
Abstract
Background:
Immunotherapy combined with platinum-based chemotherapy is now the standard first-line treatment for non-small cell lung cancer (NSCLC) patients. However, limited evidence exists to show the efficacy of immunotherapy plus taxanes for patients who have progressed after platinum-based chemotherapy.
Methods:
The immunotherapy naïve patients with metastatic NSCLC who received anti-PD-1/PD-L1 monotherapy or combined with nab-paclitaxel after prior platinum-based chemotherapy from 2015 to 2018 in PLA General Hospital were identified. The progression-free survival, overall survival (OS), objective response rate (ORR), disease control rate (DCR) and safety were assessed.
Results:
Of 57 patients, 40 were treated with anti-PD-1/PD-L1 monotherapy and 17 were treated with anti-PD-1/PD-L1 plus nab-paclitaxel. With a median OS follow-up of 16.3 months, the nab-paclitaxel group showed significantly longer OS compared with the immune monotherapy group (median, 28.6 months versus 15.9 months, log-rank p = 0.020). When adjusted by covariates in COX proportional regression model, both the treatment group [p = 0.009, hazard ratio (HR) 0.361; 95% confidence interval (CI) 0.168–0.773] and performance status (p = 0.003, HR 0.372; 95% CI 0.192–0.721) demonstrated independent association with the longer OS from combination therapy. In addition, ORR was 23.5% (4/17) in the immune checkpoints inhibitors (ICIs) plus nab-paclitaxel group versus 13.5% (5/37) in immune monotherapy group (p = 0.439), with a DCR of 88.2% (15/17) and 59.5% (22/37) (p = 0.034), respectively. The incidence of grade 3/4 adverse events was 23.5% (4/17) in the combination group and 2.5% (1/40) in the immune monotherapy group.
Conclusion:
PD-1/PD-L1 inhibitor plus nab-paclitaxel resulted in significantly longer OS and higher response versus ICI single agent in metastatic NSCLC patients who have progressed after platinum-based chemotherapy. These findings need to be further explored by prospective studies.
Introduction
Immune checkpoints inhibitors (ICIs), including anti-programmed cell death protein 1 (PD-1) or anti-PD-1 ligand (PD-L1) monoclonal antibodies, have shown promising efficacy in the treatment of non-small cell lung cancer (NSCLC).1–8 Despite significantly prolonged overall survival in patients with NSCLC, only a small subset of patients could achieve benefit from ICIs monotherapy.9,10 Therefore, various combination strategies are being designed to enhance and broaden the clinical benefits of immunotherapy.
Numerous clinical trials are ongoing to investigate the efficacy of ICIs combined with other treatments in NSCLC, including chemotherapy, anti-angiogenesis and other novel agents which may activate tumor immunogenicity. Accumulating evidence indicates that chemotherapy could not only induce apoptosis of cancer cells, but also immediate immunogenic effects including the upregulation of the expression of PD-L1 and major histocompatibility complex (MHC) class I, activation of nuclear factor-κB (NF-κB) signaling and modulation of the tumor infiltrating lymphocytes.11–14 Vascular endothelial growth factors involved in the angiogenesis were also considered as a mediator of the immune response from multiple aspects, including promoting the suppressive immune related cells subpopulation, such as T regulatory cells and myeloid-derived suppressor cells, inhibiting the maturation of dendritic cells that present tumor-associated antigen and suppressing T cell infiltration due to abnormal tumor vasculature.15–18 Taken together, this evidence provided rationale to combine chemotherapy and/or anti-angiogenesis therapy with immunotherapy to exert a synergistic effect and maximize the benefit of immunotherapy.
Several studies have clearly demonstrated that the addition of PD-1/PD-L1 inhibitor to standard platinum-based chemotherapy with or without anti-angiogenesis therapy could exert a synergistic effect in patients with chemotherapy-naïve NSCLC, providing a better objective response rate (ORR) and improved clinical outcomes.1,7,19–22 Immunotherapy combined with platinum-based therapy with or without anti-angiogenesis therapy are now standard first-line treatment options for patients with NSCLC, including platinum-pemetrexed plus pembrolizumab or carboplatin/paclitaxel/bevacizumab plus atezolizumab for non-squamous NSCLC, and platinum-paclitaxel/nab-paxlitaxel plus pembrolizumab for squamous NSCLC. However, for patients who have progressed after platinum-based chemotherapy or who are not candidates for platinum drugs, the rational partner to immunotherapy has not been defined.
Taxanes play a central role in the management of advanced NSCLC and single agent taxane is standard treatment of patients with metastatic NSCLC.23–27 Taxanes may have pleiotropic immune-modulating effects, including promoting the maturation of dendritic cells and enhancing the secretion of proinflammatory cytokine.28,29 Nab-paclitaxel (albumin-bound paclitaxel), a form of paclitaxel formulated without the use of solvent, was also considered as a potential partner with ICIs.30,31 The phase 3 randomized controlled trial IMpassion 130 revealed the prolonged progression-free survival (PFS) among patients with metastatic triple-negative breast cancer treated with atezolizumab plus nab-paclitaxel compared with patients who received placebo plus nab-paclitaxel (7.2 months versus 5.5 months; hazard ratio 0.8; p = 0.002). 32
However, investigations of ICIs plus nab-paclitaxel for NSCLC patients with prior platinum-based chemotherapy is limited. Therefore, we conducted this retrospective analysis to investigate the efficacy and safety of ICIs combined with nab-paclitaxel for patients with metastatic NSCLC who have progressed after platinum-based chemotherapy.
Methods
Patients
Patients with metastatic NSCLC who received immunotherapy at General Hospital of the People’s Liberation Army (PLA General Hospital) were screened between March 2015 and June 2018 (Supplemental material Figure S1 online). The inclusion criteria were: (a) patients with histological confirmed stage IV NSCLC; (b) treated with ICI monotherapy or ICI plus nab-paclitaxel after progression with platinum-based chemotherapy as the metastatic-setting treatment; (c) immunotherapy naïve; (d) any ECOG PS status. The exclusion criteria were: (a) patients who received PD-1/PD-L1 inhibitors as first-line therapy; (b) patients with PD-1/PD-L1 inhibitors in combination with therapies other than nab-paclitaxel; (c) patients who never received platinum-based chemotherapy. Drugs were given according to the instructions. The Ethics Committee of PLA General Hospital approved the study (S2018-141-01) and written informed consent (including the description of the study, risks and discomforts, benefits, confidentiality, etc.) was provided by all patients, which was in accordance with the Declaration of Helsinki.
Study objectives
The objectives of this analysis were to assess the impact of ICI plus nab-paclitaxel on patient PFS, overall survival (OS), ORR, disease control rate (DCR) and safety profile. PFS was defined as the interval between the initiation of treatment and disease progression, death from any cause, or last follow-up visit. OS was defined as the interval between the initiation of treatment and death from any cause or last follow-up visit. The tumor response was evaluated according to the Response Evaluation Criteria in Solid Tumor (RECIST, version 1.1) as a complete response, partial response, progressive disease or stable disease. Adverse events were graded per the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.
Statistical analysis
Chi-square or Fisher’s exact test were used to compare categorical variables. PFS and OS were analyzed using the Kaplan–Meier method and comparisons between different groups were assessed using a stratified log-rank test and/or a Gehan–Breslow–Wilcoxon test, which were intended to assess the differences at later or earlier time points, respectively. Cox proportional multivariable model was used to assess independent predictive factors associated with PFS or OS. Variables with p ⩽ 0.05 or that might have an important effect on prognosis were included into multivariable models. Data were analyzed using GraphPad Prism (version 7.01, GraphPad Software, USA) and SPSS statistical software (version 20.0, SPSS, IBM Corporation, USA). A two-sided p value <0.05 was considered statistically significant.
Results
Patient characteristics and treatment
From March 2015 to June 2018, a total of 89 patients receiving ICIs therapy in PLA General Hospital were screened. A total of 57 patients were included in this analysis (40 patients in the ICI monotherapy group and 17 in the ICI plus nab-paclitaxel group) based on the inclusion and exclusion criteria (supplemental Figure S1). Overall, the baseline characteristics of the patients were generally balanced between the two groups, except for a higher ratio of male patients in the ICI plus nab-paclitaxel group (82.4% versus 77.5%, p = 0.000) (Table 1). Moreover, the proportion of patients with brain metastasis was higher in the ICI plus nab-paclitaxel group (41.2% versus 25.0%) despite no significant difference.
Demographics and baseline characteristics.
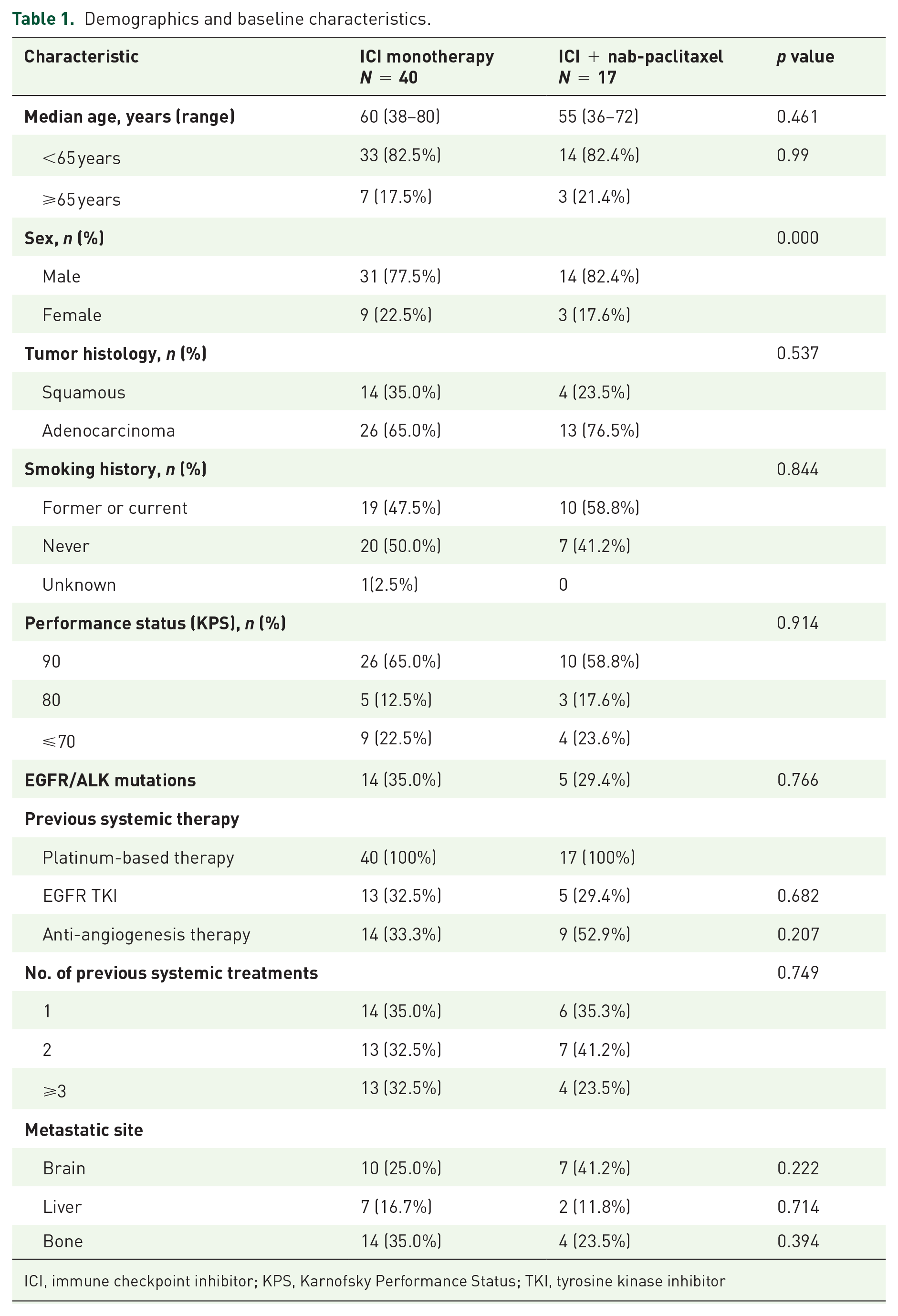
ICI, immune checkpoint inhibitor; KPS, Karnofsky Performance Status; TKI, tyrosine kinase inhibitor
Efficacy
At the time of data analysis, the median OS follow-up was 16.3 months in the total population. A trend of longer PFS was observed in the patients from the ICI plus nab-paclitaxel group than in the ICI monotherapy group [median, 7.5 months versus 3.7 months; hazard ratio (HR), 0.70; 95% confidence interval (CI), 0.38–1.27; Gehan–Breslow–Wilcoxon p = 0.049; Figure 1(A)], indicating the significantly longer PFS from the adding of chemotherapy at early time points. Patients treated with ICI plus nab-paclitaxel had significantly prolonged OS versus ICI monotherapy (median, 28.6 months versus 15.9 months; HR 0.42, 95% CI 0.20–0.89, log-rank p = 0.020, Figure 1(B)). In a multivariable model including the Karnofsky Performance Status (KPS) and treatment group, the treatment of ICI plus nab-paclitaxel (HR, 0.361; 95% CI 0.168–0.773; p = 0.009) and a KPS of 90 (HR, 0.372; 95% CI 0.192–0.721; p = 0.003) remained independent indictors for superior OS (Table 2). For most subgroups, the difference was not statistically significant, but the data also indicated a trend of PFS (supplemental Figure S2) and OS (supplemental Figure S3) benefit towards the combination treatment strategy.

Patient survival. Kaplan–Meier survival curves comparing the progression-free survival (A) and overall survival (B) between anti-PD-1/PD-L1 monotherapy and anti-PD-1/PD-L1 plus nab-paclitaxel therapy.
Univariable and multivariable analysis of progression-free survival and overall survival.

Gehan–Breslow–Wilcoxon p adopted. The log-rank p value for progression-free survival was 0.241.
CI, confidence interval; HR, hazard ratio; KPS, Karnofsky Performance Status; LDH, lactate dehydrogenase
The rate of objective response was 13.5% in the ICI monotherapy group and 23.5% in the ICI plus nab-paclitaxel group (Table 3). No patients had a complete response. The disease control rate was 59.5% in the ICI monotherapy group as compared with 88.2% in the ICI plus nab-paclitaxel group. Best objective response for all patients is depicted in supplemental Figure S4.
Responses assessed per RECIST version 1.1.

CI, confidence interval; ICI, immune checkpoint inhibitor; RECIST, Response Evaluation Criteria in Solid Tumor
As shown in Figure 2(A) and (B), a 53-year-old male patient #1 Y1285984 with lung adenocarcinoma was treated with nivolumab 200

Computed tomography images showing the response to nab-paclitaxel combination therapy in two patients. Compared with lung lesions at baseline on 4 June 2015 (A), (B) shows a significant decrease in the size of lung lesions (24 August 2015) in patient #1 Y1285984 treated with nivolumab plus nab-paclitaxel. Compared with lung lesions on 28 May 2016 (C), adrenal gland on 1 July 2016 (D) and mediastinal lymph nodes on 1 July 2016 (E) at baseline, (F, G and H) show significant decreases in the size of metastatic lesions in another 53-year old male patient, Y1881072, treated with nivolumab plus nab-paclitaxel.
Adverse events
Adverse events of any grade occurred in 12 of 17 patients (70.6%) who received ICI plus nab-paclitaxel and in 28 of 40 patients (70.0%) who received ICI monotherapy (Table 4). Incidence of grade 3–4 treatment-related adverse events was higher in those treated with ICI plus nab-paclitaxel [4 (23.5%) of 17 patients] than in those treated with ICI monotherapy [1 (2.5%) of 40 patients]. The grade 3–4 treatment-related adverse events in ICI plus nab-paclitaxel group were pneumonitis [three (17.6%)], fever [two (11.8%)], fatigue [one (5.9%)] and neutropenia [one (5.9%)]. The grade 3–4 treatment-related adverse events in ICI monotherapy group were nausea [one (2.5%)]. There were no treatment-related deaths.
Adverse events.

Discussion
In this study, we observed that the combination of ICI and nab-paclitaxel was associated with significantly improved OS among patients with metastatic NSCLC who have progressed after platinum-based chemotherapy. This represents the first retrospective study to date evaluating the efficacy of immunotherapy plus nab-paclitaxel in this patient population. In addition, we identified a higher incidence of adverse events in patients receiving ICI plus nab-paclitaxel compared with patients receiving ICI monotherapy. Nevertheless, most of the adverse events were manageable.
Previous studies have shown that PD-1/PD-L1 inhibitor monotherapy has an ORR range from 14% to 24% and median PFS range from 1.9 months to 3.9 months as second-line or later therapy in unselected patients with NSCLC.2–4,6,33–35 In our study, the ORR in ICI monotherapy group was 12.8% and the median PFS was 3.7 months, which seemed to be consistent with previous results.
Several trials that evaluated the efficacy of anti-PD-1/anti-PD-L1 plus platinum-based chemotherapy in the NSCLC population revealed an ORR of 49.0–57.9%, with median PFS of 6.3–6.4 months in squamous NSCLC,19,36 and an ORR of 47.6–63.5%, with median PFS of 8.3–13.0 months in non-squamous NSCLC.1,7,20
Nab-paclitaxel was reported to be effective as first-line therapy for NSCLC regardless of whether being used as single-agent or combined with platinum drugs. One phase II multicenter study demonstrated an ORR of 16%, with a median PFS of 6 months in patients with NSCLC who received single-agent nab-paclitaxel q3w as first-line therapy. 23 In addition, 67% of the patients in this trial were squamous NSCLC. Another phase I/II phase study suggested that weekly single-agent nab-paclitaxel was also effective in patients with chemotherapy-naïve advanced NSCLC, with an ORR of 30% and a median PFS of 5 months. 37 A phase III study indicated that nab-paclitaxel plus carboplatin has a significantly higher ORR (33% versus 25%, p = 0.005) compared with solvent-based paclitaxel plus carboplatin as first-line therapy for advanced NSCLC, although without a significant PFS improvement in the total population (6.3 m versus 5.8 m, p = 0.214). 38 Nab-paclitaxel is also a satisfactory treatment option for patients with refractory NSCLC who have progressed after progression on platinum-based chemotherapy. In several phase II trials on patients with refractory NSCLC after progression to platinum-based chemotherapy, nab-paclitaxel demonstrated an ORR of 19–32%, with a median PFS of 4.5–4.9 months.39–41 In our study, ICI plus nab-paclitaxel demonstrated encouraging efficacy in 17 patients who have progressed after platinum-based chemotherapy, with an ORR of 23.5% (95% CI 8.5–46.0), including four who reached partial response, a median PFS of 7.5 months, and a median OS of 28.6 months. A majority (64.7%) of the patients were treated as third line or later therapy, further suggesting that nab-paclitaxel might be an effective partner to immunotherapy.
Despite the refractory features of patients included in our study, the survival status was encouraging in patients received ICI plus nab-paclitaxel. Previous clinical trials indicated that patients with squamous NSCLC who received first-line treatment exhibited inferior clinical outcome compared with patients with other NSCLC subtypes.42–44 In our study, 31.6% of the total population (18 out of 57) and 23.5% (4 out of 17) of the ICI plus nab-paclitaxel group were squamous NSCLC. Furthermore, 81% of the total population and 82% of the ICI plus nab-paclitaxel group were younger patients (<65 years old). The high proportion of non-squamous NSCLC and younger patients included in our study may contribute to the superior OS benefit (HR, 0.42; 95% CI 0.20–0.89; p = 0.020) from combination therapy.
The incidence of grade 3–4 adverse events was 73% in IMpower 131 and the incidence of grade 3–5 adverse events was 69.8% in Keynote-407.19,36 The chemotherapy regimen was platinum-based in these two clinical trials, which might contribute to the higher incidence of grade 3–4 adverse events. In the present study, although the incidence of grade 3–4 adverse events was higher in the ICI plus nab-paclitaxel group (23.5% versus 2.5%), most of the adverse events were manageable. No death occurred due to treatment-related adverse events.
There are several limitations in this study. First, the limited sample size and the retrospective nature might contribute to the unavoidable bias and compromise the evidence level. The baseline characteristics were also imbalanced between the two groups, with a higher proportion of male patients in the ICI plus nab-paclitaxel group. Nevertheless, sex was not an independent indicator for PFS or OS in the univariable and multivariable analysis. Second, the assessment of PD-L1 expression is not mandatory for the majority of the studied patients, and thus was not included into analysis, which may lead to potential bias. In addition, there is a lack of chemotherapy-only group. Further investigations are warranted to explore the synergy effects of the combination therapy.
In conclusion, we observed that PD-1/PD-L1 inhibitor plus nab-paclitaxel was associated with significantly longer OS and higher response with tolerable safety compared with single agent ICI as second line therapy or higher in metastatic, refractory NSCLC patients with prior platinum-based therapy. These findings need to be further explored by prospective studies.
Supplemental Material
Supplementary_material_v2 – Supplemental material for Efficacy and safety of PD-1/PD-L1 inhibitors plus nab-paclitaxel for patients with non-small cell lung cancer who have progressed after platinum-based chemotherapy
Supplemental material, Supplementary_material_v2 for Efficacy and safety of PD-1/PD-L1 inhibitors plus nab-paclitaxel for patients with non-small cell lung cancer who have progressed after platinum-based chemotherapy by Fan Zhang, Di Huang, Lei Zhao, Tao Li, Sujie Zhang, Guoqing Zhang, Fang Yuan, Jie Zhang, Yuzi Zhang, Zhengyi Zhao, Longgang Cui, Jing Zhao, Guoqiang Wang, Shangli Cai, Yuezong Bai, Jinliang Wang and Yi Hu in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to thank all the patients in this study.
Authors’ note
Yuzi Zhang, Jing Zhao, Guoqiang Wang and Shangli Cai are currently affiliated with Burning Rock Biotech Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by grants from the National Natural Science Foundation of China (81672996 to Yi Hu, 81402552 to Fan Zhang, and 81770204 to Lei Zhao), The Young Talent Program of PLA General Hospital and the Young Talent Foundation of PLA General Hospital (2018XXFC-3,2019XXJSYX03 to Fan Zhang; 2018XXFC-11,2019XXJSYX11 to Lei Zhao), The Big Data Project of PLA General Hospital (to Lei Zhao), Major projects of the ministry of science and technology during the 13th five-year plan period (2018ZX09201013 to Guoqing Zhang), National Key R&D Program of China, Stem Cell and Translation Research (2017YFA0106200 to Fang Yuan).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.