
Abstract
Background:
Metastatic pancreatic ductal adenocarcinoma (mPDAC) bears a dismal prognosis due to the limited activity of systemic chemotherapy. In our platform for precision medicine, we aim to offer molecular-guided treatments to patients without further standard therapy options.
Methods:
In this single center, real-world retrospective analysis of our platform, we describe the molecular-based therapy approaches used in all 50 patients diagnosed with therapy-refractory mPDAC. A molecular portrait of the tumor specimens was created by next-generation sequencing, immunohistochemistry (IHC), microsatellite instability (MSI) testing, and fluorescence in situ hybridization.
Results:
In total, we detected 123 mutations in 50 patients. The five most frequent mutations were KRAS (n = 40; 80%), TP53 (n = 29; 58%), CDKN2A (n = 8; 16%), SMAD4 (n = 4; 8%), and NOTCH1 (n = 4; 8%), which together accounted for 40.2% of all mutations. Two patients had gene fusions, namely, TBL1XR1–PIK3CA and EIF3E–RSPO2. IHC detected expression of EGFR, phosphorylated mTOR, and PTEN in 36 (72%), 33 (66%), and 17 patients (34%), respectively. For 14 (28%) of the 50 patients, a targeted therapy was suggested based on the identified molecular targets. The recommended treatments included the mTOR inhibitor everolimus (n = 3), pembrolizumab (n = 3), palbociclib (n = 2), nintedanib (n = 2), and cetuximab, crizotinib, tamoxifen, and the combination of lapatinib and trastuzumab, in one patient each.
Finally, five patients received the recommended therapy. Four patients died due to disease progression before radiological assessment. One patient was treated with nintedanib and achieved stable disease for 6 months.
Conclusion:
Based on our observations, precision medicine approaches are feasible and implementable in clinical routine and may provide molecular-based therapy recommendations for mPDAC.
Keywords
Introduction
The most common subtype of pancreatic cancer is pancreatic ductal adenocarcinoma (PDAC), which stems from the epithelial cells of the pancreatic ducts. PDAC is an aggressive, lethal disease, with a dismal prognosis of approximately 5–9% 5-year overall survival. 1 Pancreatic cancer is the 7th-leading cause of cancer-related death in the world, although it is only the 11th most common cancer globally, accounting for only 4% of all cancers. 2 Pancreatic cancer is a malignancy of the elderly population, as the incidence of pancreatic cancer increases with age; the highest incidence rates are observed in patients over 70 years old. The incidence is slightly more common in men, with 5.5 per 100,000, than in women, with 4.0 per 100,000. 2 More than 450,000 people worldwide were diagnosed with pancreatic cancer in 2018, and more than 430,000 patients died of this disease in the same year. Thus, incidence roughly corresponds to mortality. Globally, the incidence of pancreatic cancer in both sexes has more than doubled (2.3 times) from 195,000 new cases in 1990 to 448,000 incident cases in 2017. 3 According to GLOBOCAN 2018, it is expected that the newly diagnosed cases of pancreatic cancer will rise to 800,000 by 2040. 2
At the localized stage, the only curative option is complete surgical resection; however, less than 20% of all patients are at a locally advanced stage at the time of initial diagnosis, and thus most are ineligible for surgery. Pancreatic cancer metastasizes at an early stage and causes unspecific symptoms. When the disease spreads, surgery is not feasible and systemic palliative chemotherapy is the cornerstone of the management of metastatic PDAC. On the front line, patients are either treated with FOLFIRINOX (folinic acid, fluorouracil, irinotecan, and oxaliplatin) or gemcitabine combined with nab-paclitaxel. In the case of tumor therapy resistance to gemcitabine and nab-paclitaxel, patients can be given nanoliposomal irinotecan (nal-IRI) and 5-fluorouracil/leucovorin (5-FU/LV) in the second line, according to the landmark phase III NAPOLI-1 trial. 4 However, after failure of the standard treatments, therapeutic options are very limited, and evidence-based data for management of therapy-refractory patients are scarce. Due to the strong immunosuppressive milieu exerted by pancreatic cancer cells, and the poor drug delivery and performance because of the dense desmoplastic and hypoxic tumor microenvironment, most drugs fail to exhibit antitumoral activity in PDAC. 5
In recent years, efforts have been made to personalize therapy regimens in specific cancers. In a few particular cancers, treatment with tyrosine kinase inhibitors, or immunotherapeutic agents tailored to the individual, have been possible, for example, trastuzumab in HER2-positive breast or gastric cancer or sunitinib in advanced renal cell carcinoma (RCC).6,7
By the application of several methods and techniques, including next-generation sequencing and immunohistochemistry, it is possible to create a molecular portrait of a tumor. Based on the molecular profile, potential druggable molecular targets can be identified that can be targeted by molecular-guided anticancer agents. This approach is known as precision medicine, and its goal is to yield deep and sustained responses by targeting specific molecular targets, and, at the same time, sparing healthy cells.
We conducted a retrospective subgroup analysis of all 50 patients with therapy-refractory metastatic PDAC (mPDAC) that had been enrolled on and profiled via our platform for precision medicine at the Medical University of Vienna. We mapped the molecular profiles of the mPDAC patients and sought to specifically target the detected molecular alterations.
Methods
Patients and design of the precision medicine platform
Patients with pretreated, advanced mPDAC, who were refractory to all standard treatment options, were eligible for enrolment in our platform for precision medicine – provided archival tissue samples were available. Patients had to have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Our platform for precision medicine is not a clinical trial; however, it aims to offer the possibility of a targeted therapy to all patients where no standard antitumoral treatment is available. Informed consent was obtained from all patients before inclusion in our platform. Furthermore, the Institutional Ethics Committee of the Medical University of Vienna also approved this analysis (Nr. 1039/2017). The General Hospital of Vienna directly covered all costs for molecular profiling, provided the cancer patients had no further standard treatment options.
Tissue samples
Formalin-fixed, paraffin-embedded tissue samples from patients with advanced mPDAC who had progressed to all standard therapy regimens were obtained from the archive of the Department of Pathology, Medical University Vienna, Vienna, Austria.
Cancer gene panel sequencing
DNA was extracted from paraffin-embedded tissue blocks with a QIAamp Tissue KitTM (Qiagen, Hilden, Germany), and 10 ng DNA per tissue sample was provided for sequencing. The DNA library was created by multiplex polymerase chain reaction (PCR) with the Ion AmpliSeq Cancer Hotspot Panel v2 (Thermo Fisher Scientific, Waltham, MA, USA), which covers mutation hotspots of 50 genes. The panel includes driver mutations, oncogenes, and tumor suppressor genes. By mid-2018, the gene panel was expanded using the 161-gene next-generation sequencing panel of Oncomine Comprehensive Assay v3 (Thermo Fisher Scientific), which covers genetic alterations and gene fusions (see supplemental information for complete list of the gene panel). The Ampliseq cancer hotspot panel was sequenced with an Ion PGM (Thermo Fisher Scientific) and the Oncomine Comprehensive Assay v3 on an Ion S5 sequencer (Thermo Fisher Scientific). The description of each mutation was presented according to the Human Genome Variation Society (HGVS). 8
Immunohistochemistry
Immunohistochemistry (IHC) was performed using 2-μm-thick tissue sections read by a Ventana Benchmark Ultra stainer (Ventana Medical Systems, Tucson, AZ, USA). The following antibodies were applied: anaplastic lymphoma kinase (ALK) (clone 1A4; Zytomed, Berlin, Germany), CD20 (clone L26; Dako), CD30 (clone BerH2; Agilent Technologies, Vienna, Austria), DNA mismatch repair (MMR) proteins that included MLH1 (clone M1; Ventana Medical Systems), PMS2 (clone EPR3947; Cell Marque, Rocklin, CA, USA), MSH2 (clone G219-1129; Cell Marque), and MSH6 (clone 44; Cell Marque), epidermal growth factor receptor (EGFR) (clone 3C6; Ventana), estrogen receptor (clone SP1; Ventana Medical Systems), human epidermal growth factor receptor 2 (HER2) (clone 4B5; Ventana Medical Systems), HER3 (clone SP71; Abcam, Cambridge, UK), C-kit receptor (KIT) (clone 9.7; Ventana Medical Systems), MET (clone SP44; Ventana), NTRK (clone EPR17341, Abcam), phosphorylated mammalian target of rapamycin (p-mTOR) (clone 49F9; Cell Signaling Technology, Danvers, MA, USA), platelet-derived growth factor alpha (PDGFRA) (rabbit polyclonal; Thermo Fisher Scientific), PDGFRB (clone 28E1; Cell Signaling Technology), programmed death-ligand 1 (PD-L1) (clone E1L3N; Cell Signaling Technology until mid-2018, as of mid-2018 the clone BSR90 from Nordic Biosite, Stockholm, Sweden has been used), progesterone receptor (clone 1E2; Ventana), phosphatase and tensin homolog (PTEN) (clone Y184; Abcam), and ROS1 (clone D4D6; Cell Signaling Technology).
To assess the immunostaining intensity for the antigens EGFR, p-mTOR, PDGFRA, PDGFRB, and PTEN, a combinative semiquantitative score for immunohistochemistry was used. The immunostaining intensity was graded from 0 to 3 (0 = negative, 1 = weak, 2 = moderate, and 3 = strong). To calculate the score, the intensity grade was multiplied by the percentage of corresponding positive cells: (maximum 300) = (% negative × 0) + (% weak × 1) + (% moderate × 2) + (% strong × 3).
The immunohistochemical staining intensity for HER2 was scored from 0 to 3+ (0 = negative, 1+ = negative, 2+ = positive, and 3+ = positive) pursuant to the scoring guidelines of the Dako HercepTestR from the company Agilent Technologies (Agilent Technologies, Vienna, Austria). In case of HER2 2+, a further test with HER2 in situ hybridization was performed to verify the HER2 gene amplification.
Estrogen receptor and progesterone receptor stainings were graded according to the Allred scoring system, from 0 to 8, while MET staining was scored from 0 to 3 (0 = negative, 1 = weak, 2 = moderate, and 3 = strong).
For PD-L1, the tumor proportion score was calculated, which is the percentage of viable malignant cells showing membrane staining.
All antibodies used in this study were validated and approved at the Clinical Institute of Pathology of the Medical University of Vienna, and are typically used in routine IHC staining for clinical purposes.
All tumor specimens of the patients with mPDAC were examined, evaluated, and graded by a single experienced pathologist.
Microsatellite instability analysis
The status of MSI was analyzed by the MSI Analysis System, Version 1.1 (Promega Corporation, Madison, WI, USA) in cases with a loss of MMR protein expression.
Fluorescence in situ hybridization
Fluorescence in situ hybridization (FISH) was applied only in selected cases to verify PTEN loss. FISH was performed with 4-μm-thick formalin-fixed, paraffin-embedded tissue sections. The following FISH probe was utilized: PTEN (10q23.31)/Centromere 10 (ZytoVision, Bremerhaven, Germany). A total of 200 cell nuclei per tumor were evaluated. The PTEN FISH was considered positive for PTEN gene loss with ⩾30% of cells with only one or no PTEN signals. A chromosome 10 centromere FISH probe served as a control for ploidy of chromosome 10.
Multidisciplinary boards (molecular tumor boards for precision medicine)
After thorough examination of the molecular profile of each tumor sample by a qualified and competent molecular pathologist, the results and findings were reviewed in a multidisciplinary tumor board (MTB) meeting held every other week. The online database “MY CANCER GENOME” was used for the discussions in the MTB. 9
Members of the board included molecular pathologists, radiologists, clinical oncologists, and basic scientists. The MTB recommended a targeted therapy based on the specific molecular profile of each patient, based on the prerequisite that all lines of standard therapy were already exhausted in agreement with international guidelines. The targeted therapies included tyrosine kinase inhibitors, checkpoint inhibitors [e.g., anti-programmed death-ligand 1 (PD-L1) monoclonal antibodies], and growth factor receptor antibodies with or without endocrine therapy. The treatment recommendations by the MTB were prioritized, depending on the level of evidence, from high to low according to phase III to phase I trials.
If more than one druggable molecular aberration was identified, the MTB recommended a therapy regimen to target as many molecular aberrations as possible, prioritizing putative driver mutations, with special consideration to the toxicity profile of each antitumoral agent and their potential interactions. Since the majority of patients had already received the available standard treatment options for their cancer disease prior to their inclusion in our platform, nearly all targeted agents were suggested for off-label use. If the tumor profile and the clinical characteristics of a patient met the requirements of a clinical trial for targeted therapies that was conducted in our cancer center, patients were preferentially asked if they wanted to participate in this trial.
Statistical method
The Student’s t test was employed to explore potential gender-specific differences regarding the molecular profile. A p value less than 0.05 was considered statistically significant. For statistical analysis, the software package IBM SPSS Statistics Version 26 was used.
Results
From June 2013 to January 2020, 50 patients diagnosed with therapy-refractory mPDAC were included in this subgroup analysis from our cohort of precision medicine, which has so far profiled over 550 patients with various advanced cancer types without further standard treatment. All patients were of Caucasian origin. The median age at first diagnosis was 58.8 years (range: 23–78 years), and the median age at the time when the molecular profiling was performed was 60.5 years (range: 25–79 years; Table 1). The tumor tissue was obtained from an actual biopsy or during surgical intervention.
Patient characteristics (n = 50).

PDAC, pancreatic ductal adenocarcinoma.
At the time of molecular profiling, all patients had advanced and therapy-refractory mPDAC distant metastases, mainly in the lungs, liver, and peritoneum. Three patients also had bone metastasis, while 14 patients (28%) had undergone a surgical intervention. The patients received a median of two lines of prior systemic chemotherapy, ranging from one to five lines. The chemotherapy regimens included FOLFIRINOX, gemcitabine and nab-paclitaxel, FOLFIRI (folinic acid, fluorouracil, and irinotecan), FOLFOX (folinic acid, fluorouracil, and oxaliplatin), nanoliposomal irinotecan plus fluorouracil, and folinic acid.
In total, we detected 123 mutations in 50 patients. The five most frequent mutations were KRAS (n = 40; 80%), TP53 (n = 29; 58%), CDKN2A (n = 8; 16%), SMAD4 (n = 4; 8%), and NOTCH1 (n = 4; 8%), which accounted for more than half of all mutations (69.1%). BRCA2 mutation was observed in two patients (Tables 2 and 3). A total of 22 patients (44%) were found to have only one mutation, and 13 patients (26%) had more than one mutation. No mutations were found in two patients. Two patients had gene fusions, namely, TBL1XR1–PIK3CA and EIF3E–RSPO2. IHC detected the expression of EGFR, phosphorylated mTOR, and PTEN in 36 (72%), 33 (66%), and 17 patients (34%), respectively. Loss of PTEN was observed in three patients (6%). The median IHC score of EGFR was 200, and 20 patients had high levels of EGFR expression with an EGFR score between 200 and 300. The expression of p-mTOR was intermediate, with a median score of 140; six patients had a high p-mTOR score of 200–300. Expressions of PD-L1 and PDGFRα/β were observed in two patients each, while 3+ HER2 expression and 3+ MET expression were observed in one patient each. Expressions of estrogen receptors and progesterone receptors were seen in one patient. None of the patients were MSI-high. Gene amplification was detected in one tumor specimen that harbored an amplification in ESR1 with a copy number of 18.2.
Genomic profile of the PDAC patients.
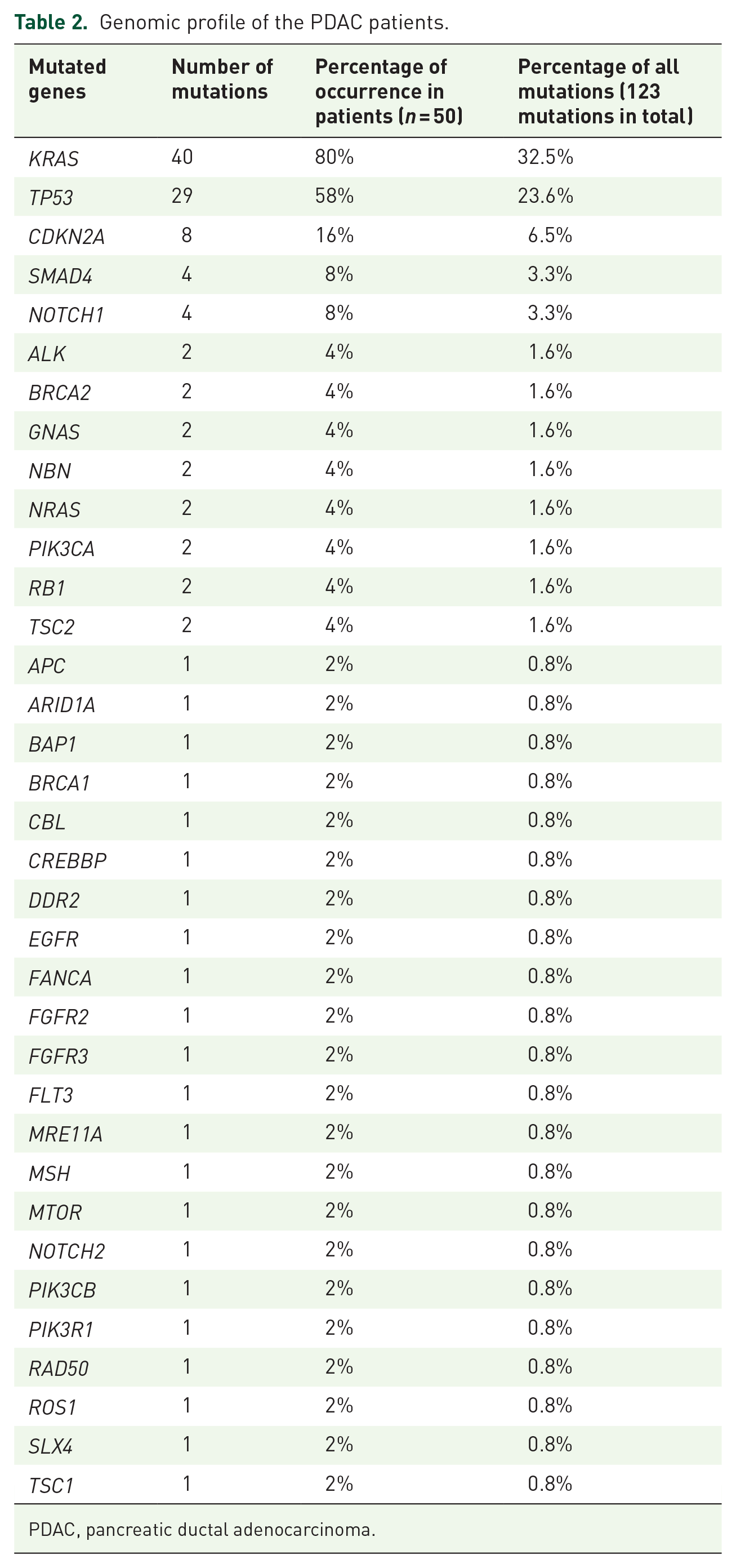
PDAC, pancreatic ductal adenocarcinoma.
Genetic profile of each mPDAC patient (n = 50).
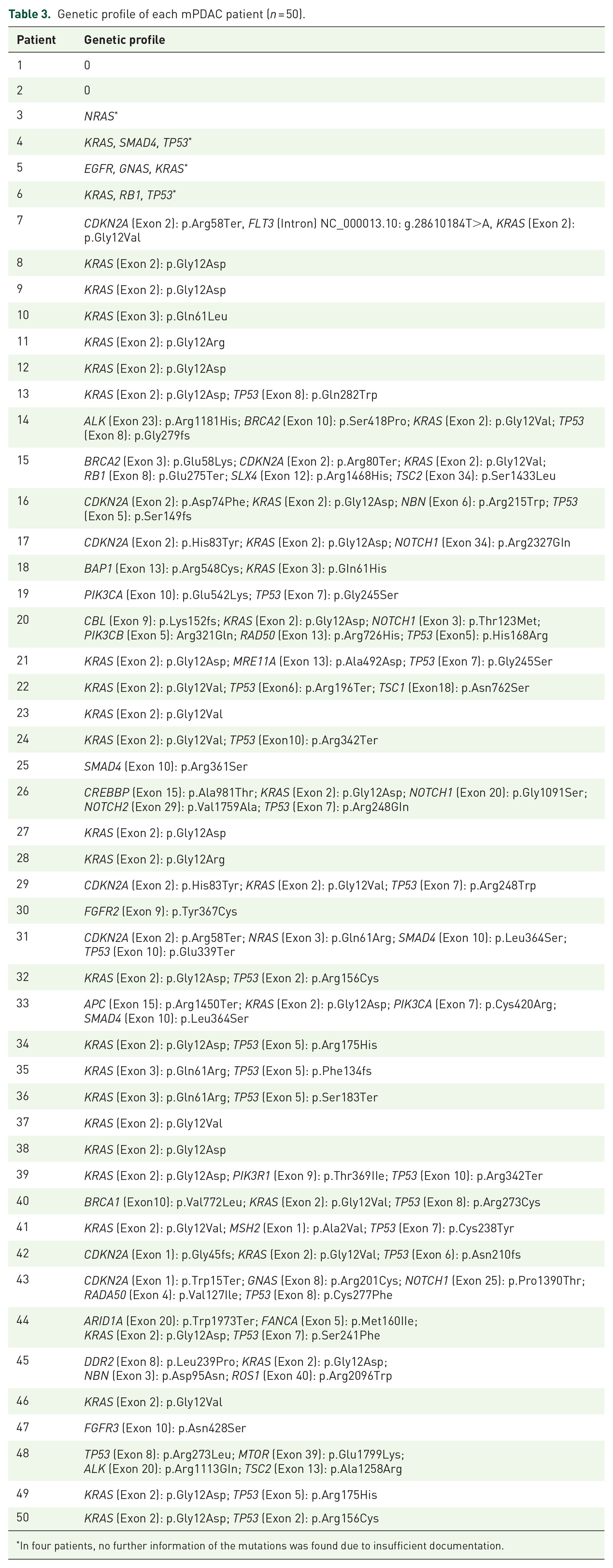
In four patients, no further information of the mutations was found due to insufficient documentation.
In 14 patients, tumor tissue was obtained during surgical resection. The median time interval between initial diagnosis and surgery in resectable tumors was 8.5 weeks, while the median time interval between resection and molecular analysis of the tumor tissue was 15.6 months (range: 6–42 months). A total of 36 patients had a nonresectable tumor at initial diagnosis and underwent biopsy for diagnostic confirmation of PDAC. The median turnaround time between initiation of molecular profiling and discussion in MTB and molecular-based therapy initiation for all 50 patients was 32 and 42 days, respectively.
For 14 (28%) of the 50 patients, including eight men and six women, a targeted therapy was suggested, based on the identified molecular targets. The recommended treatments included the mTOR inhibitor everolimus (n = 3), pembrolizumab (n = 3), nintedanib (n = 2), palbociclib (n = 2), and cetuximab, crizotinib, tamoxifen, and the combination of lapatinib and trastuzumab, each in one patient. See Table 4 for the rationale behind the therapy recommendations.
Rationale for therapy recommendations.

ABL, Abelson murine leukemia viral oncogene homolog 1; ALL, acute lymphatic leukemia; AML, acute myeloid leukemia; BCR, breakpoint cluster region; CML, chronic myeloid leukemia; CRC, colorectal cancer; EGFR, epidermal growth factor receptor; EMA, European Medicines Agency; FDA, Food and Drug Administration; FLT3, FMS-like tyrosine kinase 3; GIST, gastrointestinal stromal tumor; HL, Hodgkin lymphoma; HNSCC, head and neck squamous cell carcinoma; NSCLC, non-small-cell lung carcinoma; PD-1, programmed cell death protein 1; PDAC, pancreatic ductal adenocarcinoma; PDGFR, platelet-derived growth factor receptor; Ph+, Philadelphia chromosome positive; p-mTOR, phosphorylated mammalian target of rapamycin; RCC, renal cell carcinoma; RET, rearranged during transfection; VEGFR, vascular endothelial growth factor receptor.
Finally, 5 of the 14 patients received the recommended therapy. The received therapies included cetuximab, crizotinib, everolimus, nintedanib, and trastuzumab in combination with lapatinib.
Four patients died due to disease progression, receiving the therapy prior to radiological assessment of treatment efficacy. One patient was treated with nintedanib and achieved stable disease for 6 months. Eight patients did not receive the therapy suggested by the MTB. In two cases, the responsible oncologist opted for another treatment. Six patients died or their health condition deteriorated before the targeted therapy could be initiated.
The application of the Student’s t test did not detect any significant gender-specific differences regarding the expression of mTOR (p = 0.157), EGFR (p = 0.541), and PTEN (p = 0.979), or in the number of mutations (p = 0.933).
Discussion
In this retrospective analysis of our platform for precision medicine at the Medical University of Vienna, we described real-life clinical data of 50 patients diagnosed with therapy-refractory mPDAC with no further standard treatment option. For 14 patients, a targeted therapy was offered. Although our study demonstrated that precision medicine can be implemented and integrated into clinical practice, only one patient had a clinical benefit from the personalized treatment approach. One important reason for the poor outcome may be the long median turnaround time of 42 days between molecular profiling and therapy initiation. Thus, during this time interval, six patients died or their condition worsened before therapy initiation. Another reason is that mPDAC is a devastating cancer disease that grows aggressively. Without a potent antitumoral therapy, tumor growth cannot be controlled, and when the tailored therapy is initiated with delay, it fails to hinder the progress of the cancer disease. Thus, four patients died during the course of the personalized therapy prior to radiological assessment. These data show that it is crucial to reduce the turnaround time between molecular profiling and therapy initiation, particularly for a devastating and aggressive cancer disease like mPDAC. Solutions for this challenge include the development and employment of modern automated techniques and algorithms for a faster molecular analysis and removal of cumbersome bureaucratic obstacles for the acquirement of the needed targeted drug. An important limitation of this study is that the median time interval between resection and molecular analysis of the tumor tissue was 15.6 months (range: 6–42 months). This means that the molecular profile may had evolved in this time interval. A growing body of evidence suggests that even systemic antitumoral therapy can drive and inform the clonal and molecular evolution of PDAC. 10 Liquid biopsy may help in the future to detect the molecular aberrations and alterations in real-time to tailor a targeted therapy that matches the current molecular landscape. Findings by liquid biopsy may also be translated into the development of new biomarkers to enable molecular therapy monitoring and to detect relapse at an earlier stage than conventional imaging techniques.11,12 Our study suggests that molecular profiling should be performed prior to failure of the last line of standard treatment options to potentially drive late-line treatment decisions without treatment delays.
Based on an informative molecular profile, we recommended a precision treatment in 28% of our patients. Five patients (10%) received the targeted therapy. A similar study conducted by Pishvaian et al. in the Unites States (US) performed molecular profiling on tumor samples from over 600 patients. The researchers detected highly actionable genomic alterations and actionable proteomic alterations in 27% and 5% of the patients, respectively. From over 600 patients, only 17 (2.8%) received a targeted therapy. Unlike Pishvaian et al., we conducted this study exclusively in patients with therapy-refractory mPDAC with no further standard treatment options available. 13
The five most frequent mutations in this study were observed in KRAS, TP53, CDKN2A, SMAD4, and NOTCH1. This finding is in keeping with a growing body of literature that has identified genetic aberrations in KRAS, CDKN2A, TP53, and SMAD4 as the major and most common driver mutations in pancreatic carcinogenesis.14–16
When it comes to the application of targeted therapies in mPDAC, several unique and distinct features of this cancer disease should be taken into consideration. PDAC exhibits remarkable intra- and intertumoral heterogeneity and diversity on several levels, including the genetic, epigenetic, proteomic, and metabolomic levels.17–19 Further, the unique tumor microenvironment (TME) of PDAC is informed by an abundant and dense desmoplastic stroma produced and maintained by pancreatic stellate cells (PSCs). The dense stroma builds a barrier that results in hypovascularity and builds up a hypoxic and acidic environment that impedes and limits drug delivery. Several cell types, including myeloid-derived suppressor cells (MDSCs), tumor-associated macrophages (TAMs), regulatory T cells (Tregs), cancer-associated fibroblasts, and mast cells, create a highly immunosuppressive milieu that inhibits antitumor immune response. These multiple factors render pancreatic cancer cell therapy resistant and immunoevasive.20,21
For three patients, we recommended mTOR inhibitor everolimus with strong p-mTOR expression and loss of PTEN. PIK3CA was mutated in two patients. One patient harbored a mutation in PIK3CB and TP53. Previous studies suggest that patients with PTEN deficiency and mutations in the PIK3CA may benefit from the application of an mTOR inhibitor.22,23 As evidenced by Utomo et al., a subpopulation of patients with PDAC showed a strong activation of the mTOR signaling pathway with increased sensitivity to rapamycin in ex vivo analysis. 24 In their important study, Morran et al. investigated mTOR dependency in mice and in mouse PDAC cell lines, and stated that mTOR inhibition may lead to proliferative arrest and even tumor regression in pancreatic tumors driven by activated KRAS and PTEN deficiency, but not in tumors driven by activated KRAS and mutant p53. 23 Later, this finding was confirmed by Hassan et al. and Driscoll et al., who reported that mTORC2 inhibition resulted in delayed tumorigenesis, and that combined mTORC1/2 and PI3K inhibition significantly increased survival in mice with PDAC.25,26 However, these studies are limited by the fact that they were conducted only in mice.
The humanized antibody pembrolizumab targets the PD-1 receptor of lymphocytes. It was offered as a targeted therapy for three patients, two of whom had high levels of PD-L1 expression of around 50%. In a meta-analysis, Gao et al. stated that the PD-L1 expression rate in PDAC ranged from 19% to 62.5%, and may be a marker for reduced overall survival. 27 A phase I trial by Brahmer et al. showed that the PD-L1 antibody BMS-936559 did not result in objective responses in patients with colorectal or pancreatic cancer. 28 However, in this trial, patients were not stratified based on their PD-L1 expression. Further, in May 2017, the Food and Drug Administration (FDA) took an unprecedented step and approved pembrolizumab for adult and pediatric patients with unresectable or metastatic, microsatellite instability-high, or mismatch repair-deficient solid tumors, regardless of tumor site or histology. 29 This was the first tissue-agnostic FDA approval for a drug. According to the latest American Society of Clinical Oncology (ASCO) guidelines, pembrolizumab is recommended as a second-line therapy for the treatment of pancreatic cancer patients with mismatch repair-deficient or microsatellite instability-high tumors. 30
The majority of ARID1A mutations are inactivating mutations and lead to loss of ARID1A deficiency. 31 The one patient with ARID1A mutation was offered pembrolizumab based on a groundbreaking research article by Shen et al. that showed the interaction of ARID1A with mismatch repair (MMR) protein MSH2. 32 The authors observed that treatment with anti-PD-L1 antibody reduced the tumor burden and prolonged the survival of mice bearing ARID1A-deficient but not ARID1A wild-type ovarian tumors. Thus, they concluded that ARID1A deficiency potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. 32
For the two patients with CDKN2A mutation, the cyclin-dependent kinase (CDK) inhibitor palbociclib was suggested by the MTB. A research work by Young et al. showed that mutations of the CDKN2A gene in melanoma cell lines predicted sensitivity to the CDK4/6 inhibitor palbociclib. 33 However, our recommendations were made prior to the publication of the results from the TAPUR study that showed that single-agent palbociclib has no meaningful clinical activity in patients with CDKN2A-mutated or -deleted advanced pancreatic cancer and cholangiocarcinoma. 34
Nintedanib is a multi-targeted tyrosine kinase inhibitor that was suggested for two patients with high levels of PDGFRα/β expression. Furthermore, one of them had an FGFR2 mutation and the other harbored an FLT3 mutation. The recommendation of nintedanib was based on a research article by Awasthi et al. that showed the strong antitumor activity of nintedanib – particularly in combination with gemcitabine – in experimental PDAC. 35
We suggested lapatinib combined with trastuzumab for one patient with a high HER2 expression of 3+. In a phase II study, lapatinib was applied in conjunction with capecitabine in second-line treatment for mPDAC. Of 17 patients, 6 experienced progressive disease afterwards, and another 6 achieved stable disease. The authors noted that patients with stable disease had a significantly better clinical outcome in terms of progression-free survival (PFS) and overall survival (OS) than patients with progressive disease. 36
The anti-EGFR monoclonal antibody cetuximab in combination with gemcitabine was suggested for one patient with a high EGFR expression score of 300 and KRAS wild type.
Our recommendation was derived from an important phase II trial by Xiong et al. that tested cetuximab combined with gemcitabine only in pancreatic cancer patients with at least 1+ EGFR staining. This combination therapy regimen achieved a disease control rate of approximately 75%. 37 A clinical phase III trial by Philip et al. comparing gemcitabine plus cetuximab versus gemcitabine monotherapy in PDAC patients concluded that cetuximab did not improve the outcome compared with patients treated with gemcitabine alone. 38 However, the major limitation of this trial was that patients were neither screened for EGFR expression nor for oncogenic mutations in KRAS. Notably, the KRAS status of malignancies is of the utmost importance when it comes to the efficacy of EGFR antibodies. It has been observed that certain mutations, particularly in KRAS exon 2, may confer resistance to cancer cells in different entities against cetuximab.39–42
Tamoxifen was suggested for one patient with a strong expression of estrogen receptors based on a phase II trial by Tamao et al. 43 One patient with MET and ALK expression was offered crizotinib on the basis of a research work done by Yan et al. 44
Taken together, the management of mPDAC poses several major challenges, including the long turnaround time until therapy initiation, the extreme intra- and intertumoral molecular heterogeneity of PDAC, and the complex immunosuppressive, hypovascular, acidic, and hypoxic tumor microenvironment. Further research is warranted for a better comprehension of the complex tumor biology.
This study has several limitations. First, this is a non-randomized, retrospective sub-analysis of our cohort for precision medicine. Second, the studied 50 patients were not compared with an adequate control group. Further, the analysis may be somewhat biased due to the good performance status of the patients at the time of molecular analysis.
However, for all we know, this is the first study that shows – based on real-life data – the feasibility, potentials, and challenges of precision medicine in therapy-refractory mPDAC patients. Based on our observations, it is of major importance that a molecular tumor portrait is created prior to failure of the last line of standard treatment options to potentially drive late-line treatment decisions without treatment delay.
Our study supports further clinical trials, studies, and research works for the development and implementation of molecular-guided treatment approaches in the therapeutic management of PDAC patients.
Supplemental Material
Supplemental material for Applied precision medicine in metastatic pancreatic ductal adenocarcinoma
Supplemental material, supplemental_material for Applied precision medicine in metastatic pancreatic ductal adenocarcinoma by Hossein Taghizadeh, Leonhard Müllauer, Robert M. Mader, Martin Schindl and Gerald W. Prager in Therapeutic Advances in Medical Oncology
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.