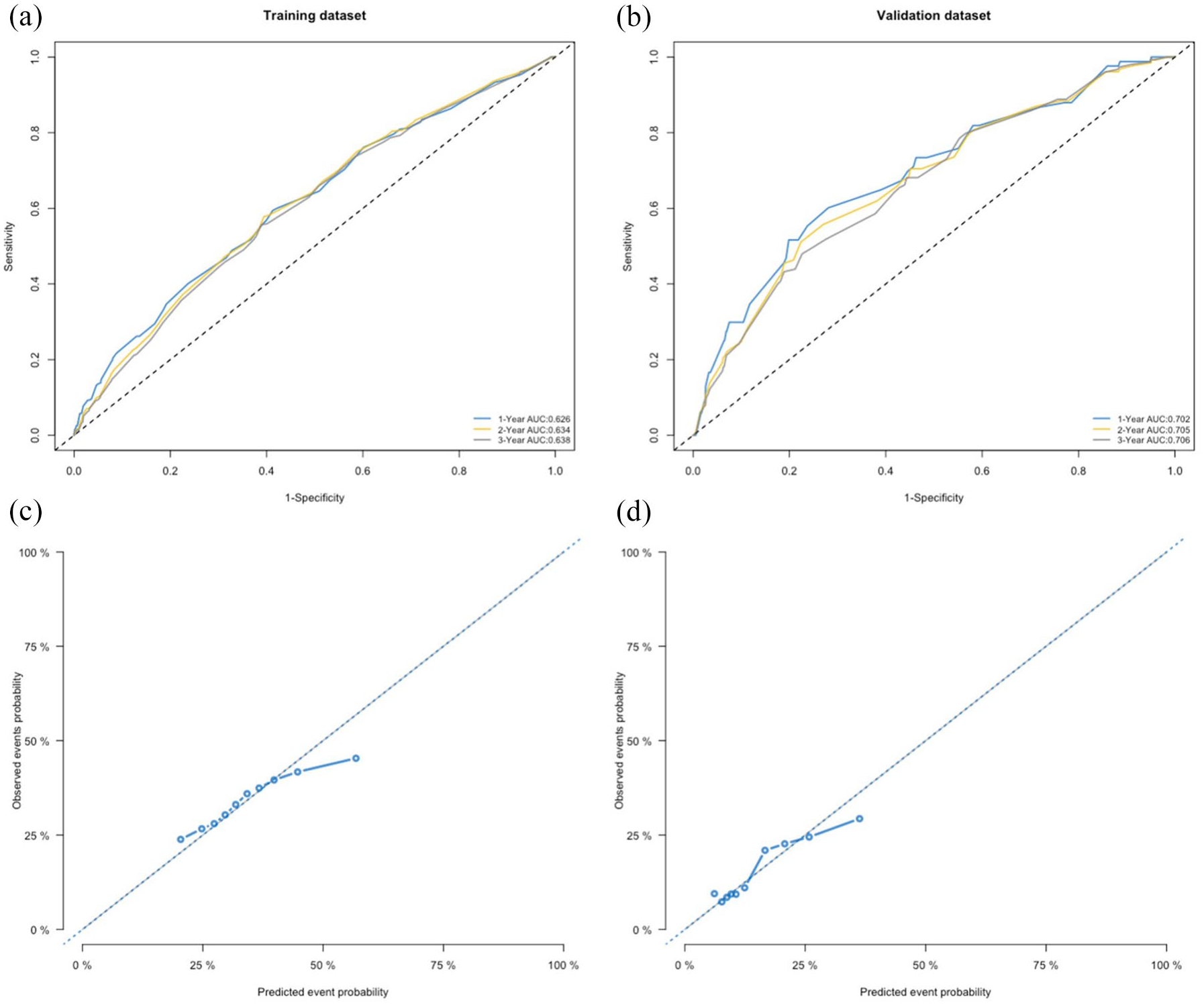
(a) Receiver operating characteristic (ROC) curves for 1-, 2-, and 3-year locoregional recurrence (LRR) according to the nomogram in the training cohort. The area under the curve (AUC): blue line (1-year), yellow line (2-year), gray line (3-year). (b) ROC curves for 1-, 2-, and 3-year LRR rates according to the nomogram in the validation cohort. AUC: blue line (1-year), yellow line (2-year), gray line (3-year). (c) Calibration plot for 3-year LRR prediction according to the nomogram in the training cohort. (d) Calibration plot for 3-year LRR prediction according to the nomogram in the validation cohort.
Multivariate competing-risks analysis of locoregional recurrence and distant metastasis in unirradiated patients in the training cohort.

CI, confidence interval; LVSI, lymph vascular space invasion.
Locoregional recurrence stratification
The decision tree analysis identified two cutoff points (scores of 79 and 135.5), and 3 risk categories were developed (Figure 3(a)). Patients with a risk score of ⩽79 were assigned to the low-risk group (1065 of 3652, 29.2%) and those with a risk score of > 79 to ⩽135.5 were assigned to the intermediate-risk group (1936 of 3652, 53.0%), with the remaining patients assigned to the high-risk group (651 of 3652, 17.8%) with a risk score of > 135.5. The baseline characteristics of the different groups are summarized in Supplemental Table 2. For patients receiving surgery alone, the OS, LRR, and DM rates in each group were significantly distinct from each other (Figure 3(b)–(d)).

(a) Decision tree analysis according to the effect of nomogram score on locoregional recurrence (LRR) in unirradiated patients. (b) Cumulative incidence of LRR rate and distant metastasis (DM) rate. (c) Cumulative incidence of DM. (d) Cumulative incidence of mortality.
Cumulative incidence analysis in each risk group
In the low-risk group, the median time to recurrence was 13.9 months in the S group and 13.2 months in the PORT group. The 3-year LRR rate was significantly lower in the S group than that in the PORT group, but the 3-year DM rate and 5-year OS rate were similar between the two treatment groups (Figure 4(a)–(c)). The baseline characteristics before and after sIPTW in each risk group were summarized in Supplemental Table 3. After sIPTW, the 5-year OS rates were comparable between treatment groups (S group: 66.8%; PORT group: 71.9%; p = 0.461) (Supplementary Figure 1A).

Cumulative incidence of locoregional recurrence (LRR) rate, distant metastasis (DM) rate, and overall survival (OS) in the low-risk group (a–c), intermediate-risk group (d–f), and high-risk group (g–i), respectively. S: surgery; PORT: postoperative radiation therapy.
In the intermediate-risk group, the median time to recurrence was 12.0 months in the S group and 16.7 months in the PORT group. Patients in the PORT group were significantly associated with a lower 3-year LRR rate and a higher 3-year DM rate compared with those in the S group, whereas the 5-year OS was similar between the two treatment groups (Figure 4(d)–(f)). However, the baseline characteristics were unbalanced, and a more advanced N stage was observed in the PORT group compared with the S group. After sIPTW, PORT reversely correlated with an improved 5-year OS rates (S group: 45.2%; PORT group: 55.4%; p < 0.001) (Supplementary Figure 1B).
In the high-risk group, the median time to recurrence was 6.9 months in the S group and 11.7 months in the PORT group. A lower 3-year LRR rate, a higher 3-year DM rate, and an improved 5-year OS rate were observed in the PORT group compared with the S group (Figure 4(g)–(i)). After sIPTW, PORT still significantly correlated with an improved 5-year OS rate (S group: 19.6%; PORT group: 29.0%; p < 0.001) (Supplementary Figure 1 C).
Toxicity
Toxicities were evaluated according to the Common Terminology Criteria for Adverse Events v3.0 and Radiation Therapy Oncology Group. The rates of radiotherapy-related early adverse reactions were 39.0% (n = 384) for radiation esophagitis (grade 3/4, n = 16) and 6.5% (n = 64) for upper digestive tract, respectively. The rates of grade 3/4 hematology were 6.7% (n = 66) in the PORT group, and 4.6% (3/65) patients in the S group (only for those who received surgery plus adjuvant chemotherapy). Besides, the frequency of anastomotic stenosis was 15 and 7 patients in the PORT and S groups, respectively. A total of five patients in the S group died of gastric bleeding during follow-up compared with eight patients in the PORT group, but it was not clear whether the death was related to radiotherapy.
Discussion
It is necessary to identify patients at a high risk of LRR after surgery without receiving neoadjuvant therapy and estimate whether these patients could benefit from PORT. Accordingly, the current study developed a competing-risks nomogram to evaluate an individual risk of LRR in TESCC patients after radical esophagectomy. The nomogram showed good prognostic efficacy and high generalizability when validated in an external cohort. Patients were stratified into three risk categories using a decision tree analysis, and those in the intermediate- and high-risk groups could obtain survival benefits from PORT.
Several reports have investigated the risk factors associated with postoperative recurrence in patients with esophageal cancer. Peyre et al. 14 reported that node status, depth of invasion, and the number of involved lymph nodes as significant determinants of system disease. Other studies10,23–26 reported the risk of tumor recurrence was mainly associated with surgical approaches, age, dysphagia, tumor length, histologic grade, and so on. Similarly, our study identified five risk factors associated with LRR and DM, including sex, age, histologic grade, tumor location, and N-stage. Besides with N-stage, five clinicopathologic factors were added in the LRR nomogram, which demonstrated good prognostic discrimination and a high reproducibility when externally validated with AUC values ranging from 0.638 to 0.706, as demonstrated by some investigators’ reports that the C-index of nomograms in predicting recurrence ranged from 0.62 to 0.69.27–29 However, few clinical studies have reported a C-index exceeding 0.75, which might indicate that recurrence prediction is complex and can be affected by other unknown factors. In the study reported by Gregory et al., 30 tumor genomics was an effective supplement for clinicopathologic factors to predict recurrence pattern after surgery of early-stage lung adenocarcinoma. Thus, more laboratory studies to identify tumor genomic factors associated with recurrence in esophageal cancer may be warranted.
Based on individual risk quantification of LRR, all TESCC patients were classified into three risk categories, which had significant implications for the decision-making of PORT. In the low-risk group, the main component of this cohort was patients in the pN0–1 stage, with the lowest LRR rate (19.2%) and the highest OS rate (67.6%). We found that PORT correlated with a reduced LRR rate without significant influence on OS, which is consistent with the prospective study reported by Deng et al. 31 Therefore, these data indicated that intensive PORT may be of less value for patients in the low-risk group. For patients in the intermediate-risk group, the median time to recurrence was 12.0 months and approximately 30% of patients developed LRR. Given the unbalanced baseline characteristics between the two groups, the cumulative incidence analysis showed that PORT is significantly associated with a reduced LRR rate but not with improved OS. After sIPTW, 5-year OS was significantly higher in the PORT group compared with the S group (45.2% versus 55.4%, respectively; p < 0.001). However, caution should still be exercised when drawing conclusions because of the considerable heterogeneity of patients within this group, but we still highly recommended PORT for patients in the intermediate-risk group. For patients in the high-risk group, the LRR rate was remarkably high (39.8%) and half of the recurrence occurred within 7 months. Compared with surgery alone, there was an evident reduction of risk in LRR and a significant improvement on OS in favor of PORT, which was still consistent with the result after balancing the baseline characteristics, suggesting PORT for patients in the high-risk group may be warranted. Similar findings were reported in previous studies,32–35 specifically, PORT correlated with a better prognosis in more locally advanced esophageal cancer patients.
The rationale for combined system therapy in TESCC is the high prevalence of DM after surgery. In this context, we found the rates of DM were relatively high in the intermediate- and high-risk groups (15.2% and 23.7%, respectively). Similarly, Mariette et al. 9 reported that 19.8% of patients developed DM after curative esophagectomy for thoracic esophageal cancer. Furthermore, given that a proportion of patients survived longer after PORT due to a reduction in LRR and a prolonged regular recurrence time, DM occurred more frequently and became the main reason for failure in the PORT group. The value of postoperative chemoradiation therapy in treating resectable TESCC remains uncertain, but a recent meta-analysis of 2165 patients demonstrated that postoperative chemoradiation is associated with significantly improved OS and significantly reduced LRR rate compared with non-chemoradiation postoperative treatments (chemotherapy alone, radiotherapy alone, or observation). 36 The integration of chemotherapy, radiotherapy, and immunotherapy is a way to go of esophageal cancer therapy. These treatment approaches might only bring survival benefits at certain stages of treatment. Hence, clinicians needed to pay more attention to the risk-stratified studies, as the CheckMate 577 37 trial reported nivolumab was associated with significant improvement in disease-free survival after neoadjuvant chemoradiotherapy and surgery in patients with resected esophageal or gastroesophageal junction cancer who did not achieve the pathological complete response.
The major limitation of this study is selection bias due to the nature of the retrospective analysis. Our study comprised a small number of cases using minimally invasive esophagectomy, which has become more prevalent in recent years. However, a meta-analysis reported no statistically significant differences in long-term oncological outcomes between the minimally invasive esophagectomy and open esophagectomy. 38 Therefore, our results could still assist clinical decision-making. In addition, the LRR nomogram was limited to the patients who received surgery alone but not to patients who received neoadjuvant treatment. Nevertheless, our study also has several strengths: it involved a large cohort of TESCC patients with long-term follow-up; it used an independent cohort as the external validation; it is unique in its stratification of recurrence risk groups based on the cumulative score of the nomogram. However, this approach for selected potential beneficiaries of PORT needed to be validated in a prospective trial.
In conclusion, a competing-risks nomogram could effectively quantify the individualized risk of LRR by integrating independent risk factors, and patient stratification by decision tree analysis showed good discrimination between recurrence patterns. This newly defined intermediate- and high-risk patient subgroup is highly recommended to undergo PORT for survival benefits. This study provides clinical guidance for adjuvant radiotherapy for TESCC patients after surgery and lays a preliminary foundation for designing a prospective stratified trial.
Supplemental Material
sj-docx-1-tam-10.1177_17588359211061948 – Supplemental material for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy
Supplemental material, sj-docx-1-tam-10.1177_17588359211061948 for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy by Xiao Chang, Junqiang Chen, Wencheng Zhang, Jinsong Yang, Shufei Yu, Wei Deng, Wenjie Ni, Zongmei Zhou, Dongfu Chen, Qinfu Feng, Jima Lv, Jun Liang, Zhouguang Hui, Lvhua Wang, Yu Lin, Xiaohui Chen, Qi Xue, Yousheng Mao, Yushun Gao, Dali Wang, Feiyue Feng, Shugeng Gao, Jie He and Zefen Xiao in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359211061948 – Supplemental material for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy
Supplemental material, sj-docx-2-tam-10.1177_17588359211061948 for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy by Xiao Chang, Junqiang Chen, Wencheng Zhang, Jinsong Yang, Shufei Yu, Wei Deng, Wenjie Ni, Zongmei Zhou, Dongfu Chen, Qinfu Feng, Jima Lv, Jun Liang, Zhouguang Hui, Lvhua Wang, Yu Lin, Xiaohui Chen, Qi Xue, Yousheng Mao, Yushun Gao, Dali Wang, Feiyue Feng, Shugeng Gao, Jie He and Zefen Xiao in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359211061948 – Supplemental material for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy
Supplemental material, sj-docx-3-tam-10.1177_17588359211061948 for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy by Xiao Chang, Junqiang Chen, Wencheng Zhang, Jinsong Yang, Shufei Yu, Wei Deng, Wenjie Ni, Zongmei Zhou, Dongfu Chen, Qinfu Feng, Jima Lv, Jun Liang, Zhouguang Hui, Lvhua Wang, Yu Lin, Xiaohui Chen, Qi Xue, Yousheng Mao, Yushun Gao, Dali Wang, Feiyue Feng, Shugeng Gao, Jie He and Zefen Xiao in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-4-tam-10.1177_17588359211061948 – Supplemental material for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy
Supplemental material, sj-docx-4-tam-10.1177_17588359211061948 for Recurrence risk stratification based on a competing-risks nomogram to identify patients with esophageal cancer who may benefit from postoperative radiotherapy by Xiao Chang, Junqiang Chen, Wencheng Zhang, Jinsong Yang, Shufei Yu, Wei Deng, Wenjie Ni, Zongmei Zhou, Dongfu Chen, Qinfu Feng, Jima Lv, Jun Liang, Zhouguang Hui, Lvhua Wang, Yu Lin, Xiaohui Chen, Qi Xue, Yousheng Mao, Yushun Gao, Dali Wang, Feiyue Feng, Shugeng Gao, Jie He and Zefen Xiao in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We appreciate the financial support by the Beijing Hope Run Special Fund of Cancer Foundation of China (LC2016L04).
Author contributions
ZX and JH participated in the study conception and design, data analysis, reviewed the paper and approved the final draft for submission; XC and J.C participated in statistical analyses and drafted the manuscript; WZ, JY, SY, WD, and WN participated in methodology, investigation, reviewed the paper, and approved the final draft for submission. ZZ, DC, QF, JL, JL, ZH, LW, and YL participated in investigation, reviewed the paper, and approved the final draft for submission. XC, QX, YM, YG, DW, FF, and SG participated in conceptualization, reviewed the paper, and approved the final draft for submission.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Beijing Hope Run Special Fund of Cancer Foundation of China (LC2016L04).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.